Colleagues- Please find the latest draft of my proposal for ESCape
advertisement

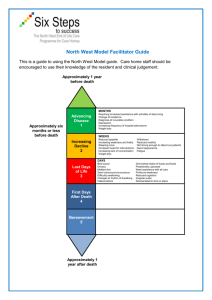
ColleaguesPlease find the latest draft of my proposal for ESCape tomorrow. I am sorry for this being late but it has changed significantly over the weekend after input from Pat O on Friday. I am looking forward to presenting to you all tomorrow. There are several areas I would most appreciate feedback (although any ideas are welcome). 1- What should be the balance of resident driven assessment and faculty driven assessment for entrustment of trainees in GME. 2- How to best assess the implementation of this system (ie: process measurements- completion rates, time until completion vs. outcomes measures- satisfaction, EPAs vs. milestones for assessment) 3- Amount of time needed to ask a data management consultant to be involved to help us prepare and collect appropriate assessment data Thanks again! Jeff Creation of a learner driven GME EPA assessment network for internal medicine residency and fellowship programs. Background Assessment of graduate medical education trainees is a high priority of training programs. Training program directors must be able to certify that graduates are able to practice independently in their respective specialty/subspecialty. Various frameworks have arisen to guide how to assess and report the competence of trainees. Increasingly, professional milestones are used by program directors to ensure that trainees are ready for independent practice In the case of internal medicine, both the body accrediting programs (ACGME) and the organization certifying individuals (American Board of Internal Medicine (ABIM)) have had major roles in structuring how program directors assess trainees in medicine specialties and subspecialties. Their philosophy has evolved over time to include greater proscription of this assessment. This evolution began in 1999 when the ACGME introduced the six core competencies (patient care, medical knowledge, systems-based practice, practice-based learning, communication and professionalism). This began a transition of philosophy of accreditation from process to training outcomes. The recent introduction of the Next Accreditation System (NAS) evolved these concepts to include milestones as subsections of the core competencies. The internal medicine community developed 142 educational milestones, now termed curricular milestones, to further describe the knowledge, skills and attitudes of observable development from a novice to a proficient trainee. The developmental milestones were recognized as being too extensive to be effectively implemented or evaluated. A second effort produced the reporting milestones, a narrative based set of 22 milestones. The 6 ACGME competency domains organize these 22 milestones such that each competency now has 2 to 5 subcompetencies. (2) An alternative approach to assessment involves using entrustable professional activities (EPAs) as a framework for assessing competence. EPAs reflect the degree of mastery of professional tasks that together constitute the work of a profession. (3) Carrying EPAs requires abilities in multiple competencies. This approach recognizes that professional tasks are complex and breaking those tasks down to discreet, measurable steps, such as might occur with a milestone based approach, loses the ability to provide a holistic view of the successful acquisition of professional skills. These EPAs are best evaluated by observation of professional skills by experienced faculty members. Current UCSF Department of Medicine Assessment Strategy: As required by the ACGME and the ABIM, all Department of Medicine (DOM) ACGME training programs assess the specialty/subspecialty specific milestones; the reporting milestones are recorded in the Evalue platform system. Programs may deploy different tools (global assessments, procedure observations, 360’s, chart stimulated recall, qualitative comments) to assess their program specific milestones but most programs depend upon observational methods to record the initial milestone assessment. Clinical competency committees (CCCs) then meet to determine the summative milestone score that is reported to the ACGME and the ABIM. The CCCs are largely dependent upon the milestone scores obtained from direct faculty observations. Analysis of Current Milestone Assessment Strategy Program CCCs are reporting issues with their newly implemented milestone assessment processes that have been in effect since AY2013-14 for the internal medicine residency program and AY2014-15 for the fellowship programs. First, compliance with completing the assessments is poor; across the DOM training programs, the overall compliance of assigned evaluations is initially only 50%.. Much administrative time is spent trying to get completed evaluations to the required 70% level and often program leadership has to step in to improve faculty compliance. Reasons faculty cite for their challenges in completing assessments is “assessment fatigue” caused by multiple end of the month evaluations being due simultaneously, the need to assess as many as 22 milestones as well as overall frustration with the Evalue platform. Second, the quality of the assessments is also in question. CCCs are now often basing their judgments too few numeric scores on each milestone category bringing their validity into question. This has led CCCs to have concerns about whether they are fully able to assess and report trainee’s performances. Similarly, it creates doubt that CCCs are able to effectively identify areas of improvement for advisors to help trainees. In response to these concerns about a milestone assessment based system and wanting to improve trainee assessment, the internal medicine residency program assessment leadership team began exploring using an EPA based assessment system in 2013. In 2013-4 we utilized a Delphi method to implement a group of 8 EPAs to help make our assessments more activity specific. (6) The EPAs are housed on the UCSFEPA.org website and contain the following assessments: •Serious Illness Communication EPA •Rounds Observation EPA •Discharge summary EPA •4 habits clinic survey •Clinic Post-Discharge EPA •Acute Care EPA •Code Leadership EPA •Multidisciplinary Rounds Inpatient Feedback These assessments are recorded utilizing Qualtrics through the UCSF MyAccess website and are accessed by the faculty to generate evaluations. Several internal medicine fellowships (Palliative Care, Geriatrics and Hematology/Oncology) have begun to use EPAS and the UCSFEPA.org platform for assessment of their trainees. Each of these EPAs can be mapped to several milestones at the same time as is shown in the following chart from proposed gynecology residency EPAs. Benefits of using EPAs includes improved overall compliance with obtaining assessments due to trainee initiation of the assessment, real time assessment by the faculty and ease with utilizing the Qualtrics platform. Although not formally compared, there is a sense that the quality of the EPA assessments may be better than the milestone based assessments. Although these, and future EPAs, consist of a robust network of evaluations, we have been unable to fully implement them due to several limitations with our assessment technology and expertise. The GME office is now able to address these challenges by adding administrative leadership and data management assistance. This help creates a firm infrastructure but to create a trainee centered, interactive assessment network we will need additional help from Information Technology (IT) to create a more seamless platform. Past Assessment Efforts: Over the last four years we have made a concerted effort to bring a coordinated IT effort to enable utilizing our EPA network. Our initial efforts utilized the Mahara portfolio platform. Conceptually this system offered several advantages including resident control over their assessments on their own customizable webpage. Material could be collected and correlated for review with trusted advisors and create a framework for individual assessment that could highlight a trainee’s skills. Unfortunately, residents did not utilize this tool for several reasons. First, residents were too busy to log on to the system to record evaluations. Second, they did not feel empowered to ask for completion of evaluations. Third, since the Mahara system was completely resident driven there was no way to reliably track resident completion of educational tasks. Efforts to move Myfolio system through the Evalue platform were similarly unsuccessful due to data management problems and the inability to design an appropriate single log-in access for faculty or residents to review. Also, residents did not have ability to control their assessment information to pick their best work to present to the CCC. Last year we moved our EPAs to the Qualtrics survey platform and housed our EPAs on a website created through consultation with Eric Widera MD, from the department of geriatrics and palliative care. This system created a much easier system to collect EPA data, but currently our faculty completion rates remain low as there is are no automatic reminder systems to help busy clinicians to remember to complete these evaluations. The EPAs that are most successful have a faculty champion, such as Heather Whelan MD, a hospitalist at the VAMC. Each month she circulates a meeting list to our ward interns to schedule time to complete this EPA. This activity has created popular feedback for our interns and is quite well received by our housestaff. This individual effort is time intensive, however, and unlikely to be sustainable leaving our EPA system longevity in doubt. During this time we began the process of seeking more information from our trainees about what their goals are for their assessment process by doing focus groups with convenience samples of residents. Focus Group Themes: Eight focus groups in our internal medicine residency (and fellowship) programs over the last three years involving approximately one-hundred trainees have demonstrated several themes regarding our assessments. These themes were derived from our focus group notes and match concerns voiced by resident trainees across the country when there is inadequate supervision or feedback. (4-5) First, residency assessment that depends on summative feedback from end of rotation, milestone-based assessments, lack specificity to enable residents to improve their professional practice. Residents would prefer more timely, qualitative, in-person and practice based feedback to help them grow professionally. Second, currently used assessment tools create scores and comments that are difficult for residents to understand or access to help them follow their progress. Third, with the advent of the Clinical Competency Committee (CCC) mandated by the ACGME, residents feel there is a lack of transparency or control over their own assessments leading to mistrust of the evaluation system. Finally, the current culture in our residency and fellowship programs does not facilitate constant, clear and continuous feedback from faculty to trainees or from trainees to faculty. Residents feel this acutely and do not feel they have permission to give constructive feedback to faculty and often feel criticized when receiving anything less than superlative feedback from faculty. Current Pilot Program: With the help of Holly Nishimura BA, and Christy Boscardin PhD, fifty two of our internal medicine Prime residents are starting a two month evaluation project where they actively solicit EPA activity based feedback from faculty or other professional staff. These evaluations will be completely resident driven and will be collected in Qualtrics. Each participating resident was assigned a unique code number by Amy Forseth BA, our division administrator. She then emailed this individual code to each participating resident. The email code is unique to each participant and is easily forwarded to observing faculty and staff. The forwarded email automatically links the observing faculty member to the EPA survey menu where they can easily choose the EPA they observed and quickly complete the evaluation via email. The data are then captured for that individual resident. This “proof of concept pilot” enables us to examine the rates of completion of EPAs, willingness of residents to participate in the process and their satisfaction with the feedback they receive. Although this pilot is an exciting advance, it only fulfills our goals of facilitating timely resident feedback, it does not address our goals of creating an accessible resident dashboard where they are able to drive their own assessments and highlight their best work for the CCC. It also only takes a small incremental step towards moving our assessment and feedback culture forward to be more open and meaningful. Proposal Goals: The goal of our proposal is to address the four listed focus group themes by restructuring our assessment system over the next five years to be primarily trainee driven and to improve our information system so that all evaluations will be available to, and controlled by, the residents who receive them. Our vision is that every trainee entering the internal medicine residency or subspecialty fellowship programs would be given an assessment “dashboard” that would collect and store information that demonstrates their progress towards independent practice throughout their training. Data would be collected through a number of sources; Evalue, EPAs from Qualtrics, inservice exam scores, clinic patient dashboards and resident portfolio data and will be mapped to milestones to facilitate reporting to the ACGME. Trainees will be able to review all their data and will be able to “release” their best work to demonstrate their entrustability on the milestones. This trainee assessment dashboard will use the same Qlikview platform used by the medical school. Therefore our project research question is: Is restructure of competency assessment to a trainee-driven process associated with improved understanding of resident’s preparedness for independent practice amongst UCSF GME trainees? Process Proposal: Create a resident-driven, EPA based evaluation network that will expand following the previously published Delphi-derived EPAs for internal medicine and medicine subspecialty fellowships. The goals of the project will use the focus group themes to create a learner driven evaluation network with a goal of addressing each of the four themes. Theme #1: To create more timely opportunities for feedback the residents will be asked to solicit evaluations from their observing faculty. Trainees will send a uniquely coded email to the faculty member that requests feedback on the EPA activity they want assessed. Residents will be required to complete at least 3 EPAs per activity per year utilizing different faculty assessors, but they can choose which of the scores and assessments they release to the CCC for final review. Theme #2: Accessibility to their feedback will be ensured through creation of a resident assessment home page for each resident in the program. The homepage will contain sections that organize and display summative data from Evalue, EPA feedback evaluations, in service exam scores and a resident portfolio that allow the resident to track and record their clinical and academic progress by uploading documents that support mastery of individual milestones. Residents cannot edit this material but can add annotations if they so desire. This homepage will be based on work done in the SOM after meeting with Maxine Papadakis MD, Karen Hauer MD, PhD and Bonnie Helvig BA regarding strengths and challenges with their current dashboard program. Importantly, this system must have the flexibility to modify and grow as we fine tune assessments of trainee activities. Dashboard homepages will contain: Each trainee’s original ERAS application, Evalue and Qualtrics data for evaluations, a schedule function for viewing past/present schedules as well as vacations with an interactive timeline to enable residents to track administrative tasks, links to online modules that the residents need to access/complete (and to be able to record when they have completed them), self-assessment tools for faculty/trainee reviews, records for communication for feedback from our CCC, individual trainee quality of care dashboard data from both inpatient and clinic practice as well as instructional links and short videos instructing how decipher data as it comes in. Please see sample homepage provided below. Theme #3: Residents will control the data contained on their homepage. Residents can choose which EPA evaluations are available for the CCC enabling them to show off their best work. Similarly, CCC reports will become available to residents after each meeting so they can follow their progress on the ACGME milestones. This is based on the theoretical work presented by Patricia O’Sullivan PhD in her portfolio seminar regarding learning theory and adult learners. Theme #4: Our hope is that along with our fledgling faculty education efforts, constant collection of resident driven EPA based data will slowly help begin an overall culture change in assessment and feedback in our department. Residents will become more comfortable asking for activity specific feedback and faculty will become more comfortable giving it. This culture change will take time and effort but the resident focus group data was clear that they want timelier, activity-driven feedback so they should be motivated to ask for it. Sample Resident Landing Page: Specific Aims: 1- Create a resident and fellow assessment network that utilizes a resident driven, EPA based evaluations. 2- Create an individual resident homepage that will become a landing page that can link residents to all their assessment materials but also to UCSF based learning resources. 3- Ensure a more organized and efficient assessment data management system. 4- Change culture for assessment and feedback to become more transparent, ongoing and meaningful system for our trainees. Evaluation Plan: Process measures 1234- Percentage of responses to emails c/w Evalue time to completion of epa evaluations c/w evalue descriptive eval of epas completed amount of time of resident use of dashboard 5- actual vs reported numbers of epas completed Outcome measures 1- satisfaction (faculty/trainees) with system (focus groups) 2- comparison of entrustment on mapped epas c/w milestones 3- number of residents entrustable via epas c/w evalue milestones what about how it influences CCC Plan for Sustainability: After the initial start-up effort and costs to construct the Dashboard system this assessment system should be able to collect all the assessment data (Evalue, Qualtrics, Portfolio, In-service scores, Qualitative comments, clinic dashboards, patient follow-up reviews), create summary milestone reports for the CCC, and be updated annually for new residency and fellow trainees each year. The estimate from the Information Services Unit (ISU) group is that it will take 6 hours, $500 annually, for trouble shooting and updates to the system which will be made available from Departmental funds. Updates and administrative work will mostly involve construction of the new trainee dashboards which can be done by our program administrator, Amy Forseth. Team Members: Jeff Kohlwes MD, MPH. School of Medicine. Department of Internal Medicine. Clinical Professor of Medicine. Director, PRIME Residency Program, Associate Program Director for Assessment and Feedback Internal Medicine Residency Program. Patricia Cornett MD. School of Medicine. Department of Internal Medicine. Clinical Professor of Medicine. Associate Chair for Education, Department of Internal Medicine. Vanessa Thompson MD. School of Medicine. Department of Internal Medicine. Assistant Clinical Professor of Medicine. General Medicine Clinic Assistant Medical Director San Francisco General Hospital, Internal Medicine Residency Director of Academic Development Irina Kryzhanovskaya MD. School of Medicine. Department of Internal Medicine. Senior Resident in Internal Medicine, Chief Resident-Elect. Ray Chen MD. School of Medicine. Department of Internal Medicine. Junior Resident in Internal Medicine Total Budget 10. Consultations Completed: Nina Jameson, Deputy Director, Program Management, Information Services Unit (ISU)- Consultation on costs on IT solutions. Maxine Papadakis MD, Bonnie Helvig BA, UME Dashboard and IT expert for demonstration on UME dashboard and problem solving on creation of GME dashboard. Karen Hauer MD, PhD consultation on assessment of EPAs and milestones. Christy Boscardin PhD, Holly Nishimura BA, Department of Medical Education- Assessment expertise and Qualtrics planning for the current Pilot Study. References: 1- Green et al, J Grad Med Educ. 2009; 1:5-20. 2- http://www.acgme.org/acgmeweb/portals/0/pdfs/milestones/internalmedicinemilestones.pdf Accessed 11/13/15 3- Ten Cate et al. Academic Medicine, Vol. 82, No. 6 / June 2007 4- Farnan et al. A systematic review: the effect of clinical supervision on patient and residency education outcomes. Acad Med. 2012 Apr;87(4):428-42. 5- Foster et al. RAFT (Resident Assessment Facilitation Team): supporting resident well-being through an integrated advising and assessment process. Fam Med. 2012 Nov-Dec;44(10):731-4 6- Hauer K, et al. Identifying entrustable professional activities in internal medicine training. J Grad Med Educ. 2013 Mar;5(1):54-9.