fever - Professor Fink
advertisement

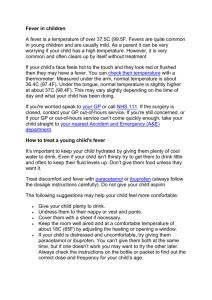
1 FEVER [from Wikipedia; http://en.wikipedia.org/wiki/Fever] Fever (also known as pyrexia, from the Greek pyretos meaning fire, or a febrile response, from the Latin word febris, meaning fever, and archaically known as ague) is a frequent medical sign that describes an increase in internal body temperature to levels above normal. Fever is most accurately characterized as a temporary elevation in the body's thermoregulatory set-point, usually by about 1–2 °C (1.8-3.6 °F). Fever is caused by an elevation in the thermoregulatory set-point, causing typical body temperature (generally and problematically considered to be 37 °C ±1 °C, or approximately 99 ±2 °F; see below for specifics) to rise, and effector mechanisms are enacted as a result. A feverish individual has a general feeling of cold despite an increased body temperature, and increases in heart rate, muscle tone and shivering, all of which are caused by the body's attempts to counteract the newly-perceived hypothermia and reach the new thermoregulatory set-point. Fever differs from hyperthermia in that hyperthermia is an increase in body temperature over the body's thermoregulatory set-point, due to excessive heat production or insufficient thermoregulation, or both. A fever is considered one of the body's immune mechanisms to attempt a neutralization of a perceived threat inside the body, be it bacterial or viral. Carl Wunderlich discovered that fever is not a disease, but the body's response to a disease. Measurement and normal variation Normally, a fever is when the core body temperature is at or over 38.0 °C (100.4 °F). At a first glance, fever is present if: Temperature in the anus (rectum/rectal) or in the ear (otic) is at or over 38.0 °C (100.4 °F) Temperature in the mouth (oral) is at or over 37.5 °C (99.5 °F) Temperature under the arm (axillary) is at or over 37.2 °C (99.0 °F) The common oral measurement of normal human body temperature is 36.8±0.7 °C (98.2±1.3 °F). This means that any oral temperature between 36.1 and 37.5 °C (96.9 and 99.5 °F) is likely to be normal. However, there are many variations in normal body temperature, and this needs to be considered when measuring for fever. The values given are for an otherwise healthy, non-fasting adult, dressed comfortably, indoors, in a room that is kept at a normal room temperature (22.7 to 24.4 °C or 73 to 76 °F), during the morning, but not shortly after arising from sleep. Furthermore, for oral temperatures, the subject must not have eaten, drunk, or smoked anything in at least the previous fifteen to twenty minutes. Body temperature normally fluctuates over the day, with the lowest levels around 4 a.m. and the highest around 6 p.m.[1] (assuming the subject follows the prevalent pattern, i.e, sleeping at nighttime and staying awake during daytime). Therefore, an oral temperature of 37.2 °C (99.0 °F) would strictly be a fever in the morning, but not in the afternoon. An oral body temperature reading up to 37.5 °C (99.5 °F) in the early/late afternoon or early/late evening also wouldn't be a fever. Normal body temperature may differ as much as 1 °F (0.6 °C) between individuals or from day to day. 1 2 In women, temperature differs at various points in the menstrual cycle, and this can be used as part of fertility awareness (although temperature is only one of the variables). Temperature is increased after eating, and psychological factors also influence body temperature. There are different locations where temperature can be measured, and these differ in temperature variability. Tympanic membrane thermometers measure radiant heat energy from the tympanic membrane (infrared). These may be very convenient, but may also show more variability. Children develop higher temperatures with activities like playing, but this is not fever because their set-point is normal. Elderly patients may have a decreased ability to generate body heat during a fever, so even a lowgrade fever can have serious underlying causes in geriatrics. Fever is usually accompanied by sickness behavior which consists of lethargy, depression, anorexia, sleepiness, hyperalgesia, and the inability to concentrate.[2][3][4] Mechanism Temperature is ultimately regulated in the hypothalamus. A trigger of the fever, called a pyrogenin, causes a release of prostaglandin E2 (PGE2). PGE2 then in turn acts on the hypothalamus, which generates a systemic response back to the rest of the body, causing heatcreating effects to match a new temperature level. Hyperthermia: Characterized on the left. Normal body temperature (thermoregulatory set-point) is shown in green, while the hyperthermic temperature is shown in red. As can be seen, hyperthermia can be conceptualized as an increase above the thermoregulatory set-point. Hypothermia: Characterized in the center: Normal body temperature is shown in green, while the hypothermic temperature is shown in blue. As can be seen, hypothermia can be conceptualized as a decrease below the thermoregulatory set-point. Fever: Characterized on the right: Normal body temperature is shown in green. It reads "New Normal" because the thermoregulatory set-point has risen. This has caused what was the normal body temperature (in blue) to be considered hypothermic. 2 3 Pyrogens A pyrogen is a substance that induces fever. These can be either internal (endogenous) or external (exogenous) to the body. Endogenous Cytokines (especially interleukin 1) are a part of the innate immune system, are produced by phagocytic cells, and cause the increase in the thermoregulatory set-point in the hypothalamus. Other examples of endogenous pyrogens are interleukin 6 (IL-6), and tumor necrosis factor-alpha. These cytokine factors are released into general circulation where they migrate to the circumventricular organs of the brain due to easier absorption caused by the blood-brain barrier's reduced filtration action there. The cytokine factors then bind with endothelial receptors on vessel walls, or interact with local microglial cells. When these cytokine factors bind, the arachidonic acid pathway is then activated. Exogenous Gram-negative bacteria contain a lipopolysaccharide (LPS) in the cell wall. An immunological protein called lipopolysaccharide-binding protein (LBP) binds to LPS. The LBP–LPS complex then binds to the CD14 receptor of a nearby macrophages. This binding results in the synthesis and release of various endogenous cytokine factors, such as interleukin 1 (IL-1), interleukin 6 (IL-6), and the tumor necrosis factor-alpha. In other words, exogenous factors cause release of endogenous factors, which, in turn, activate the arachidonic acid pathway. Prostaglandin (PGE2) release PGE2 release comes from the arachidonic acid pathway. This pathway (as it relates to fever), is mediated by the enzymes phospholipase A2 (PLA2), cyclooxygenase-2 (COX-2), and prostaglandin E2 synthase. These enzymes ultimately mediate the synthesis and release of PGE2. PGE2 is the ultimate mediator of the febrile response. The set-point temperature of the body will remain elevated until PGE2 is no longer present. PGE2 acts on neurons in the preoptic area (POA) of the Hypothalamus through the prostaglandin E receptor 3 (EP3). EP3-expressing neurons in the POA innervate the dorsomedial hypothalamus (DMH), the rostral raphe pallidus nucleus in the medulla oblongata (rRPa) and the paraventricular nucleus (PVN) of the hypothalamus . Fever signals sent to the DMH and rRPa lead to stimulation of the sympathetic output system, which evokes non-shivering thermogenesis to produce body heat and skin vasoconstriction to decrease heat loss from the body surface. It is presumed that the innervation from the POA to the PVN mediates the neuroendocrine effects of fever through the pathway involving pituitary gland and various endocrine organs. Hypothalamus response The brain ultimately orchestrates heat effector mechanisms via the autonomic nervous system. These may be: Prevention of heat loss, such as cutaneous vasoconstriction. Increased heat production by shivering and hormones like epinephrine (Adrenalin). The autonomic nervous system may also activate brown adipose tissue to produce heat (non-exerciseassociated thermogenesis, also known as non-shivering thermogenesis), but this seems mostly important for babies. Increased heart rate and vasoconstriction contribute to increased blood pressure in fever. 3 4 Types According to one common rule of thumb, fever is generally classified for convenience as an anal (core) temperature of: Fever classification Grade °C °F low grade 38–39 100.4–102.2 moderate 39–40 102.2–104.0 high-grade 40–41.1 104.0–106.0 hyperpyrexia >41.1 >106.0 The last is a medical emergency because it approaches the upper limit compatible with human life. If the temperature is taken by another route (mouth, ear, armpit), then the reading needs to be converted to the equivalent core body temperature. Most of the time, fever types can not be used to find the underlying cause. However, there are specific fever patterns that may occasionally hint the diagnosis: Pel-Ebstein fever: A specific kind of fever associated with Hodgkin's lymphoma, being high for one week and low for the next week and so on. However, there is some debate as to whether this pattern truly exists.[5] Continuous fever: Temperature remains above normal throughout the day and does not fluctuate more than 1 °C in 24 hours, e.g. lobar pneumonia, typhoid, urinary tract infection, brucellosis, or typhus. Typhoid fever may show a specific fever pattern, with a slow stepwise increase and a high plateau. Intermittent fever: Elevated temperature is present only for some hours of the day and becomes normal for remaining hours, e.g. malaria, kala-azar, pyaemia, or septicemia. In malaria, there may be a fever with a periodicity of 24 hours (quotidian), 48 hours (tertian fever), or 72 hours (quartan fever, indicating Plasmodium malariae). These patterns may be less clear in travelers. Remittant fever: Temperature remains above normal throughout the day and fluctuates more than 1 °C in 24 hours, e.g. infective endocarditis. A neutropenic fever, also called febrile neutropenia, is a fever in the absence of normal immune system function. Because of the lack of infection-fighting neutrophils, a bacterial infection can spread rapidly and this fever is therefore usually considered a medical emergency. This kind of fever is more commonly seen in people receiving immune-suppressing chemotherapy than in apparently healthy people. Febricula[6] is a mild fever of short duration, of indefinite origin, and without any distinctive pathology. Causes Fever is a common symptom of many medical conditions: Infectious disease, e.g. influenza, common cold, HIV, malaria, infectious mononucleosis, or gastroenteritis Various skin inflammations, e.g. boils, pimples, acne, or abscess Immunological diseases, e.g. lupus erythematosus, sarcoidosis, inflammatory bowel diseases Tissue destruction, which can occur in hemolysis, surgery, infarction, crush syndrome, rhabdomyolysis, cerebral hemorrhage, etc. Drug fever 4 5 o directly caused by the drug, e.g. lamictal, progesterone, or chemotherapeutics causing tumor necrosis o as an adverse reaction to drugs, e.g. antibiotics or sulfa drugs. o after drug discontinuation, e.g. heroin or fentanyl withdrawal Cancers, most commonly renal cancer and leukemia and lymphomas Metabolic disorders, e.g. gout or porphyria Thrombo-embolic processes, e.g. pulmonary embolism or deep venous thrombosis Persistent fever which cannot be explained after repeated routine clinical inquiries, is called fever of unknown origin. Usefulness of fever There are arguments for and against the usefulness of fever, and the issue is controversial. [7][8] There are studies using warm-blooded vertebrates[9] and humans[10] in vivo, with some suggesting that they recover more rapidly from infections or critical illness due to fever. A Finnish study suggested reduced mortality in bacterial infections when fever was present. [11] Theoretically, fever can aid in host defense.[7] There are certainly some important immunological reactions that are sped up by temperature, and some pathogens with strict temperature preferences could be hindered.[12] Fevers may be useful to some extent since they allow the body to reach high temperatures, causing an unbearable environment for some pathogens. White blood cells also rapidly proliferate due to the suitable environment and can also help fight off the harmful pathogens and microbes that invaded the body. Research[13] has demonstrated that fever has several important functions in the healing process: increased mobility of leukocytes enhanced leukocytes phagocytosis endotoxin effects decreased increased proliferation of T Cells[14] enhanced activity of interferon[14] Treatment Fever should not necessarily be treated. Fever is an important signal that there's something wrong in the body, and it can be used to govern medical treatment and gauge its effectiveness. Moreover, not all fevers are of infectious origin. Even when treatment is not indicated, however, febrile patients are generally advised to keep themselves adequately hydrated, as the dehydration produced by a mild fever can be more dangerous than the fever itself. Water is generally used for this purpose, but there is always a small risk of hyponatremia if the patient drinks too much water. For this reason, some patients drink sports drinks or electrolyte-replacing products designed specifically for this purpose. Most people take medication against fever because the symptoms cause discomfort. Fever increases heart rate and metabolism, thus potentially putting an additional strain on elderly patients, patients with heart disease, etc. This may even cause delirium. Therefore, potential benefits must be weighed against risks in these patients. In any case, fever must be brought under control in instances when fever escalates to hyperpyrexia and tissue damage is imminent. 5 6 Treatment of fever is normally done by lowering the set-point, but facilitating heat loss may also be effective. The former is accomplished with antipyretics such as acetominophen (Tylenol) or ibuprofen (Advil; Motrin). Heat loss may also be accomplished by heat conduction, convection, radiation, or evaporation (sweating, perspiration), or a combination of these. 1. ^ Body Temperature 2. ^ Hart, B. L. (1988) "Biological basis of the behavior of sick animals". Neurosci Biobehav Rev. 12: 123-137.PubMed 3. ^ Johnson, R. (2002) "The concept of sickness behavior: a brief chronological account of four key discoveries". Veterinary Immunology and Immunopathology. 87: 443-450 PubMed 4. ^ Kelley, K. W., Bluthe, R. M., Dantzer, R., Zhou, J. H., Shen, W. H., Johnson, R. W. Broussard, S. R. (2003) "Cytokine-induced sickness behavior". Brain Behav Immun. 17 Suppl 1: S112-118 PubMed 5. ^ Hilson, A.J.W.; DiNubile, M.J. (1995-07-06), "Correspondence", New England Journal of Medicine 333: 66–67, doi:10.1056/NEJM199507063330118, PMID 7777006, http://content.nejm.org/cgi/content/short/333/1/66, retrieved on 2008-03-18. They cite Richard Asher's lecture Making Sense (Lancet, 1959, 2, 359) 6. ^ Febricula, definition from Biology-Online.org, consulted June 7, 2006 http://www.biologyonline.org/dictionary/Febricula 7. ^ a b Schaffner A. Fever—useful or noxious symptom that should be treated? Ther Umsch 2006; 63: 185-8. PMID 16613288 8. ^ Soszynski D. The pathogenesis and the adaptive value of fever. Postepy Hig Med Dosw 2003; 57: 531-54. PMID 14737969 9. ^ Su, F.; Nguyen, N.D.; Wang, Z.; Cai, Y.; Rogiers, P.; Vincent, J.L. Fever control in septic shock: beneficial or harmful? Shock 2005; 23: 516-20. PMID 15897803 10. ^ Schulman, C.I.; Namias, N.; Doherty, J., et al. The effect of antipyretic therapy upon outcomes in critically ill patients: a randomized, prospective study. Surg Infect (Larchmt) 2005; 6:369-75. PMID 16433601 11. ^ Rantala S, Vuopio-Varkila J, Vuento R, Huhtala H, Syrjänen J. Predictors of mortality in betahemolytic streptococcal bacteremia: A population-based study. J Infect. 2009 Mar 2. PMID 19261333 12. ^ Fischler, M.P.; Reinhart, W.H. Fever: friend or enemy? Schweiz Med Wochenschr 1997; 127: 864-70. PMID 9289813 13. ^ Craven, R and Hirnle, C. (2006). Fundamentals of nursing: Human health and function. Fourth edition. p. 1044 14. ^ a b Lewis, SM, Heitkemper, MM, and Dirksen, SR. (2007). Medical-surgical nursing: Assessment and management of clinical problems. sixth edition. p. 212 15. ^ Craven ,R and Hirnle,C. (2006). "Fundamentals of nursing:Human health and function. Forth edition.". Antipyretics 11 (7-8): 1044. PMID 15636181. Further reading Rhoades, R. and Pflanzer, R. Human physiology, third edition, chapter 27 Regulation of body temperature, p. 820 Clinical focus: pathogenesis of fever. ISBN 0-03-005159-2 Kasper, D.L.; Braunwald, E.; Fauci, A.S.; Hauser, S.L.; Longo, D.L.; Jameson, J.L. Harrison's Principles of Internal Medicine. New York: McGraw-Hill, 2005. ISBN 0-07-139140-1. External links What to do if your child has a fever from Seattle Children's Hospital Fever and Taking Your Child's Temperature US National Institute of Health factsheet 6 7 Fever and Infections Although it varies throughout the day, many people believe that the body’s normal temperature is about 98.6° F, and that fever (when the temperature climbs higher) is the body’s normal reaction to inflammation or infection. Although this is usually the case, many other conditions such as autoimmune diseases, cancer, and heart attack, may cause a low-grade fever (99 to 100° F). If you develop a fever that persists that does not seem to be caused by an infection, see a doctor to investigate other causes. An infection caused by a virus is commonly referred to as a “cold” or “flu.” When a common virus infects the body, symptoms typically last from three or four days to two weeks, and may include the following: headache, cough, abdominal pain, rash, diarrhea, joint pain, nausea, vomiting, sore throat, earache, sinus pressure, and/or runny nose. A virus does not respond to antibiotics and is treated with medications aimed to lessen symptoms. That is, a runny nose is treated with a decongestant, a cough with dextromethorphan, a headache with acetominophen, diarrhea with Immodium D, sore throat with salt water gargle, etc. You can’t do much to kill the virus; you must simply wait for your body to expel the unwanted intruder. Bacterial Infections A fever may also be caused by a bacterial illness. Bacterial infections can be much more severe as bacteria can cause organ damage or other severe complications. Common bacterial infections can be related to the following conditions: Otitis Media (bacterial inner ear infection) Conjunctivitis/Pink Eye (bacterial infection of the superficial eye) Sinusitis (bacterial sinus infection) Strep throat or pharyngitis (bacterial throat infection) Cellulitis (bacterial skin infection) Septic Arthritis (bacterial joint infection) Pneumonia (bacterial lung infection) Acute Bronchitis (bacterial infection of the lung passageways) Acute Cholecystitis (bacterial infection of the gall bladder) Intra-abdominal Abscess (bacterial collection located in the abdominal cavity) Abscess general (bacterial collection located anywhere in the body under the skin) Pyelonephritis (bacterial infection of the kidney) Urinary Tract Infection (bacterial bladder infection) Urethritis (bacterial infection of the urethra) Pelvic Inflammatory Disease (bacterial infection of the female reproductive organs) It is not easy to tell if an infection is viral or bacterial. Many times, they will both give you the symptoms you have described. Acute bacterial infections are more likely to cause a fever. Chronic sinusitis is not. Some viral infections have a fever, others do not. Viral infections are far more common in the winter, usually go away in 3 to 7 days and are mostly an annoyance. Bacterial infections may not get better without antibiotics and make you feel really badly. There are medications that loosen the congestion and make it easier to cough up. They are medications that contain guiafenesin. 7