IFHC Encounter Data Entry Form HEALTH CENTER # CLIENT
advertisement

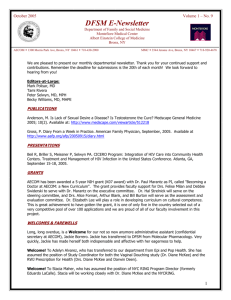
IFHC Encounter Data Entry Form HEALTH CENTER # SERVICES PROVIDED (check all applicable) CLIENT NUMBER # DATE OF VISIT / / 2013 FIPS CODE RACE (check all that apply) 1. White 5. Unknown/Not Reported 2. Black 7. Native Hawaiian/Pacific Islander 3. American Indian/Alaska Native 4. Asian ETHNIC ORIGIN - Hispanic Yes No Unknown INTERPRETER/BILINGUAL STAFF NEEDED 1. Yes 2. No GENDER (check one) Female Male PREGNANCY HISTORY (female only) a. Number of previous pregnancies: ___________ b. Number of live births: ___________________ d. Age at first pregnancy: __________________ e. Age at first live birth: ___________________ f. Last pregnancy ended (mo./yr.): ____ / _____ mm YYYY PREGNANCY DESIRED WITHIN 1 YEAR? Yes No EMPLOYMENT STATUS 1. Employed – Full Time 2. Employed – Part Time 3. Unemployed 4. Not Seeking Work CURRENTLY IN SCHOOL? Yes No EDUCATIONAL LEVEL (last grade completed) 1. Grade 1-8 2. Grade 9-12 3. GED/HS Diploma 4. Grad. School 17-20 5. Undergrad/Tech School 13-16 6. Unknown/None PURPOSE OF VISIT (check one) 1. Initial Comprehensive 2. Annual Comprehensive 9. Other Comprehensive 8. Medical Problem 6. Post Partum DATE OF BIRTH / INCOME AND FAMILY SIZE 5. Deferred 3. Routine Medical 4. Education/Counseling 7. Emergency Contraception / Monthly Family Income? ___________ Family Size? _______________ PRIMARY SOURCE OF PAYMENT (check one) 1. Medicaid Only 2. No Fee 3. Partial Fee 4. Full Fee 6. Private Insurance 8. ADV 9. Other 10. CHIP INSURANCE (check one) 1. Private w/BC coverage 2. Private w/o BC coverage 3. Medicaid/Public 4. Private/ BC coverage Unknown 5. Uninsured 6. Unknown 01. Blood Pressure 30. Wet Mount 02. Height/Weight 64. HSV Test 03. Thyroid Palp 63. Urine Pregnancy Test 04. Heart/Lung Aus 43. Negative Preg. Test 05. Breast Exam 44. Positive Preg. Test 06. Abdominal Palp 67. Contraceptive Injection 07. Extremities 57. IUD Insert 08. Bimanual Pelvic 58. IUD Removal 09. Speculum Exam 89. HPV vaccine 11. Female External Genitalia 34. Other Lab or Exam 10. Male Genitalia 45. Treatment: Gonorrhea 18. Post Abortion Check 50. Treatment: Chlamydia 19. Postpartum Check 61. Treatment: Cervicitis 20. Hgb 46. Treatment: PID 22. HIV Test 52. Treatment: Wart 88. HIV WB Results Given 62. Treatment: HSV 23. Syphilis Test 49. Treatment: Vaginitis 24. Urine Dipstick 66. Treatment: UTI 25. Pap Smear 72. Treatment: Anemia 26. Repeat Pap Smear 95. Treatment: Urethritis 28. Gonorrhea/CT Test COUNSELING EDUCATION PROVIDED (check all applicable) 01. Contraceptive 18. HIV Post Test 02. NFP 11. Other 04. Infertility 19. Exercise/Nutrition 05. Smoking/Tobacco 13. Abstinence 06. Alcohol/Drug Abuse 15. Crisis 07. Pregnancy 16. Abnormal Pap 08. PCC/Folic Acid 17. Domestic Violence 09. STD/HIV Prevention 20. SBE 10. HIV Pre Test 21. Adolescent Counseling BMI BMI EDUCATION? 1. <18.5 4. 30-39.9 YES 2. 18.5-24.9 5. 40 and above NO 3. 25-29.9 CIGS/DAY SERVICE PROVIDER 1. <5 5. NONE 1. Physician 2. 5-10 2. PA, NP, CNM 3. 11-20 3. Other Clinical Staff 4. >20 4. Non-Clinical Staff CONTRACEPTIVE METHOD 15. Abstinence 02. IUD 09. Sterilization 05. Condom 07. Natural Method 19. Vaginal Ring 14. Depo Provera Inj 13. None 20. Vasectomy 03. Diaphragm 11. Other 21. Female Condom 16. ECP 18. Patch 01. Oral 06. Spermicide 04. Foam & Condom 10. Sponge 12. Hormone Implant CONT. BEFORE:______ CONT. AFTER: ______ WHY NO METHOD? 1. Pregnancy Planned 4. Other Medical Reason 9. Pregnancy Unplanned 6. Other 2. Infertility 8. Refused 3. Seeking Pregnancy CONDOMS: Yes No ECP FUTURE USE: Yes No REFERRALS (check all applicable) 01. Sterilization 15. Mammogram 02. Gynecology 08. Other Medical 03. Prenatal 05. Social Services 16. Abortion 11. Nutrition 06. Contraception 12. Other 10. Infertility 17. Breast 07. STD 18. Adoption 14. HIV HIV RESULTS HIV WB F/U RESULTS 1. Negative 1. Confirmed Pos 2. Invalid 2. Confirmed Neg 3. Prel + Serum WB 3. Indeterminate 4. Prel + OraSure 5. Pending IFHC 4/29/11, rev. 9/11, 1/12, 1/13 IFHC Encounter Data Entry Form IFHC 4/29/11, rev. 9/11, 1/12, 1/13