National Cancer Programme Update January 2015
advertisement

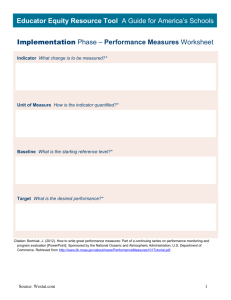
National Cancer Programme Update: January 2015 Welcome to the latest edition of our newsletter, which highlights key areas of our work programme. Please forward this update to interested colleagues. If you don’t want to receive these updates, please reply to this email with “unsubscribe” in the subject line. National Cancer Programme Work Plan for 2014/15 Improving equity in cancer outcomes for all New Zealanders – irrespective of gender, ethnicity or socio-economic status - is a key focus of the recently released National Cancer Programme Work Plan 2014/15 The Programme brings together the work of district health boards (DHBs), regional cancer networks and the Ministry to implement the Government’s priorities for cancer. To improve cancer outcomes for Māori, which are poorer than for the general population, the Programme is guided by the overarching framework and aspirations in the recently refreshed Māori Health Strategy, He Korowai Oranga A framework has also been developed alongside He Korowai Oranga to drive improved equity in health care. The Programme will apply this framework to work plan priorities for 2014/15 to design new approaches that improve cancer outcomes for Māori. Activities already underway include the: Cancer Nurse Coordinator (CNC) initiative newly announced plans for a regional programme of supportive care services ongoing work of the Adolescent and Young Adult (AYA) Cancer Network Aotearoa. Analysis of the new cancer health target data by ethnicity will also provide important information to guide future activities to ensure equity. The 2014/15 Work Plan priorities at a national, regional and local level are: implementing the new Faster cancer treatment health target implementing new budget initiatives sustaining performance against policy priority 30, that is that all patients ready to treat will receive radiation therapy or chemotherapy within four weeks continuing to implement the Faster cancer treatment programme, including: – implementing the tumour standards of service provision work programme – supporting DHBs to implement the CNC initiative. Budget 2014 provided an additional $32.7 million over four years to further improve cancer services and provide better support for cancer patients specifically: $19.5 million will be used to: – employ up to 20 cancer supportive care workers as well as provide funding for psychologists in the six cancer centres to ensure that the supportive care needs of cancer patients and their families are met – develop tools to support full data capture and establish regional information repositories to inform clinical practice and support standardisation of care $8 million will be used to reduce wait times for colonoscopies $5.2 million will be used to increase breast and cervical screening coverage. The new Faster cancer treatment health target Data for the first quarter of the new 62-day Faster cancer treatment health target will be publicly reported for the first time in February 2015. Target Champion Dr Andrew Simpson says significant progress has been made in reducing waiting times for people with cancer over the past six years. The new target will further build on this and support ongoing improvement in services. While the Faster cancer treatment health target focuses on a smaller group of patients than the previous target, it has a whole of pathway approach covering all tests and investigations needed to confirm a diagnosis, as well as all forms of treatment including surgery. Establishing the required data collection and reporting systems for the target has been challenging, but DHBs have made good progress and now have much more visibility across the cancer pathway. Over the next few months, Dr Simpson will visit DHBs to support implementation and visibility of the target. If you would like a visit to your DHB to be prioritised, please email Clare Possenniskie, Programme Manager Faster Cancer Treatment at clare_possenniskie@moh.govt.nz Some key points about the Faster cancer treatment health target and indicators are set out below. Further information is available here on the Ministry website. 62-day Faster cancer treatment health target: On 1 October 2014, the 62-day indicator became the new cancer health target, with 85 percent of patients to be seen within this timeframe by July 2016, increasing to 90 percent by June 2017. The 62-day target covers the length of time from receipt of referral, where the triaging clinician considers there to be a high suspicion of cancer and a need to be seen within two weeks, through to first cancer treatment (or other management). Results against the Faster cancer treatment health target will be published quarterly along with the six other national health targets. 31-day Faster cancer treatment indicator: The 31-day indicator covers the length of time it takes for a patient to receive their first cancer treatment (or other management) from the date of a decision-to-treat. The 31-day indicator includes all patients with a confirmed cancer diagnosis who receive their first cancer treatment, irrespective of how they were initially diagnosed or referred. The 31-day indicator is a policy priority measure. No achievement level has been set for the 31-day indicator. Shorter waits for cancer treatment - radiotherapy and chemotherapy (4 week indicator): Until 1 October 2014 this indicator was the cancer health target. It is now a policy priority measure. The achievement expectation for this indicator continues to be that all patients ready-fortreatment wait less than four weeks (28 days) to receive radiotherapy or chemotherapy from the date of a decision-to-treat. What is the difference between a health target and a policy priority? Both health target and policy priority measures are used to monitor DHBs' performance in achieving the Government’s priority goals and objectives. The main difference is that results against policy priority measures are not publicly reported in the media, although performance is still reported to the Ministry and Minister. Why hasn't the new 31-day FCT indicator replaced the 4 week Shorter waits indicator? Although similar - both indicators measure the length of time from decision-to-treat to treatment - the 4 week indicator covers all chemotherapy and radiotherapy treatment (including adjuvant), while the 31-day indicator measures only the first cancer treatment. Removal of the 4 week Shorter waits indicator would therefore mean that access to adjuvant chemotherapy and radiotherapy would no longer be measured. The Ministry will review the reporting of these two indicators for the 2016/17 financial year but in the meantime DHBs will be required to report against both. Continued reporting during this time will also show that DHBs are maintaining their achievement of the 4 week Shorter waits indicator following the transition to policy priority status. National workshop on Image Guided Radiation Therapy a huge success A first ever national Image Guided Radiation Therapy (IGRT) workshop is being hailed a huge success as a knowledge-sharing forum that could speed up the introduction of new technology around the country and improve patient care. The one day workshop, held in Wellington in October 2014, aimed to promote understanding of IGRT among radiation oncologists, medical physicists and radiation therapists to help with its safe introduction into cancer centres. This includes ensuring IGRT practices are aligned across the country, so patients receive safe, best practice treatment regardless of their location. More than 100 people attended the workshop, which featured two international keynote speakers - Danish medical physicist and lecturer Associate Professor Marianne Aznar and Australian radiation oncologist Professor Michael Barton. Wellington consultant radiation oncologist Dr Carol Johnson, who chairs the Ministry’s Radiation Oncology Work Group, says in recent years the main advances in radiation oncology have been around better use of technology to hopefully improve the disease control or patient toxicity, or both. These advances impact on the way radiation oncologists, radiation oncology medical physicists and radiation therapists can work, and can only be introduced in collaboration. She says all centres have good equipment, but they need the manpower and time to safely introduce the new technology. “Different cancer centres around the country are using new technology differently and some are more advanced in the use of advanced techniques than others,” she says. “Some centres are introducing the technology tumour site by tumour site or anatomic site by anatomic site. “Through the workshop, we wanted to facilitate knowledge sharing to help centres learn from others, to speed up the introduction of new technology and ensure a high standard of treatment is available at all cancer centres. “There was a lot of networking and excited dialogue and contacts being made, as centres all shared their processes. That was certainly a highlight for me seeing people passionate about their work and keen to learn from others.” Dr Johnson says she is indebted to consultant radiation oncologist Dr Nichola Naidoo, who led organisation of the event. It is likely the relevant professional colleges will work together to organise a similar workshop, possibly focusing on stereotactic radiation. Forum to share Faster Cancer Treatment innovation A one day forum will be held in Wellington on 16 April 2015 to share progress and success stories implementing the Faster Cancer Treatment programme. The forum will also support the second round of the Service Improvement Fund being held this year. There will be opportunities for DHBs and regional cancer networks to share their success stories and lessons learned through the first round of the fund and to ask any questions they may have about the second round. The forum is open to all DHBs and further details will be provided soon. Feedback needed on draft prostate cancer guidance The deadline for feedback is approaching on two draft national clinical guidance documents being developed to help primary care and specialist services provide better quality and more consistent care to men with prostate cancer. One set of guidance will help primary care manage men who request a prostate cancer test or have symptoms suggestive of prostate cancer. It includes recommendations on when prostate specific antigen (PSA) results require specialist review. The other guidance will support urologists to provide active surveillance for men with localised, low risk prostate cancer. Documents have been sent to the sector and feedback is due by 5pm on 20 February 2015. It is expected to be published around June 2015. The guidance is being developed by the Prostate Cancer Working Group and its primary care and specialist sub-groups, as part of the Ministry’s Prostate Cancer Awareness and Quality Improvement Programme. More information about the programme and the Prostate Cancer Working Group can be found on the Ministry’s website If you have any queries, please contact Emma Craigie at emma_craigie@moh.govt.nz AYA Workshop registrations All those involved in delivering care to adolescents and young adults (AYA) across the cancer pathway are encouraged to register now for the AYA Standards of Care Workshop, to be held in Wellington on 27 February 2015. You can register by emailing info@ayacancernetwork.org.nz by 16 February 2015. The workshop will discuss the need for age-specific national standards of care for AYA cancer patients. The standards will be developed by a Standards of Care Working Group, will be established following the workshop. The AYA Standards of Care will include a set of prioritised statements that describe the level of service that young cancer patients aged 12 to 24 years should have access to. They will consider the complete care pathway from public health to health and social care. The Standards will help drive quality improvements for adolescent and young adults with cancer by ensuring health professionals have the best evidence based information to guide care. They will help service providers to easily assess and improve the care they provide. The Ministry of Health is currently hosting an interim website which is: www.health.govt.nz/ayacancernetwork The existing www.ayacancernetwork.org.nz website has been redirected to this site until further notice. Australasian AYA Oncology Congress Planning is also underway for the inaugural Australasian AYA Oncology Congress, which will be held in Sydney from 3 - 5 December 2015. The Congress is being run by the Youth Cancer Service in Australia and Canteen Australia. There will be split sessions focusing on medical, psycho-social and nursing themes throughout the three days. The conference is preceded by a two day Youth Cancer Summit for patients and their families. A number of presentation slots will be available for speakers from New Zealand. World Cancer Congress presentations Three World Cancer Congress 2014 electronic poster presentations highlighting key Faster Cancer Treatment initiatives can now be viewed here on the Ministry’s website. The presentations, from the Ministry’s Clinical Director for Cancer, Dr Andrew Simpson, and Cancer Services Manager Saskia Booiman, were introduced to an international audience of cancer control professionals at the Congress in Melbourne in December 2014. The presentations cover the development of New Zealand tumour standards, implementation of the 62 day Faster Cancer Treatment health target, and the Cancer Nurse Coordinator initiative. The Congress was an opportunity to achieve high-level, international exposure for New Zealand, its health system and the work that is being carried out along the cancer continuum. Dr Simpson says it was also a valuable networking opportunity and a chance to see how other countries are approaching improved cancer control. Of particular interest were the newly released cancer patient management frameworks, developed by the Department of Health in Victoria, Australia. The frameworks take a tumour stream approach to cancer care and are similar to the tumour standards developed in New Zealand. The Congress attracted more than 2700 participants, including health ministers, officials, health professionals, NGO representatives and consumers. The key focus of the conference was to arm delegates with the tools that would enable them to make a difference, to implement change and take action as part of the global fight against cancer. The Congress was preceded by the 2014 World Cancer Leaders Summit. The Summit is an annual high-level policy meeting dedicated exclusively to furthering global cancer control. The event brings together key decision makers from around the world and encourages debate on emerging issues related to cancer. The 2014 Summit focused on The Economic Case for Cancer Control. You can read a summary of the 2104 World Cancer Leaders’ Summit report Cancer Nursing Knowledge and Skills Framework The Cancer Nursing Knowledge and Skills Framework (KSF) has been endorsed by the National Nursing Consortium, the body established to endorse nursing KSFs in New Zealand. The KSF identifies the key fields of practice required to care for patients with cancer and also the core skills required at different levels of practice to provide high quality care to people with cancer. It can be used by individual nurses to guide their professional development and by DHBs and regions to inform cancer workforce planning and development. It will be circulated within the sector by the Cancer Nurses College of the New Zealand Nurses Organisation, DHB nurse educators and other senior nurse leaders, supported by the Ministry and the Medical Oncology Work Group. The Ministry would like to acknowledge Cancer Nurse Coordinator Julie Cairns and the Chair of the Cancer Nurses College, Angela Knox, who led this work, the writing reference group members, and others who supported this project. New DON for cancer Karyn Sangster, Chief Nurse Advisor Primary and Integrated Care at Counties Manukau DHB, has been nominated by the national Director of Nursing (DON) group as the new lead DON for cancer. She has wide experience in district nursing and has worked with hospice and hospital services providing home based nursing care for people with cancer. She previously worked as the Nurse Leader Primary Health Care which included Clinical Nurse Director for District Nursing. Karyn says, “Cancer affects many people of all ages and stages of life. It touches all of us at some time through our own or our family’s experience. I am hoping to influence cancer outcomes for our most vulnerable populations and improve the patient experience. “I am looking forward to continuing the great work started by Robyn Henderson from Nelson Marlborough DHB, the previous Lead DON for cancer.” Training programme for nurses performing endoscopy A training programme that will enable suitably trained and qualified nurses to perform endoscopy is expected to be up and running in the second semester of 2015. Discussions are underway between the Ministry, universities and DHBs about how and where the training programme will run. The training of nurses in endoscopy will be subject to sites being accredited for training and will take account of available supervision and support. In order to be able to perform endoscopies nurses will be required to undertake a post graduate programme which contains both theoretical and practicum components. Once the training programme is successfully completed, candidates will undergo further supervised clinical practice. The endoscopy nurse role is not seen as a substitute for the role of gastroenterologists and general surgeons. Having trained nurses available to perform endoscopies will provide additional capacity to deliver endoscopy services to patients in the future. Paediatric Oncology Shared Care Service Agreements The National Child Cancer Network (NCCN) has completed a two-year programme to implement Service Agreements with the specialist child cancer centres in Auckland and Christchurch, and the 14 shared care centres. A draft monitoring and evaluation process has been developed to allow NCCN to determine whether a service is accomplishing its goals. It identifies strengths and weaknesses, areas for revision and areas that meet or exceed expectations. The cornerstone of this review process involves systematically observing and collecting information that is used to compare what is happening now with what is expected to happen. The process captures learnings from the past three years and uses these to improve current activities and consider future service developments. Interactive web-accessed software is expected to be developed in early 2015 that will allow shared care teams to collaborate within and across DHBs to assess performance and identify development goals.