full text
advertisement

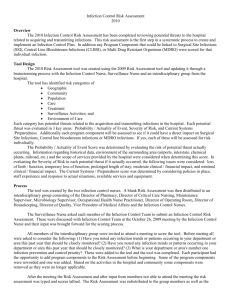
Prevention of central line-associated bloodstream infections through quality improvement interventions: a systematic review and meta-analysis Koen Y Blot, Jochen Bergs, Stijn I Blot, Dominique M Vandijck Affiliations Faculty of Medicine and Health Sciences, Ghent University, Ghent, Belgium (KY Blot BSc, Prof SI Blot PhD, Prof D Vandijck PhD); General Internal Medicine and Infectious Diseases, Ghent University Hospital, Ghent, Belgium (Prof D Vandijck PhD); and Health Economics and Patient Safety, Hasselt University, Diepenbeek, Belgium (J Bergs MSc, Prof D Vandijck PhD) Corresponding author Koen Blot, Ghent University, Faculty of Medicine and Health Sciences, 9000 Ghent, Belgium, koen.blot@ugent.be, +32476992438 Keywords Central line-associated bloodstream infection, catheter-related bloodstream infection, quality improvement intervention, compliance, meta-analysis. Summary (39 of 40 words) Nosocomial central line-associated bloodstream infections are associated with the use of central venous catheters. Quality improvement interventions aim to improve professional adherence to prevention measures. The results of the meta-analysis provide evidence that quality improvement interventions decrease infection rates. 1 Abstract (146 of 150 words) Background A systematic review and meta-analysis was performed to examine the impact of quality improvement interventions on central line-associated bloodstream infections in adult ICUs. Methods Studies were identified through Medline (1995–June 2012) and manual searches. Odds ratios (OR) and 95% CIs were calculated for infection rate reductions using a random-effects model. Subgroup analysis assessed the impact of bundle/checklist interventions and high baseline rates on treatment effect. Results Forty-three studies were included. Meta-analysis of interrupted time series studies revealed an infection rate reduction three months post-intervention (OR 0.30; 95% CI 0.10–0.88; p=0.03). Likewise, before-after studies identified an infection rate decrease (OR 0.39; 95% CI 0.33–0.46; p<0.001). This effect was more pronounced for before-after trials implementing bundle or checklist interventions (p=0.03). Conclusion This analysis suggests that quality improvement interventions contribute to the prevention of central lineassociated bloodstream infections. Implementation of care bundles and checklists appears to yield stronger risk reductions. 2 Introduction Central venous catheters, central lines that terminate at or close to the heart, are indispensable devices in the intensive care unit (ICU). Approximately half of patients admitted require a central line for infusion of medication, fluid, or blood products, hemodialysis, withdrawal of blood, or hemodynamic monitoring. However, use of these invasive devices predisposes for the development of central line-associated bloodstream infections (CLABSI). These serious, preventable complications increase patient morbidity, leading to increased length of hospitalization and resource use.[1,2] Moreover, CLABSI might impact mortality and compromise patient prognosis.[3-5] Infection prevention measures during insertion or maintenance of central lines, such as hand hygiene, use of maximal sterile barriers upon catheter insertion, disinfecting the skin with chlorhexidine, optimal catheter site selection, and daily review of line necessity with prompt removal of unnecessary lines, have been proven to decrease the risk of CLABSI incidents.[6,7] The Institute for Healthcare Improvement (IHI) recommends use of the aforementioned items, in the form of a central line care bundle, to decrease CLABSI occurrence. Despite the presence of evidence-based interventions, summarized in guidelines,[8,9] CLABSI remain a substantial threat for hospitalized patients, with pooled estimated mean occurrence rates of 4.4 CLABSI per 100 devices inserted (95% confidence interval [CI] 4.1–4.9) and 2.7 CLABSI per 1000 catheter days (95% CI 2.6–2.9).[10] In recent years it has become clear that the limiting factor to infection prevention is the implementation rather than publication of recommendations.[11] Introducing prevention measures may be hampered by multiple factors, such as lack of problem awareness, poor familiarity or non-agreement with the guidelines, low self-efficacy, inability to change previous practice, or lack of resources.[12,13] Quality improvement interventions such as personnel education, feedback reporting of infection rates, or use of central line care bundles and checklists aim to decrease CLABSI incidence by improving adherence to prevention measures.[14] However, the efficacy of these interventions has not yet been fully assessed. The objective of this study was to examine whether quality improvement strategies, defined as a combination of quality improvement interventions, reduce CLABSI rates in the adult ICU. Subgroup analyses were conducted to determine whether certain quality improvement interventions led to stronger 3 infection rate reductions. 4 Methods Search strategy Medline was systematically searched (1995–June 2012) through PubMed MesH terms. Extra studies were identified by scanning reference lists of articles, manually and through Ovid and ScienceDirect databases. A combination of the following search terms was used: catheter-related infections/prevention and control; catheterization, central venous/adverse effects; catheters, indwelling/adverse effects; infection control/methods; infection control/standards; intensive care units; quality control; quality of health care; and bundle. (webappendix 1). The search strategy was developed by two authors (KB and DV) and performed by one investigator (KB). Study selection Eligible studies used before-after, interrupted time series (ITS), controlled before-after, non-randomized controlled trial, or randomized controlled trial study designs that complied with the Cochrane EPOC Group methodological criteria. ITS studies report at least three data points before and after a defined point in time in which the intervention is implemented. Participants consisted of adult ICU patients with central line catheters. Trials implemented a quality improvement intervention aimed at increasing professional adherence to evidence-based infection prevention processes. The primary outcome measure was the CLABSI rate: the number of CLABSI per catheter days during pre- and post-intervention. Only English language papers were included. Medline search results were screened and excluded by their title or abstract (KB). Selected papers underwent a full-text assessment (KB) and eligibility issues were resolved between authors (KB, SB, DV). Data extraction Extracted data included author and year of publication, settings and study populations, study designs and periods, implemented quality improvement and preventive interventions in the baseline and intervention periods, number of CLABSI and catheter days, and applied CLABSI definitions. Secondary outcome 5 measures such as length of stay, mortality, hospital costs and savings, and compliance reporting were likewise noted for the systematic review. Two authors (KB and DV) developed a data extraction sheet and one reviewer (KB) retrieved the data from included studies. Study authors were not contacted for additional data. To obtain effect sizes for ITS studies, infection rate data was extracted from figures published in original papers using the program PlotDigitizer. Results reported as a mix from both included and excluded study participants were included. When studies provided only two of three CLABSI rate parameters (number of CLABSI, catheter days, and CLABSI per 1000 catheter days), the third was derived through manual calculation. To avoid adding extraneous data, quality improvement interventions were classified under general headers (webappendix 2) and only preventive interventions described by the CDC guidelines[8] and applicable to the majority of ICU patients were noted. Quality assessment The Downs and Black checklist was applied to ascertain study methodological risk of bias (KB).[15] The tool consists of 27 questions concerning the reporting, external validity, internal validity, and power of nonrandomized studies of health care interventions. Studies were scored based on whether they sufficiently fulfilled the items. The criteria for these individual checklist items were adapted for CLABSI studies following discussion between authors (KB, SB, DV). A power analysis was performed to determine whether studies had a sufficient sample size to detect an odds ratio (OR) of 0.50 with a p-value of less than 5%. Statistical analysis A random-effects meta-analysis was performed using the DerSimonian-Laird estimator to obtain the OR and 95% CI for CLABSI rate reductions. Clinical heterogeneity was assessed by comparing study settings, CLABSI definitions, and intervention implementation methodology. The Higgins I2 test was predefined to quantify heterogeneity (I2≤25% for low, 25%<I2<50% for moderate, and I2≥50% for high). Subgroup analysis by means of meta-regression was carried out for before-after study designs by comparing treatment effects between studies that did and did not implement bundle/checklist interventions and studies with a baseline rate above or equal to and below 4.0 CLABSI per 1000 catheter days. A funnel plot was 6 constructed to assess publication bias and a sensitivity analysis was performed to identify heterogeneous studies that could influence the meta-analysis model. Monthly ITS study data was standardized by dividing the outcome and standard error (SE) by the pre-intervention standard deviation (SD). One study reported annual data points; these were used for the 12 and 24 month follow-up analyses.[16] The intervention effect was calculated through SPSS version 22, using segmented time series regression analysis, taking into account time trend and autocorrelation among the observations. A negative change in level or slope indicates an intervention effect: an infection rate reduction.[17] A p-value less than 0.05 was used to denote statistical significance. Role of the funding source There was no funding source for this study. SB holds a research mandate of the Specific Research Fund at Ghent University. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication. 7 Results The search algorithm identified 633 abstracts (627 in PubMed and six in Ovid and ScienceDirect). Fortythree studies, published in English between January 1995 and June 2012 consisting of 584 ICUs, were included for meta-analysis (figure 1). Two studies[18,19] continued their quality improvement initiatives and republished their old data with new results.[7,20] The older study by Coopersmith et al.[18] was included for the meta-analysis of ITS studies and the paper by Pronovost et al.[19] was accessed to supplement information. One trial could not be included for meta-analysis because although baseline and intervention period interventions were qualitatively different, no new intervention types were implemented.[21] Another study included multiple sets of data, for which the set with the longest follow-up period was chosen.[22] Eleven studies could not included for ITS analysis because they implemented interventions in a step-wise manner.[20,21,23-31] The majority of the 43 studies were prospective before-after intervention trials in medical-surgical ICUs (webappendix 3). Most trials implemented quality improvement interventions without simultaneously introducing new prevention measures and used CDC definitions for CLABSI diagnosis. The 584 included ICUs consisted of 564 adult, 11 pediatric,[22,32,33] and nine neonatal units.[22] Four studies, reported the number of adult ICUs studied, but did not specify the ICU type (n=270).[33-36] The remaining 294 adult ICUs were primarily mixed medical-surgical (n=135), medical (n=51), and surgical (n=61). The analysis consisted of 35 before-after,[6,20,22,24-26,31-59] seven interrupted time series,[16,18,38,6063] and one controlled before-after study.[64] Five of the ITS studies were eligible for inclusion in the meta-analysis consisting of primarily before-after study designs.[16,38,61-63] Duration of study periods ranged from nine[56] to 180 months,[16] with a mean length of 26.75 months. Multiple quality improvement interventions were implemented in combinations (figure 2). Up to 14 different types of interventions were reported: personnel education, feedback reporting of infection or compliance rates, use of care bundles or checklists, prepackaged catheter carts or kits, surveillance of compliance with infection prevention processes, posters that raise awareness or report infection or compliance rates, designation of leaders or champions for CVC prevention measures, empowering nurses to 8 stop incorrectly performed procedures, clinical reminders, distribution of fact sheets or leaflets, personnel training, organizational changes, and installation of hand-rub dispensers (figure 3). There were levels of variability between implemented quality improvement interventions, the detail with which they were reported, and the methods used to apply them. Nearly all trials implemented educational interventions (n=33) consisting of single, monthly, quarterly, or yearly sessions on CLABSI prevention. Feedback reporting of infection or compliance rates to personnel occurred at monthly or quarterly intervals. Likewise, surveillance of compliance with preventive interventions was implemented daily, periodically, or at random intervals. Half of trials implemented bundle or checklist interventions (n=20). Trials either initiated bundle interventions without checklists (n=2),[6,43] only checklists because bundles were used during the baseline period (n=9),[36,42,50,51,53,55,57,60,61] or both bundle and checklist interventions (n=9).[25,26,31,33,35,39,41,45,52] Differing amounts of care items were grouped together to form a care bundle or checklist. Two trials[50,57] did not report which care items comprised their bundle and one used a checklist for one sole care process.[51] Other trials used either all five (n=7),[6,25,35,36,41,52,61] four (n=5),[26,31,39,45,60] three (n=3),[33,42,53] or two (n=2)[43,55] IHI care items in their bundle or checklist. Four studies concomitantly targeted other healthcare-associated infections such as ventilator-associated pneumonia (VAP),[34] both VAP and catheter-associated urinary tract infections,[26,57] or VAP and surgical site infections.[32] Eight studies simultaneously initiated new prevention measures alongside their quality improvement interventions.[24,37,38,40,41,46,50,51] The total number of CLABSI and catheter days were provided by 32 studies and manually calculated for eight.[6,16,34,39-41,48,53] The baseline CLABSI incidence varied between studies: rates ranged from 2.1[32] to 46.3 CLABSI per 1000 catheter days.[44] Sixteen trials[24,25,32-35,41,49-51,55-57,59,60,62] reported baseline infection rates equal to or lower than 5 CLABSI per 1000 catheter days and six trials above 15 CLABSI per 1000 catheter days.[16,22,39,44,47,58] Total scores on the Downs and Black quality assessment tool ranged from 15[57] to 26,[20,22,47] with a median score of 21 (webappendix 4). The checklist revealed that two studies did not describe their CLABSI 9 definition,[38,57] nine did not interventions,[22,31,41,44,51,54,55,57,63] sufficiently and 27 describe measured their quality compliance with improvement preventive intervention.[6,20,22,25,31,33-36,38,39,42-44,46-48,51,53-58,61,64] Twenty-two reported confounding factors such as duration of catheterization, patient characteristics or injury severity,[18,20,22,2426,37,39,41,44,48-52,55,56,59,61,64,65] which were comparable between baseline and intervention in 18 trials.[18,20,22,25,26,37,44,48,50-52,55,56,59,61,64,65] However, two trials corrected for the measured differences in patient characteristics.[39,49] The power analysis revealed that studies tended to have either low (n=24) or high power (n=13).[6,16,20,22,24,32,35,36,45,47,50,54,63] Nearly all trials demonstrated CLABSI rate decreases, only ten did not achieve statistical significance.[34,37,39,48,49,53,55,57,62,64] Two studies, reporting outcomes from ICUs separately, revealed non-significant results for neurosurgical, neurological, cardiothoracic, and coronary care units, yet decreased their total CLABSI rate.[44,45] Meta-analysis was performed on 41 before-after and seven ITS study designs to assess the impact of quality improvement interventions on the occurrence of CLABSI. The before-after trials showed a reduction in the CLABSI rate (OR 0.39; 95% CI 0.33–0.46; p<0.0001, figure 4) with high statistical heterogeneity (I2=85.4%). Analysis of six ITS studies, involving 11 ICUs, identified a change in level for the CLABSI rate at 3 months post-intervention (OR 0.30; 95% CI 0.10–0.88; p=0.028, figure 5) with low heterogeneity (I2=24.5%). Changes in infection rate slope (OR 0.81; 95% CI 0.59–1.13; p=0.216) and levels at 6 (OR 0.36; 95% CI 0.11–1.19; p=0.094), 12 (OR 0.17; 95% CI 0.02–1.27; p=0.084), and 24 months postintervention (OR 0.052; 95% CI 0.003–1.02; p=0.051) trended towards reductions, yet were not significant. Subgroup analysis of before-after trials revealed that the CLABSI risk reduction was significantly stronger (p=0.026; figure 4) in trials implementing care bundles or checklists (OR 0.34; 95% CI 0.27–0.41) than in those implementing other interventions (OR 0.45; 95% CI 0.36–0.55) (webappendix 5). Further analysis revealed that studies with baseline rates above 4.0 CLABSI per 1000 catheter days (OR 0.37; 95% CI 0.33– 0.46) did not demonstrate significantly better risk reductions (p=0.18) compared to studies below this infection rate (OR 0.49; 95% CI 0.37–0.66). 10 Funnel plots displayed asymmetrical patterns for before-after, but not ITS study designs (webappendix 6). The results of the sensitivity analysis of before-after study designs suggest that two studies contribute to residual heterogeneity; removing them from the meta-analysis model would reduce variability between studies.[47,50] However, doing so does not affect the results, therefore the choice was made to retain these studies (webappendix 7). 11 Discussion The results of the meta-analysis of 43 studies, involving 584 ICUs, provide evidence that quality improvement interventions reduce CLABSI rates in adult ICUs. The effect size of 41 studies was significant yet highly heterogeneous. This infection rate decrease was more pronounced in studies using bundles or checklists, suggesting that implementation of these interventions as part of a quality improvement strategy lead to stronger rate reductions. The change in infection rate level for six studies at 3 months follow-up also demonstrates the beneficial impact of quality improvement interventions, but with a low level of heterogeneity. Changes in levels at the 6, 12, and 24 month period were not significant yet trended towards decreases. Reflecting the importance of multifaceted initiatives to improve patient safety culture, studies often implemented multiple quality improvement interventions, as recommended by guidelines.[8] Strengths of this study include the comprehensive search strategy encompassing various quality improvement interventions, the methodological quality assessment of trials, and the random-effects model analysis with multiple studies and interrupted time series study designs. It is however hampered by certain limitations: a lack of randomized or controlled study designs, inconsistent reporting of prevention measure compliance, and heterogeneity. Before-after studies run a higher risk of bias due to their liberal study design: they hamper the ability to recognize phenomena that influence the CLABSI rate such as virulent epidemic outbreaks or spontaneous regression to the mean.[14] There is some evidence to suggest that the effects of quality improvement interventions are overestimated when based on before-after studies. Time series designs limit this risk of bias by attempting to detect whether an intervention has had an effect significantly greater than the underlying baseline trend.[66] However, since these designs require initiatives to begin at a well-defined point in time, 11 studies with step-wise intervention implementation had to be excluded. Clinical and methodological heterogeneity stemmed from the use of differing intervention strategies, study designs, population characteristics, and baseline standard of care. No distinction was made between interventions applied as part of a structured program or introduced to solve a specific recurring problem. Such differences in intervention implementation cannot be readily quantified. For example, one study formed a team of nurses to evaluate care processes and data related to an infection rate increase. By applying 12 a comparable yet distinct quality improvement strategy, they decreased their rate from 1.5 to 0 CLABSI per 1000 catheter days.[21] Additionally, this review did not aim to identify strategies that lead to an optimal uptake of quality improvement initiatives. Although interventions implemented in settings with higher baseline rates are more likely to be successful, no significant difference (p=0.18) was found between studies with baseline infection rates above or below 4.0 CLABSI per 1000 catheter days, a rate that is neither optimal nor drastic. Noteworthy is that the study with the lowest baseline rate (2.1 CLABSI per 1000 catheter days) still achieved a significant rate reduction by providing feedback of biannual infection rates.[32] There are several issues related to the meta-analysis of before-after studies. All quality improvement interventions were considered to have an equal impact, yet this may not be a fair assumption. For instance, if a new intervention takes months to implement, then those introduced in a later study phase could have less effect compared to earlier initiatives. Bias could also be present due to inclusion of studies from identical authors.[22,47,54,58,59,63,64] Two of these studies were performed in the same hospital, which could lead to an overestimation of the intervention effect due to hospital experience in intervention implementation.[58,64] Furthermore, results of the forest plot of 41 studies revealed a lack of smaller studies with less drastic infection rate decreases, suggesting the presence of publication bias. Nevertheless, analysis of ITS designs aims to avert such barriers, and there was no evidence of publication bias amongst those studies. This meta-analysis is the first to include before-after studies researching the prevention of CLABSI through quality improvement interventions and identify a preventive effect associated with care bundle and checklist interventions. Two previous systematic reviews concluded that they were unable to ascertain which quality improvement interventions should be recommended for widespread implementation.[14,67] Another recommended the use of educational programs and multidisciplinary teams.[68] One other meta-analysis included ITS studies, yet used differingg population criteria. They reported mixed effects on the CLABSI rate, with small effect sizes.[17] Comparable points of criticism noted by these papers was the low quality of included studies due to high baseline infection rates, inadequate reporting of multiple CLABSI data points, process adherence measurements, and intervention details. 13 In conclusion, the results of this meta-analysis provide evidence that quality improvement interventions reduce infection rates in intensive care units. Forty-one studies demonstrated consistent, beneficial results, which appeared to be more pronounced amongst studies implementing care bundle and checklist interventions. These findings were corroborated by interrupted time series studies. Conflicts of interest We declare that we have no conflicts of interest. Contributors KB conceived and designed the study, performed the search of published work, literature search, data acquisition, interpretation and synthesis, statistical analysis, and wrote the paper. JB performed the statistical analysis, contributed to data interpretation, and revised the statistical portions of the report. SB designed the study, substantially contributed to the search of published work and data interpretation and synthesis, and critically revised the final manuscript. DV conceived and designed the study, substantially contributed to data interpretation and synthesis, and critically revised the final manuscript. Acknowledgements The results of this study were partially presented at the 26th annual congress of the European Society of Intensive Care Medicine, Paris, France, 5–9 October 2013. 14 Figure 1. Summary of literature search and study selection 15 Figure 2. Distribution of quality improvement strategy size 16 Figure 3. Number of studies implementing quality improvement interventions 17 Figure 4. Overall effect of quality improvement interventions on CLABSI rates including subgroup analysis of bundle and checklist interventions 18 Figure 5. Change in CLABSI infection rate level 3 months post-intervention 19 References 1. Blot SI, Depuydt P, Annemans L, et al. Clinical and economic outcomes in critically ill patients with nosocomial catheter-related bloodstream infections. Clinical Infectious Diseases 2005; 41:1591– 1598. 2. Umscheid CA, Mitchell MD, Doshi JA, Agarwal R, Williams K, Brennan PJ. Estimating the Proportion of Healthcare-Associated Infections That Are Reasonably Preventable and the Related Mortality and Costs. Infection Control and Hospital Epidemiology 2011; 32:101–114. 3. Rosenthal VD. Central Line–Associated Bloodstream Infections in Limited‐ Resource Countries: A Review of the Literature. Clinical Infectious Diseases 2009; 49:1899–1907. 4. Olaechea PM, Palomar M, Álvarez-Lerma F, et al. Morbidity and mortality associated with primary and catheter-related bloodstream infections in critically ill patients. Rev Esp Quimioter 2013; 26:21– 29. 5. Januel JM , MPH, RN, Harbarth S , MD, MS, Allard R , MD, MSc, et al. Estimating Attributable Mortality Due to Nosocomial Infections Acquired in Intensive Care Units. Infect Control Hosp Epidemiol 2010; 31:388–394. 6. Marra AR, Cal RG, Durao MS, et al. Impact of a program to prevent central line-associated bloodstream infection in the zero tolerance era. Am J Infect Control 2010; 38:434–439. 7. Pronovost PJ, Goeschel CA, Colantuoni E, et al. Sustaining reductions in catheter related bloodstream infections in Michigan intensive care units: observational study. BMJ 2010; 340:c309. 8. O'Grady NP, Alexander M, Burns LA, et al. Guidelines for the Prevention of Intravascular Catheterrelated Infections. Clinical Infectious Diseases 2011; 52:e162–e193. 9. Yokoe DS, Mermel LA, Anderson DJ, et al. Executive Summary:A Compendium of Strategies to Prevent Healthcare‐ Associated Infections in Acute Care Hospitals •. Infect Control Hosp Epidemiol 20 2008; 29:S12–S21. 10. Maki DG, Kluger DM, Crnich CJ. The risk of bloodstream infection in adults with different intravascular devices: a systematic review of 200 published prospective studies. Mayo Clin. Proc. 2006; 81:1159–1171. 11. Blot S, Vandijck D, Vogelaers D, Labeau S. Bridging the gap between theory and practice. ICU Management 2011; :40–11. 12. Labeau SO, Vandijck DM, Rello J, et al. Centers for Disease Control and Prevention guidelines for preventing central venous catheter-related infection: Results of a knowledge test among 3405 European intensive care nurses*. Critical Care Medicine 2009; 37:320–323. 13. Cabana MD, Rand CS, Powe NR, et al. Why don't physicians follow clinical practice guidelines? A framework for improvement. JAMA 1999; 282:1458–1465. 14. Agency for Healthcare Research and Quality (AHRQ). Closing The Quality Gap: A Critical Analysis of Quality Improvement Strategies: Volume 6--Prevention of Healthcare-Associated Infections. 2007; :1–167. 15. Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health 1998; 52:377–384. 16. Fraher MH, Collins CJ, Bourke J, Phelan D, Lynch M. Cost-effectiveness of employing a total parenteral nutrition surveillance nurse for the prevention of catheter-related bloodstream infections. J Hosp Infect 2009; 73:129–134. 17. Flodgren G, Conterno LO, Mayhew A, Omar O, Pereira CR, Shepperd S. Interventions to improve professional adherence to guidelines for prevention of device-related infections. Chichester, UK: John Wiley & Sons, Ltd, 2013. 21 18. Coopersmith CM, Rebmann TL, Zack JE, et al. Effect of an education program on decreasing catheter-related bloodstream infections in the surgical intensive care unit. Critical Care Medicine 2002; 30:59–64. 19. Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med 2006; 355:2725–2732. 20. Coopersmith CM, Zack JE, Ward MR, et al. The impact of bedside behavior on catheter-related bacteremia in the intensive care unit. Arch Surg 2004; 139:131–136. 21. Richardson J, Tjoelker R. Beyond the central line-associated bloodstream infection bundle: the value of the clinical nurse specialist in continuing evidence-based practice changes. Clin Nurse Spec 2012; 26:205–211. 22. Rosenthal VD, Maki DG, Rodrigues C, et al. Impact of International Nosocomial Infection Control Consortium (INICC) strategy on central line-associated bloodstream infection rates in the intensive care units of 15 developing countries. Infect Control Hosp Epidemiol 2010; 31:1264–1272. 23. Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med 2004; 32:2014–2020. 24. Cherry-Bukowiec JR, Denchev K, Dickinson S, et al. Prevention of catheter-related blood stream infection: back to basics? Surg Infect (Larchmt) 2011; 12:27–32. 25. Longmate AG, Ellis KS, Boyle L, et al. Elimination of central-venous-catheter-related bloodstream infections from the intensive care unit. BMJ Qual Saf 2011; 20:174–180. 26. Miller RS, Norris PR, Jenkins JM, et al. Systems initiatives reduce healthcare-associated infections: a study of 22,928 device days in a single trauma unit. J Trauma 2010; 68:23–31. 27. Munoz-Price LS, Dezfulian C, Wyckoff M, et al. Effectiveness of stepwise interventions targeted to decrease central catheter-associated bloodstream infections. Crit Care Med 2012; 40:1464–1469. 22 28. Ong A, Dysert K, Herbert C, et al. Trends in central line-associated bloodstream infections in a trauma-surgical intensive care unit. Arch Surg 2011; 146:302–307. 29. Ramos ER, Reitzel R, Jiang Y, et al. Clinical effectiveness and risk of emerging resistance associated with prolonged use of antibiotic-impregnated catheters: More than 0.5 million catheter days and 7 years of clinical experience*. Critical Care Medicine 2011; 39:245–251. 30. Royer T. Implementing a better bundle to achieve and sustain a zero central line-associated bloodstream infection rate. J Infus Nurs 2010; 33:398–406. 31. Seddon ME, Hocking CJ, Mead P, Simpson C. Aiming for zero: decreasing central line associated bacteraemia in the intensive care unit. N Z Med J 2011; 124:9–21. 32. Gastmeier P, Geffers C, Brandt C, et al. Effectiveness of a nationwide nosocomial infection surveillance system for reducing nosocomial infections. J Hosp Infect 2006; 64:16–22. 33. McLaws ML, Burrell AR. Zero risk for central line-associated bloodstream infection: are we there yet? Crit Care Med 2012; 40:388–393. 34. Bonello RS, Fletcher CE, Becker WK, et al. An intensive care unit quality improvement collaborative in nine Department of Veterans Affairs hospitals: reducing ventilator-associated pneumonia and catheter-related bloodstream infection rates. Jt Comm J Qual Patient Saf 2008; 34:639–645. 35. Koll BS, Straub TA, Jalon HS, Block R, Heller KS, Ruiz RE. The CLABs collaborative: a regionwide effort to improve the quality of care in hospitals. Jt Comm J Qual Patient Saf 2008; 34:713–723. 36. Render ML, Hasselbeck R, Freyberg RW, Hofer TP, Sales AE, Almenoff PL. Reduction of central line infections in Veterans Administration intensive care units: an observational cohort using a central infrastructure to support learning and improvement. BMJ Qual Saf 2011; 20:725–732. 23 37. Bijma R, Girbes AR, Kleijer DJ, Zwaveling JH. Preventing central venous catheter-related infection in a surgical intensive-care unit. Infect Control Hosp Epidemiol 1999; 20:618–620. 38. Dixon JM, Carver RL. Daily chlorohexidine gluconate bathing with impregnated cloths results in statistically significant reduction in central line-associated bloodstream infections. Am J Infect Control 2010; 38:817–821. 39. Duane TM, Brown H, Borchers CT, et al. A central venous line protocol decreases bloodstream infections and length of stay in a trauma intensive care unit population. Am Surg 2009; 75:1166– 1170. 40. Frankel HL, Crede WB, Topal JE, Roumanis SA, Devlin MW, Foley AB. Use of corporate Six Sigma performance-improvement strategies to reduce incidence of catheter-related bloodstream infections in a surgical ICU. J Am Coll Surg 2005; 201:349–358. 41. Galpern D, Guerrero A, Tu A, Fahoum B, Wise L. Effectiveness of a central line bundle campaign on line-associated infections in the intensive care unit. Surgery 2008; 144:492–5– discussion 495. 42. Gozu A, Clay C, Younus F. Hospital-wide reduction in central line-associated bloodstream infections: a tale of two small community hospitals. Infect Control Hosp Epidemiol 2011; 32:619– 622. 43. Guerin K, Wagner J, Rains K, Bessesen M. Reduction in central line-associated bloodstream infections by implementation of a postinsertion care bundle. Am J Infect Control 2010; 38:430–433. 44. Higuera F, Rosenthal VD, Duarte P, Ruiz J, Franco G, Safdar N. The effect of process control on the incidence of central venous catheter-associated bloodstream infections and mortality in intensive care units in Mexico. Crit Care Med 2005; 33:2022–2027. 45. Kim JS, Holtom P, Vigen C. Reduction of catheter-related bloodstream infections through the use of a central venous line bundle: epidemiologic and economic consequences. Am J Infect Control 2011; 24 39:640–646. 46. Lopez AC. A quality improvement program combining maximal barrier precaution compliance monitoring and daily chlorhexidine gluconate baths resulting in decreased central line bloodstream infections. Dimens Crit Care Nurs 2011; 30:293–298. 47. Rosenthal VD, Guzman S, Pezzotto SM, Crnich CJ. Effect of an infection control program using education and performance feedback on rates of intravascular device-associated bloodstream infections in intensive care units in Argentina. Am J Infect Control 2003; 31:405–409. 48. Santana SL, Furtado GH, Wey SB, Medeiros EA. Impact of an education program on the incidence of central line-associated bloodstream infection in 2 medical-surgical intensive care units in Brazil. Infect Control Hosp Epidemiol 2008; 29:1171–1173. 49. Seguin P, Laviolle B, Isslame S, Coue A, Malledant Y. Effectiveness of simple daily sensitization of physicians to the duration of central venous and urinary tract catheterization. Intensive Care Med 2010; 36:1202–1206. 50. Shannon RP, Frndak D, Grunden N, et al. Using real-time problem solving to eliminate central line infections. Jt Comm J Qual Patient Saf 2006; 32:479–487. 51. Tsuchida T, Makimoto K, Toki M, Sakai K, Onaka E, Otani Y. The effectiveness of a nurse-initiated intervention to reduce catheter-associated bloodstream infections in an urban acute hospital: an intervention study with before and after comparison. Int J Nurs Stud 2007; 44:1324–1333. 52. Venkatram S, Rachmale S, Kanna B. Study of device use adjusted rates in health care-associated infections after implementation of ‘bundles’ in a closed-model medical intensive care unit. J Crit Care 2010; 25:174 e11–8. 53. Wall RJ, Ely EW, Elasy TA, et al. Using real time process measurements to reduce catheter related bloodstream infections in the intensive care unit. Qual Saf Health Care 2005; 14:295–302. 25 54. Warren DK, Cosgrove SE, Diekema DJ, et al. A multicenter intervention to prevent catheterassociated bloodstream infections. Infect Control Hosp Epidemiol 2006; 27:662–669. 55. Yoo S, Ha M, Choi D, Pai H. Effectiveness of surveillance of central catheter-related bloodstream infection in an icu in korea. Infect Control Hosp Epidemiol 2001; 22:433–436. 56. Zingg W, Imhof A, Maggiorini M, Stocker R, Keller E, Ruef C. Impact of a prevention strategy targeting hand hygiene and catheter care on the incidence of catheter-related bloodstream infections. Crit Care Med 2009; 37:2167–73– quiz 2180. 57. Chua C, Wisniewski T, Ramos A, Schlepp M, Fildes JJ, Kuhls DA. Multidisciplinary trauma intensive care unit checklist: impact on infection rates. J Trauma Nurs 2010; 17:163–166. 58. Lobo RD, Levin AS, Gomes LM, et al. Impact of an educational program and policy changes on decreasing catheter-associated bloodstream infections in a medical intensive care unit in Brazil. Am J Infect Control 2005; 33:83–87. 59. Warren DK, Zack JE, Cox MJ, Cohen MM, Fraser VJ. An educational intervention to prevent catheter-associated bloodstream infections in a nonteaching, community medical center. Crit Care Med 2003; 31:1959–1963. 60. Berriel-Cass D, Adkins FW, Jones P, Fakih MG. Eliminating nosocomial infections at Ascension Health. Jt Comm J Qual Patient Saf 2006; 32:612–620. 61. Peredo R, Sabatier C, Villagra A, et al. Reduction in catheter-related bloodstream infections in critically ill patients through a multiple system intervention. Eur J Clin Microbiol Infect Dis 2010; 29:1173–1177. 62. Perez Parra A, Cruz Menarguez M, Perez Granda MJ, Tomey MJ, Padilla B, Bouza E. A simple educational intervention to decrease incidence of central line-associated bloodstream infection (CLABSI) in intensive care units with low baseline incidence of CLABSI. Infect Control Hosp 26 Epidemiol 2010; 31:964–967. 63. Warren DK, Zack JE, Mayfield JL, et al. The effect of an education program on the incidence of central venous catheter-associated bloodstream infection in a medical ICU. Chest 2004; 126:1612– 1618. 64. Lobo RD, Levin AS, Oliveira MS, et al. Evaluation of interventions to reduce catheter-associated bloodstream infection: continuous tailored education versus one basic lecture. Am J Infect Control 2010; 38:440–448. 65. Seguin P, Rosenthal VD, Cherry-Bukowiec JR, et al. Effect of an infection control program using education and performance feedback on rates of intravascular device-associated bloodstream infections in intensive care units in Argentina. Am J Infect Control 2003; 31:405–409. Available at: http://linkinghub.elsevier.com/retrieve/pii/S0196655302482521. 66. Eccles M, Grimshaw J, Campbell M, Ramsay C. Research designs for studies evaluating the effectiveness of change and improvement strategies. Qual Saf Health Care 2003; 12:47–52. 67. Safdar N, Abad C. Educational interventions for prevention of healthcare-associated infection: A systematic review. Critical Care Medicine 2008; 36:933–940. 68. Aboelela SW, Stone PW, Larson EL. Effectiveness of bundled behavioural interventions to control healthcare-associated infections: a systematic review of the literature. Journal of Hospital Infection 2007; 66:101–108. 27