Program Director Information Table ()
advertisement
")
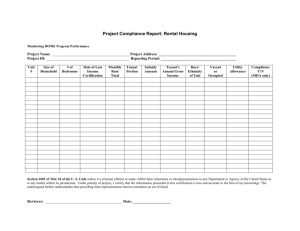
Program Director Information Complete the table below with the program director’s information. Name: Title: Credentials (MD, MPH, etc.): Address: City State: Telephone: Zip code: FAX: Email: Date the program director was first appointed: Primary specialty board certification: Most recent certification/recertification date: Secondary specialty board certification: Most recent certification/recertification date: Is the program director ABMS or RCPSC (i.e., ABPN, ABIM) certified? YES NO Is the program director UCNS certified in Neurocritical Care? YES NO YES NO YES NO YES NO Number of years spent teaching in GME in this subspecialty: Is the program director a full-time staff member of the sponsoring or primary institution? Does the program director hold a current license to practice medicine in the state of the sponsoring or primary institution? Is the program director based at primary teaching institution? Percentage of hours per week the program director spends in: Clinical (Time spent in patient care): Administration (Time spent in program administrative duties): Is the program director also the department chair? Research (Time spent completing research activities): YES Education (Time spent instructing fellows and preparing instruction materials): NO If no, chair name and credentials: Template forms must be used / Only provide requested information UCNS Program Change Program Director Information Table Page 1 of 1 2014

![Wildland Physical Fitness Test/Refresher Course Completion [DOC]](http://s3.studylib.net/store/data/006709807_1-4600d298059b59e0186774511edae385-300x300.png)