New patient details and information sheet
advertisement

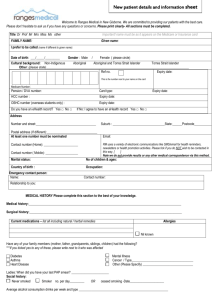
New patient details and information sheet Welcome to Ranges Medical in New Gisborne. We are committed to providing our patients with the best care. Please don’t hesitate to ask us if you have any questions or concerns. Please print clearly- All sections must be completed. First Title: Dr Prof Mr Mrs Miss Ms other Important! name must be as it appears on the Medicare or Insurance card FAMILY NAME: ……………………………………………………………….. Given name: I prefer to be called (name if different to given name): Date of birth: ___/_____/_________ Gender : Male / Female ( please circle) Cultural background: Non-Indigenous Aboriginal Aboriginal and Torres Strait Islander Torres Strait Islander Other: (please state)________________________________________________________________________________________ Ref no. Expiry date: This is the number next to your name on the card Medicare Number: Pension / DVA number: Card type: HCC number : Expiry date: OSHC number (overseas students only) : Expiry date: Do you have an eHealth record? Yes □ No □ Expiry date: If No: I agree to have an eHealth record Yes □ No □ Address Number and street:_____________________________________ Postal address (If different):_______________________________ At least one number must be nominated Contact number (Home): _____________________ Suburb : ____________ Email: RM uses a variety of electronic communications like SMS/email for health reminders, newsletters or health promotion activities. Please tick if you do NOT wish to be contacted in this way. [ ] Note we do not provide results or any other medical correspondence via this method. Contact number ( Mobile): ____________________ Marital status: No of children & ages: Country of birth : Occupation: Emergency contact person: Name: _State:______Postcode___________ Contact number: Relationship to you: MEDICAL HISTORY Please complete this section to the best of your knowledge. Medical history:______________________________________________________________________________________________ Surgical history:______________________________________________________________________________________________ Current medications – list all including natural / herbal remedies Allergies Nil known Have any of your family members (mother, father, grandparents, siblings, children) had the following? ***If you ticked yes to any of these, please write next to it who was affected Diabetes Asthma Heart Disease Mental Illness Cancer / Type______________________________________ Other (Please Specify) _______________________________ Ladies: When did you have your last PAP smear? _______________________ Social history: Never smoked Smoker no. per day_________ OR ceased smoking -Date_____________________ Average alcohol consumption drinks per week and type _______________________________________________________ TERMS AND CONDITIONS: Dear Patients, please note the following policies for this practice *** We have ZERO TOLERANCE of abuse to any of our staff either in person or on the phone. You will be asked to leave the practice*** Appointments: Our reception staff will ask you at the time of booking which doctor you would prefer to see; and the length of appointment you require. Please note a ‘standard appointment – i.e. 15 minutes’ allows for the discussion of one to two simple issues only. If you require completion of forms, have complex or several issues to discuss or need a procedure of any kind, including a pap smear, then please ask for a ‘double appointment’. This ensures there is minimal delay for other patients who are also waiting. Advising our reception staff will assist them to book the most efficient and cost effective appointment for you. Not all of our Doctors do all procedures. After hours care: For all urgent medical care after hours phone the After hours GP help line: 1800 022 222. Privacy statement and consent to release relevant health information: We require you to provide us with your personal details and a full medical history so that our Doctors can properly assess, diagnose, treat and be proactive in your health care needs. We do not share this without your consent in accordance with the National Privacy Principles (NPP) and the Privacy Act. Information regarding your medical records will only be released following a request in writing and following permission by the treating Doctor. Practice billing policy: This is a private billing practice. All consultations are payable on the day. The practice has claim facilities allowing patients to pay and then claim the Medicare rebate on site. When making your appointment please enquire with the receptionist as to the fee applicable. We provide a high standard of care in a well equipped and located practice. We only provide direct medicare billing to children under 16,DVA and aged/disability pensioners, however there is a reduced fee for those patients holding a student or health care card including Commonwealth senior health card. Your card must be shown at the visit. Saturday consultations incur a surcharge fee for all patients. Phone calls / emails: As courtesy for the patient with them, as well as privacy, our Doctors will not accept calls during consultation times. Please leave a message with the Reception staff and they will pass the message onto the Doctor for you. Our Doctors will not use email to communicate clinical or personal matters. Scripts and referrals to specialists without appointments: To maintain quality healthcare service, a consultation with the doctor is required to determine the appropriateness of each request for referral or prescription, even if it is an ongoing concern. Please note: it is illegal for Doctors to backdate referrals to specialists and medical certificates. Please do not request this. **Results: In the interest of good care, It is preferred that you make an appointment to discuss any results. However the Doctor may make alternative arrangements with you which they inform you of at the appointment. Our Reception staff are NOT able to give out result details on the phone. Reports/Paperwork: If you require reports or any kind of paperwork completed you will need to make a double appointment with the Doctor and attend in person. We will not complete any forms, including driver’s licence forms unless you attend an appointment. This kind of work is generally non Medicare rebateable- check with reception. Additional administration costs will be incurred if printing, faxing or postage is required. Late cancellations / No shows for booked appointments: We would appreciate that you give as much notice as possible of your inability to attend your appointment (no less than 4 hrs). Failure to attend appointments causes inconvenience for the Doctors and those who missed out on an appointment. Quality Care: This Practice prides itself on quality health care. If you have any questions, concerns or complaints we would be happy to hear from you or you can place a comment in our suggestion box. Please contact the Practice Manager either in person, by phone or in writing with the details above. Alternatively you can contact Health Quality and Complaints Commission at www.health.vic.gov.au/hsc/ or phone on 1300 582 113. Health Promotion and Preventative Care: Ranges Medical operates a patient reminder system and preventative medicine program for follow up and promotion of important medical issues. Please notify staff if you do not wish to be contacted via SMS or email. The practise website contains further information about our services at www.rangesmedical.com.au. Translation services: Please notify our receptionists PRIOR to the appointment if you require translation/ National Relay Services (deaf/ speech impaired) so that these can be organised. Some of our Doctors speak other languages so inform us when you book if you have special needs. I have read and understood the terms and conditions of Ranges Medical Your Signature: _____________________________________ Date: _________________ You can book online at www.rangesmedical.com.au