Research of accommodative microfluctuations caused by visual
advertisement

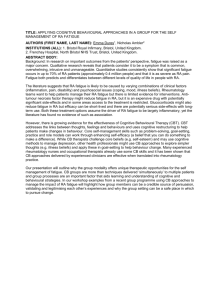
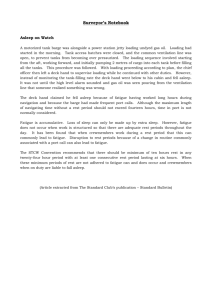
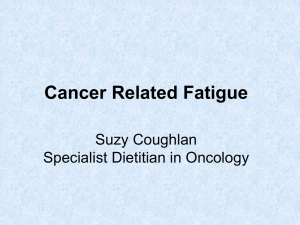
Research of accommodative microfluctuations caused by visual fatigue based on liquid crystal and laser displays Wei-De Jeng,1 Yuan Ouyang,2 Ting-Wei Huang,1 Jeng-Ren Duann,3 Jin-Chern Chiou,1,3 Yu-Shun Tang,1 and Mang Ou-Yang1,* 1 Department of Electrical and Computer Engineering, National Chiao Tung University, Hsinchu 30010, Taiwan 2 Department of Electrical Engineering, Chang Gung University, Kwei-Shan, Tao-Yuan 33302, Taiwan 3 Biomedical Engineering R&D Center, China Medical University, Taichung 40402, Taiwan *Corresponding author: oym@cn.nctu.edu.tw Received 5 May 2014; revised 8 July 2014; accepted 13 July 2014; posted 14 July 2014 (Doc. ID 211202); published 14 August 2014 Different levels of visual fatigue in the human eye depend on different color-formation methods and image quality. This paper uses the high-frequency component of the spectral power of accommodative microfluctuations as a major objective indicator for analyzing the effects of visual fatigue based on various displays, such as color-formation displays and 3D displays. Also, a questionnaire is used as a subjective indicator. The results are that 3D videos cause greater visual fatigue than 2D videos (p < 0.001), the shutter-type 3D display causes visual fatigue more than the polarized type (p ˆ 0.012), the display of the time-sharing method causes greater visual fatigue than the spatial-formation method (p ˆ 0.008), and there is no significance between various light source modules of displays (p ˆ 0.162). In general, people with normal color discrimination have more visual fatigue than those with good color discrimination (p < 0.001). Therefore, this paper uses the high-frequency component of accommodative microfluctuations to evaluate the physiological stress or strain by overexerting the visual system, and can compare the level of visual fatigue between various displays. © 2014 Optical Society of America OCIS codes: (120.2040) Displays; (330.1720) Color vision; (330.4595) Optical effects on vision; (330.7310) Vision. http://dx.doi.org/10.1364/AO.53.000H76 1. Introduction Currently, visual fatigue is a common affliction because people frequently view displays for a long time. As these stimulate the eyes continuously, they also cause a great number of visual problems. Therefore, it is worth discussing the effects of such displays on people’s vision [1]. From a visual standpoint, displays can be divided into three parts: color-formation methods, 3D technologies, and different light sources. In a study on the effects of visual fatigue from various colors and image appearances, it is necessary to find a stressfree way for people to view things. Color-formation methods involve time sharing and spatial formation [2], 3D display technology has shutter and polarized type, and the light source module usually includes a light-emitting diode (LED) and a laser diode (LD). To date, the color breakup from the timesharing method has been known to cause visual fatigue in the human eye according to [3–9], and it is common for 3D displays to make people feel tired. Therefore, the main focus of this research is to investigate the degree of visual fatigue based on various displays. To solve these problems, it is necessary to find a suitable indicator for evaluating the effects of various displays on the human eye. There are various indicators for evaluating visual fatigue. A subjective method such as a questionnaire could be used, and some objective methods, such as critical fusion frequency (CFF) [10], are suitable in certain cases. This study proposes to evaluate visual fatigue through accommodative microfluctuations of the ciliary body. There is now a similar evaluation method in medical research on visual fatigue called the high-frequency component (HFC) of accommodative microfluctuations. For instance, Gray et al. [11] used the lowfrequency component (LFC) and HFC to analyze visual variations after using visual display terminals (VDTs). The HFC’s spectral power was analyzed by Kajita et al. [12]. It showed that visual fatigue could indeed be measured and quantified. This method can effectively and objectively determine whether subjects are suffering from visual fatigue. Therefore, this research uses it as an indicator for visual fatigue. In visual fatigue research, there are various and extensive indicators and measuring methods, which can be divided into five types: (1) the measurement of the oculomotor systems including eye movement velocity, accommodation power, convergence, viewing distance, pupil diameter, and blinking; (2) the measurement of visual acuity including visual acuity and CFF; (3) the measurement of performance of visual tasks, i.e., recognition speed and error detection rate; (4) the report of asthenopia symptoms; and (5) brain activity measurements such as functional magnetic resonance imaging (FMRI), magneto encephalography (MEG), and electroencephalography (EEG) for observing neural activity affected by visual fatigue, both temporally (MEG and EEG) and spatially (FMRI) [13–18]. There are objective or subjective indicators according to Chi and Lin [10], such as accommodation power, pupil diameter, visual acuity, eye movement velocity, CFF, the subjective rating of visual fatigue, and visual task performance. The subjective rating for visual fatigue is an indicator related to a judgment on the subjects’ level of visual fatigue; it will have more inaccuracies while subjects were disturbed by the response of the visual cortex neural activity. Overall, not all of the visual fatigue Table 1. Indicators Accommodation power Pupil diameter Visual acuity Comparisons between Seven Indicators for Evaluating the Level of Visual Fatigue [10] Advantages High sensitivity to near work High sensitivity to dynamic condition Suitability to evaluation of whole visual system High sensitivity to dynamic condition Eye movement velocity Critical fusion frequency Subjective rating of visual fatigue Visual task performance measurement indicators have high sensitivity in every experiment. There are different restrictions or conditions in the different experiments, as shown in Table 1. The indicators for evaluating visual fatigue, accommodation power, pupil diameter, visual acuity, eye movement velocity, CFF, subjective rating of visual fatigue, visual task performance, and brain activity measurements have their own limitations. For instance, accommodation power is best used to evaluate visual fatigue because the lens curvature becomes larger in close work and fatigue occurs over long periods of time. Work station illumination is different from that of a target or dynamic information, and the iris’s sphincter muscle, as a pupil constrictor, has to control the amount of light entering the eyes. Hence, the pupil’s diameter is a suitable evaluator under these conditions. Moreover, the subjective rating does depend on the participants’ psychological and physiological feelings, and hence has good face validity yet large intersubject variations. Therefore a large number of participants is required to yield reliable results from the subjective ratings. An appropriate evaluation indicator should be chosen to investigate the relationship between the color-formation methods, 3D technologies, different light source modules, and visual fatigue. This indicator needs to satisfy every condition to compare these relationships. This study uses dynamic information as the experimental tool since displays are used to show the dynamics of daily life. The moving frames stimulate eyesight. Moreover, it is better to use multiple visibility ranges than others that just explore the influence of different ranges at short distances. From the indicators mentioned in Table 1, accommodation and CFF are highly sensitive at short distances and low brightness contrast, respectively; both are unsuitable. Second, the pupil’s diameter is so easily influenced by exterior stimuli that it is difficult to control variations. The speed of eye movements can be adopted in a dynamic environment, but existing measurement methods are limited. Some instruments cause the eyes discomfort, and the measurement of movement time is inaccurate. Because of such difficulties, this study uses an advanced evaluation method of visual fatigue, which is accommodative microfluctuations. The accommodative microfluctuations can reflect the High sensitivity to contrast work in low brightness High face validity and easy application Direct and indirect show of visual fatigue Disadvantages Long time for stimulation Unsuitability for static condition and many limitations Long time for stimulation Unsuitability for static condition and limitations of device Long time for stimulation Low objectivity Many limitations to apply Table 2. Abbreviation Displays and Operation Modes of the Display Used in Experiment Luminance …cd∕m2 † Screen Size (inches) S3D 172.4 40 S2D 172.4 40 P3D 234.9 42 P2D 234.9 42 LP 250.7 44 Display Type Shutter 3D LCD under 3D mode Shutter 3D LCD under 2D mode Polarized 3D LCD under 3D mode Polarized 3D LCD under 2D mode Laser projector ciliary body’s response. Because this indicator is not restricted by the conditions and relates to the subjects’ physiology and the ciliary body microfluctuations, it can be more accurate when evaluating visual fatigue. Finally, this research combines the results of questionnaire tests to compare the relation between subjective and objective rating methods. 2. Accommodative Microfluctuations The eye lens’s curvature changes its dioptric ability to maintain a clear image of objects as the distance varies. This self-adjusting mechanism on the optical system is called accommodation, which varies from 0.01 m (10 D) to infinity (0 D) for normal and young eyes. The ciliary body around the lens controls the curvature of the lens by contracting and relaxing, and has a large number of suspensor ligaments connected to the lens. Theoretically, the ciliary body should be in static state when looking at an object, but actually it adjusts repeatedly instead of adjusting immediately to a suitable curvature during the accommodation process. As a result, it becomes unstable and fluctuates when focusing on an object, and the fluctuation frequency is around a few hertz. These are called accommodative microfluctuations [10,11,18–24]. As people with normal vision look at a close object, the activity of the ciliary body is relatively low when compared to viewing a far object. When people with visual fatigue look at a far object, the activity of the ciliary body is significantly higher compared to normal vision, and remains high while looking at short distances, but it is not obvious when compared to people with normal vision [11,20]. When reading at short distances, people with myopia exhibit a significant increase in the power of accommodative microfluctuations [25]. The behavior of accommodative microfluctuations is complex, without rules, and nonlinear in time [1]; however, regular patterns exist while transferring the waveform into the frequency domain. According to the waveform, accommodative microfluctuations consist of two components: LFC and HFC; the former is defined below 0.6 Hz, and the latter between 1.0 and 2.3 Hz [11,12,18,21,22]. The following section will introduce the relation between accommodative microfluctuations and these two components. Accommodative microfluctuations may be affected by the distance of the target [20,26–28], the pupil diameter [24,29–31], the form of the target [32,33], the luminance of the target [11,34,35], the eye’s age, astigmatism [36], visual fatigue [12,20,37,38], biomonocular observation of the target [30,37], and artifacts such as cardiopulmonary signals [39–41] or other rhythmical physiological systems. Neurological control also affects the LFC’s wavelength, and arterial signals correlate highly to the HFC [11,21]. However, the effect by the pupil’s diameter is the most obvious. The pupil changes with light, and when the pupil’s diameter is smaller, the HFC fluctuations are imperceptible, although the LFC increases; when the diameter increases, the HFC fluctuations become obvious and the LFC decreases [21]. Geacintov and Peavler (1974) reported that there is a connection between pupil instability and visual fatigue [42]. Some recent research has studied eye variations and visual fatigue after viewing VDTs; it indicates the close connection between the pupil’s variations and accommodative microfluctuations [11]. It showed that patients with asthenopia can indeed be diagnosed from changes in the HFC [12]. Suzuki et al. (2001) tried using a color code to show the position of targets, the accommodative response amplitude, and the HFC value as figures [21]. While viewing a distant stable target, the result shows that a normal subject’s HFC is about 50–60, labeled in green, while a subject with asthenopia is above 60, labeled in red. After combining these results, it is concluded that the ciliary body’s tension is low when viewing far objects, so its variation is large if visual fatigue occurs, and slight with short distances. Thus, the ciliary body’s tension is recognized by the HFC variations, and subjects are assessed to see whether they suffer from visual fatigue. As mentioned before, there is a high correlation between the HFC and cardiopulmonary signals; therefore, eyes suffering from visual fatigue can be evaluated by the HFC variations because physiological aspects influence cardiopulmonary signals. In addition to measuring accommodative microfluctuations and calculating the HFC, the device can be used to measure accommodation power, which has been more functional than optometers in the past. 3. Methodology and Experiments In order to research the effects on the human eye by various displays, three displays of different types were used in the experiment: a shutter-type 3D liquid crystal display (LCD), a polarized-type 3D LCD, which are using both an LED as a backlight module and the color-formation method in spatial formation. A laser projector uses a mix of LED and LD for the light source module; the color-formation method is a time-sharing method. Also, both of the 3D LCDs can change to the 2D display mode. The resolution of the 3D LCD is full HD (1920 × 1080), and the laser projector is XGA (1024 × 768). Table 2 shows the display’s luminance specifications under different display types; all the luminance values of display types were measured from a white screen. In order to express the display type in a simple way, the abbreviations are defined under different display types. An auto refract-keratometer Righton Speedy-K can record a subject’s ciliary muscle microfluctuations through built-in targets. Subjects should gaze steadily at a target, which varies from ‡ 0.5 to −3.0 D with 0.5 D step, for a total of eight targets. The software “MF-1” is then applied to analyze the data, and calculations are made by the fast Fourier transform (FFT). The mean spectral power is integrated into the frequency domain between 1 and 2.3 Hz, and used to evaluate the research’s visual fatigue level because it indicates ciliary body fluctuations. In total, there are six HFC data for each target. The Farnsworth–Munsell 100-Hue Test is a direct device used to examine chromatic discrimination, and is used by this research as a basis for grouping subjects according to their chromatic discrimination abilities. In the standard reference, an error score less than 20 is good in chromatic discrimination, between 20 and 100 is normal, and more than 100 is bad [43]. In this study, the subjects will be grouped into different chromatic discrimination abilities according to the standard reference. Figure 1 shows the flow chart for the experiment; the whole experiment is carried out in a dark room. Before viewing video subjects were asked about such discomforts as eyestrain, headache, or body stiffness; then they rested for 5 min to prevent affecting the test from prior fatigue. In the beginning of the experiment, all subjects participated two times in the hue test under a D65 light source and then divided into two groups: good chromatic discrimination and normal chromatic discrimination. After finishing the hue test, subjects were asked to take a 5 min break to relax their eyes, and then the dipoters of the left eye were measured by the auto refract-keratometer for 1 min, 45 s to get the HFC data; then the subjects filled out the questionnaire as shown in Table 3 [44,45]. The subject gave a score for each symptom before and after viewing videos; scores 1 to 5 indicate no feeling, slightly, medium, deep, and serious, respectively. Upon completing the questionnaire on 15 symptoms, subjects viewed the video sitting on a chair at about a 2 m distance from the screen for 15 min. This experiment chose two videos, and each video was separated into four parts and randomly displayed on a shutter 3D LCD under 2D and 3D mode, a polarized 3D LCD under 2D and 3D mode, and a laser projector. After viewing the videos, the eye measurements were taken again, and the questionnaire was filled in immediately afterwards. In order to prevent a large number of subjects from suffering from an accumulation of tiredness, each person was tested in only one mode per day, and each person was tested four times in Fig. 1. Flow chart of experimental process. each mode; there are five modes in total in the experiments. Hence, it takes 20 days to finish a round for each person. Finally, after all the data are collated and analyzed, the HFC is used as the major indicator. Table 3. Questionnaire for Evaluating the Level of Visual Fatigue by Different Symptoms Questions 1. Do you feel eyestrain?eyestrain 2. Do your eyes feel dry?dry eyes 3. Do you feel the environment too bright is too bright? 4. Does your eyelid twitch?eyelid twitching 5. Do you feel stress infeeling of pressure your eyes?in the eyes 6. Do you feel ache behindache behind the the eyes?eyes 7. Do you feel everything isblurred vision blurred? 8. Do you have a headache?headache 9. Does your head feel heavy? head feels heavy 10. Do you have a headachehead hurts when when shaking your head?shaken 11. Do you feel dazed?dazed feeling 12. Do you feel irritated?irritated feeling 13. Do your shoulders feel stiff? stiff shoulders 14. Do you want to sleep?sleepy feeling 15. Do you feel it is difficult to difficulty pay attention?concentrating Symptoms Before After Table 5. The questionnaire is used as a reference indicator for the analysis and discussion. 3D 2D LP 2D S3D P3D Now the HFC is measured before and after viewing videos, and the level of visual fatigue can be defined by ΔHFC. The ΔHFC means the difference between the HFC, which is measured before and after viewing videos; it means ΔHFC ˆ HFCafter −HFCbefore . Each subject is tested four times in each mode. Each time is measured six HFCs at each target, and there are eight targets in each measurement; thus, each subject has 6 × 8 × 4 ˆ 192 data for each mode. All the data from this procedure are labeled with different variables, and the analysis of variance (ANOVA) and one-tailed t-test are used to find what effects the different color-formation methods, 3D technologies, and lighting sources have on visual fatigue. There are 30 subjects in total, and the mean age is 25.0 3.8. Different chromatic discrimination abilities are considered to determine the relationship between them and visual fatigue. Besides, the ranking for mean scores is applied to analysis of questionnaires for finding what effects the different color-formation methods, 3D technologies, and lighting sources have on visual fatigue. Table 4 shows the t-test results and compares the level of visual fatigue between each mode. Standard error (SE) is the standard deviation of the sample mean. SE is computed by the sample standard deviation divided by the square root of the sample size. The asterisk indicates that the t-test result is significant (p value <0.05). The results indicate that the ΔHFC by S3D is much larger than one by S2D (p < 0.001) and the ΔHFC by P3D is much more than the one by P2D (p ˆ 0.035). Therefore, the subjects’ Variables (Mode) * t-Test Results for Each Mode Mean ΔHFC (SE) S3D S2D S3D P3D P3D P2D S2D P2D S3D P2D P3D S2D S3D LP P3D LP S2D LP P2D LP 1.43 0.63 1.43 0.87 0.87 0.44 0.63 0.44 1.43 0.44 0.87 0.63 1.43 1.03 0.87 1.03 0.63 1.03 0.44 1.03 (0.179) (0.167) (0.179) (0.172) (0.172) (0.165) (0.167) (0.165) (0.179) (0.165) (0.172) (0.167) (0.179) (0.171) (0.172) (0.171) (0.167) (0.171) (0.165) (0.171) p Value <0.001* 0.012* 0.035* 0.215 <0.001* 0.317 (0.124) (0.118) (0.171) (0.118) (0.179) (0.172) <0.001* 0.008* 0.012* ciliary body is tenser and more fatigued when viewing the 3D videos than when viewing the 2D videos. The subjects’ ΔHFC is higher when viewing S3D than P3D (p ˆ 0.012), so the shutter-type display strains the subjects’ ciliary body more than the polarized system does. There is no significant difference between viewing S2D and P2D (p ˆ 0.215), possibly because both of them are in the 2D mode using a spatial formation. Finally, the ΔHFC of watching LP is significantly different to S2D (p ˆ 0.045) and P2D (p ˆ 0.006), but not to P3D (p ˆ 0.257). The ciliary body tension is caused more by S3D than LP (p ˆ 0.052), but LP is more than S2D (p ˆ 0.045) and P2D (p ˆ 0.006). The latter result indicates that time sharing causes the human eye to experience more fatigue than the spatial-formation method does. Table 5 shows the t-tests results for the 3D and 2D modes; it shows that the 3D mode causes much more serious tension than 2D (p < 0.001). Thus, subjects strained the ciliary body more while viewing the 3D videos than the 2D videos. The t-tests results for the LP and LCD show that subjects have much more tension caused by the LP (p ˆ 0.008), indicating that the time-sharing method causes more fatigue to the ciliary body than the spatial formation does. For the two kinds of 3D displays, subjects who viewed 3D videos with shutter glasses had significant ciliary body tension compared to those wearing polarized glasses (p ˆ 0.012). Table 6 shows that the two kinds of light sources have no significant difference when compared to each other (p ˆ 0.162). It indicates that the LED backlight and LED mixed with LD light source module have the same effect on fatigue and the ciliary body. In order to investigate the relation between chromatic discrimination ability and visual fatigue, all subjects were grouped into two groups, and analyses of chromatic discrimination in each mode were conducted to understand how it affects visual fatigue. From Table 7, some first test results with the subjects have significant differences compared to 0.052 0.257 Table 6. 0.006* t-Test for LED Backlight and Mixed LED and LD Light Source Mean ΔHFC (SE) Variables Light sources A significant result (p < 0.05). 1.15 0.53 1.03 0.53 1.43 0.87 p Value A significant result (p < 0.05). 0.045* * Mean ΔHFC (SE) Variables (Mode) 4. Analysis and Results Table 4. t-Test for 3D/2D, LP/LCD, and Shutter/Polarized LED LED+LD 0.84 (0.085) 1.03 (0.171) p Value 0.162 Table 7. Subjects 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 Chromatic Discrimination Ability of All Subjects Total Error Scores 12, 08 16, 04 40, 08, 20 28, 24 48, 16, 20 36, 12 96, 40, 44 56, 20, 28 12, 24 32, 20 40, 12, 24 20, 20 20, 20 88, 88 40, 08, 20 20, 28 20, 20 28, 16 36, 32 32, 36 24, 16 08, 18 16, 24 08, 20 16, 28 72, 48, 32 12, 08 52, 36 24, 16 08, 12 Mean Error Scores 10 10 14 26 18 24 42 24 18 26 18 20 20 88 14 24 20 22 34 34 20 13 20 14 22 40 10 44 20 10 Table 8. Chromatic Discrimination good good good normal good normal normal normal good normal good normal normal normal good normal normal normal normal normal normal good normal good normal normal good normal normal good the second test results; this situation should use hypothesis testing to filter out the singular data. We compute the difference of two hue test scores (second test score minus first test score) in all normal subjects, so the total score difference is 23 (because seven subjects’ hue tests the first time may be wrong due to unfamiliarity). The mean score difference is 7.74, and the standard deviation is 5.9. Then we can find all seven subjects’ score differences are successful to reject the null hypothesis, which means if the score of the first two tests has a significant difference, this situation has very low probability of occurrence. Hence, the subject should do the third hue test. Also, we can find that after the subject finishes the third test, the score difference (between the second and third tests) becomes smaller than the score difference between the first two tests. This is why we delete the first test score. We also asked those subjects about the first hue test, and subjects said that because this test only allows a few seconds to finish, they became very anxious when the time was running, so they did not perform well on the first test, but they felt better on the second test. Finally, the numbers of subjects are 11 and 19 in good and normal chromatic discrimination, respectively. Table 8 shows a detailed analysis of chromatic discrimination power. All mode means all the 3D, 2D, and LP samples were combined together. An t-Test for Chromatic Discrimination under Each Condition Variables (Chromatic Discrimination) All Mean ΔHFC (SE) good normal good normal good normal good normal good normal good normal good normal 3D 2D S3D P3D LCD p Value <0.001* 0.64 (0.097) 1.24 (0.124) 0.87 (0.144) 1.8 (0.240) 0.56 (0.123) 0.91 (0.157) 1.15 (0.226) 1.86 (0.290) 0.65 (0.219) 1.21 (0.276) 0.36 (0.151) 0.79 (0.187) 0.69 (0.213) 1.54 (0.285) 0.005* 0.040* 0.024* 0.055 0.039* LP * 0.009* A significant result (p < 0.05). interesting consistency, found in the results above, is that the subjects’ ΔHFC with normal chromatic discrimination is higher than that with good chromatic discrimination power under All mode …p < 0.001† , under the 3D mode (p ˆ 0.005), the 2D mode (p ˆ 0.04), the shutter system (p ˆ 0.024), the polarized system (p ˆ 0.055), LCD (p ˆ 0.039), and the laser projector (p ˆ 0.009). It is understood that individual differences affect the level of visual fatigue. Figure 2 shows the mean scores for each symptom corresponding to each mode; different intensities in the radial direction mean different mean scores. The mean score for each symptom in each mode is calculated by taking the score difference from each symptom; the score difference means the score’s difference between before and after viewing the display. Then we sum the scores from the four different trials 5 4 6 3 7 2 8 1 -0.2 -0.1 0.0 0.1 0.2 0.3 0.4 0.5 0.6 9 15 10 14 11 12 13 Fig. 2. Scores of symptoms in each mode. The outer point means that the discomfort level of the symptom is more serious. S3D S2D P3D P2D LP corresponding to the 15 symptoms, then minus 15 × 2.5 ˆ 37.5 (average), which was used to compare the effect on visual fatigue caused by different variables. Figure 3 shows the total ranking for each mode. The rankings for S3D and P3D are higher than for S2D, P2D, and LP. Then S2D, LP, and P2D are in descending order from high to low. But there are no differences between S3D and P3D. Figure 4 shows the total rank in the 3D and 2D modes, the LCD and LP, and the shutter and polarized. The total rank in the 3D mode is higher than in the 2D mode, but there are no differences between the LCD and LP, or the shutter and polarized. It shows that 3D videos cause more visual fatigue than 2D ones. The error bar in Figs. 3 and 4 comes from the SEs in the total rank from all participants. Fig. 3. Total rank for mean scores of each mode. 5. Conclusions and then divide by 4 (each mode repeats four times), so the mean score of each symptom can be obtained. After computing the mean score of all the symptoms, a radar plot is used to express the analysis results by questionnaire survey. The red line labels the highest scores for each symptom: (1) eyestrain, (2) dry eyes, which are much more serious and common, and (3) too bright, (5) feeling of pressure in the eyes, (7) blurred vision, (11) dazed feeling, (14) sleepy feeling, and (15) difficulty concentrating, which are also common symptoms. However, it is still hard to compare the effects of each variable. So the total ranking of mean scores for each symptom in the modes was used in the following analyses of the relationship between each mode and visual fatigue. According to Fig. 2, each mode in every symptom can be ranked by their mean scores. The ranking for mean scores of each symptom in each mode is ranked 5 (high) to 1 (low), which means that if a mode in the first symptom (eyestrain) has the largest mean score, it can get five points. Hence, after ranking all the symptoms in each mode, the total ranking points for each mode is derived by summing all the points Fig. 4. Total ranking for mean scores under 3D/2D mode (white), LCD/LP (gray), and shutter/polarized (black). According to the results of the analysis of the ΔHFC and questionnaire, the subjects suffer much more ciliary body strain and visual discomfort while viewing 3D videos than 2D videos (p < 0.001). One possible reason could be that the brain has to make more effort to adjust to the 3D variations, so it may affect the neural processing and lead to visual fatigue. Another reason could be that maybe the stereo of the 3D video is not as real when compared with natural vision. The binocular parallax that gives the depth perception lets people feel that the stereo effect is excessive, so the accommodation system is overloaded and tension occurs in the ciliary body. The subjects suffer much more ciliary body tension and visual discomfort while viewing 3D videos with shutter glasses than with polarized glasses (p ˆ 0.012). Because of the shutter system theory, brightness is relatively lower and the frames might glitter so that the subjects’ ciliary body is relatively tenser. In the marketplace, the polarized system camp claims that their system has no disadvantages over the shutter but the stereo is quite the same, and market research from DisplaySearch shows that the polarized system’s share of the market is increasing. Nevertheless, further research is needed to confirm the above claims and conjectures. Third, the ciliary body of subjects suffers more fatigue and visual discomfort while viewing 2D videos on a LCD TV than on the laser projector (LP) (p ˆ 0.008). Taking time sharing for example, color breakup may occur and affect people’s vision. One conclusion is that the cone and rod cells that discriminate between color and gray levels, and sense the resolution, are discrete in the spatial domain. This is similar to the spatial-formation method, so this method makes the ciliary body less tense. Another conjecture is that the ciliary body may have been stimulated more slowly by the spatial-formation method than the other method, during the 15 min experiment. So, those questions are worthy of discussion. Finally, subjects with normal chromatic discrimination power strain their ciliary body more than those with good chromatic discrimination power under each condition (All, p < 0.001; 3D, p ˆ 0.005; 2D, p ˆ 0.04; shutter, 0.024; polarized, p ˆ 0.055; LCD, p ˆ 0.039; LP, p ˆ 0.009). This indicates that individual differences do affect the levels of visual fatigue. The reason might be that some parts or mechanisms of the visual system in people with worse chromatic discrimination are weaker, hence the different states of the ciliary body. Generally, visual comfort is more serious for subjects with normal chromatic discrimination than those with the good, and while watching 3D videos and especially wearing shutter glasses, or watching 2D videos and especially by LP. However, there are no differences between viewing 2D content on LCD TVs and 3D content with polarized glasses. In order to compare the subjective and objective results, the design of the questionnaire is a key point to enhance effectiveness. The rankings for S3D and P3D are higher than for S2D, P2D, and LP. Then S2D, LP, and P2D are in descending order from high to low. But there are no differences between S3D and P3D. The total rank in the 3D mode is higher than in the 2D mode, but there are no differences between the LCD and DLP, or the shutter and polarized. However, these results again show that the level of visual fatigue is more serious after viewing 3D videos. It is obvious that some mismatches occurred in the ΔHFC result analysis and questionnaire under certain conditions. Though different ciliary body conditions were detected, the visual discomfort, as evaluated by the questionnaire, is the same. One explanation is that the questionnaire is a subjective method dependent on subjective cognition for evaluations; hence, the reliability and validity of this method need to be considered. Perhaps those mismatches are due to this indicator’s inherent inaccuracies, so it is not effective in diagnosing and comparing the factors that cause visual fatigue or their significance. In conclusion, this paper discovers the following fact: 3D videos cause people more visual fatigue than do 2D videos (p < 0.001). The shutter glasses afflict people with more visual fatigue than do polarized glasses (p ˆ 0.012). The time-sharing method causes people more visual fatigue than does the spatialformation method (p ˆ 0.008). There is no difference between LED backlighting and mixed LED and LD light sources (p ˆ 0.162). People with normal color discrimination power suffer more visual fatigue than those with generally good color discrimination power (p < 0.001), but the levels of visual discomfort are the same while viewing 2D on LCD TVs, and 3D contents with polarized glasses. The HFC can indeed evaluate physiological stress or strain resulting objectively from exertion of the visual system, leading to visual fatigue. 6. Discussion In this work, using chromatic discrimination as a grouping index is very successful. From the results it can be found that people with normal color discrimination have more visual fatigue than those with good. In general, if someone’s chromatic discrimination is very good, he is supposed to distinguish the red, green, and blue subpixels easily when viewing a display, which means he will feel the image is blurred because RGB are separated. Viewing a blur image or video for a long time causes people to feel discomfort, especially in the eyes. On the contrary, the results are different, as we expected. People with normal color discrimination have more visual fatigue than those with good (p < 0.001). This part requires more verification to support the results. Another issue that should be addressed is the relation between luminance and accommodative microflutuation. As mentioned in Table 2, it can be found that different modes have each luminance; the luminance can affect the pupil size. Also, the pupil size is associated with accommodation, which means the pupil size can affect the accommodation microflutuations. However, the HFC fluctuations are imperceptible when the pupil changes with light: this only causes LFC fluctuation increases; it does not affect our results [21]. Hence, accommodative microflutuation can effectively and objectively determine whether subjects are suffering from visual fatigue when compared with other indicators. This paper was partially supported by the Aim for the Top University Program of the National Chiao Tung University, the Ministry of Education of Taiwan, the Ministry of Science and Technology of Taiwan (NSC 102-2220-E-009-016), and the Industrial Technology Research Institute. The authors also thank them for providing experimental assistance and related information. References 1. M. Lambooij, W. Ijsselsteijn, M. Fortuin, and I. Heynderickx, “Visual discomfort and visual fatigue of stereoscopic displays: a review,” J. Imaging Sci. Technol. 53, 030201 (2009). 2. E. H. Stupp and M. S. Brennesholtz, Projection Displays (Wiley, 1999). 3. T. Jarvenpaa, “Measuring color breakup of stationary images in field-sequential-color displays,” J. Soc. Inf. Display 13, 139–144 (2005). 4. D. L. Post, P. Monnier, and C. S. Calhoun, “Predicting color breakup on field-sequential displays,” Proc. SPIE 3058, 57–65 (1997). 5. X. Zhang and J. E. Farrell, “Sequential color breakup measured with induced saccades,” Proc. SPIE 5007, 210–217 (2003). 6. E. Umezawa, T. Shibata, T. Kawai, and K. Ukai, “Ergonomic evaluation of a projector using field sequential color projection system,” in Proceedings of the 11th International Display Workshops (Society for Information Display, 2004), pp. 1531–1534. 7. D. L. Post, A. L. Nagy, P. Monnier, and C. S. Calhoun, “Predicting color breakup on field-sequential displays: Part 2,” SID Symp. Dig. Tech. Pap. 29, 1037–1040 (1998). 8. S. H. Kim, T. Shibata, T. Kawai, and K. Ukai, “Physiological effects of color breakup in field-sequential color projection system,” SID Symp. Dig. Tech. Pap. 37, 314–317 (2006). 9. M. Ogata, K. Ukai, and T. Kawai, “Visual fatigue in congenital nystagmus caused by viewing images of color sequential projectors,” J. Display Technol. 1, 314–320 (2005). 10. C. F. Chi and F. T. Lin, “A comparison of seven visual fatigue assessment techniques in three data-acquisition VDT tasks,” Human Factors 40, 577–590 (1998). 11. L. S. Gray, B. Gilmartin, and B. Winn, “Accommodation microfluctuations and pupil size during sustained viewing of visual display terminals,” Ophthalmic Physiol. Opt. 20, 5–10 (2000). 12. M. Kajita, M. Ono, S. Suzuki, and K. Kato, “Accommodative microfluctuation in asthenopia caused by accommodative spasm,” Fukushima J. Med. Sci. 47, 13–20 (2001). 13. J. R. Wilson and E. N. Corlett, Evaluation of Human Work: A Practical Ergonomics Methodology (Taylor & Francis, 1995), Chap. 28. 14. N. Pouratian, S. A. Sheth, N. A. Martin, and A. W. Toga, “Shedding light on brain mapping: advances in human optical imaging,” Trends Neurosci. 26, 277–282 (2003). 15. M. J. Nichols and W. T. Newsome, “The neurobiology of cognition,” Nature 402, C35–C38 (1999). 16. B. A. Wandell and R. F. Dougherty, “Computational neuroimaging: maps and tracts in the human brain,” Proc. SPIE 6057, 605701 (2006). 17. A. M. Dale and E. Halgren, “Spatiotemporal mapping of brain activity by integration of multiple imaging modalities,” Curr. Opin. Neurobiol. 11, 202–208 (2001). 18. J. D. Bullough, Y. Akashi, C. R. Fay, and M. G. Figueiro, “Impact of surrounding illumination on visual fatigue and eyestrain while viewing television,” J. Appl. Sci. 6, 1664– 1670 (2006). 19. W. N. Charman and G. Heron, “Fluctuations in accommodation: a review,” Ophthalmic Physiol. Opt. 8, 153–164 (1988). 20. T. Iwasaki and A. Tawara, “Reduction of asthenopia related to accommodative relaxation by means of far point stimuli,” Acta Ophthalmol. Scand. 83, 81–88 (2005). 21. S. Suzuki, M. Kajita, and K. Kato, “Evaluation of accommodative function by high frequency component of accommodative microfluctuation,” Jpn. J. Vis. Sci. 22, 93–97 (2001). 22. B. Winn and B. Gilmartin, “Current perspective on microfluctuations of accommodation,” Ophthalmic Physiol. Opt. 12, 252–256 (1992). 23. E. C. Huang and V. H. Barocas, “Accommodative microfluctuations and iris contour,” J. Vis. 6(5), 653–660 (2006). 24. M. Day, N. C. Strang, D. Seidel, L. S. Gray, and E. A. H. Mallen, “Refractive group differences in accommodation microfluctuations with changing accommodation stimulus,” Ophthalmic Physiol. Opt. 26, 88–96 (2006). 25. F. W. Campbell, J. G. Robson, and G. Westheimer, “Fluctuations of accommodation under steady viewing conditions,” J. Physiol. 145, 579–594 (1959). 26. E. Harb, F. Thorn, and D. Troilo, “Characteristics of accommodative behavior during sustained reading in emmetropes and myopes,” Vis. Res. 46, 2581–2592 (2006). 27. P. Denieul, “Effects of stimulus vergence on mean accommodation response, microfluctuations of accommodation and optical quality of the human eye,” Vis. Res. 22, 561–569 (1982). 28. C. Miege and P. Denieul, “Mean response and oscillations of accommodation for various stimulus vergences in relation to accommodation feedback control,” Ophthalmic Physiol. Opt. 8, 165–171 (1988). 29. J. C. Kotulak and C. M. Schor, “Temporal variations in accommodation during steady-state conditions,” J. Opt. Soc. Am. A 3, 223–227 (1986). 30. W. N. Charman and H. Radhakrishnan, “Accommodation, pupil diameter and myopia,” Ophthalmic Physiol. Opt. 29, 72–79 (2009). 31. F. W. Campbell and G. Westheimer, “Dynamics of the accommodation responses of the human eye,” J. Physiol. 151, 285– 295 (1960). 32. L. R. Stark and D. A. Atchison, “Pupil size, mean accommodation response and the fluctuations of accommodation,” Ophthalmic Physiol. Opt. 17, 316–323 (1997). 33. L. J. Bour, “The influence of the spatial distribution of a target on the dynamic response and fluctuations of the accommodation of the human eye,” Vis. Res. 21, 1287–1296 (1981). 34. S. Phillips and L. Stark, “Blur: a sufficient accommodative stimulus,” Doc. Ophthalmol. 43, 65–89 (1977). 35. C. M. Schor, C. A. Johnson, and R. B. Post, “Adaptation of tonic accommodation,” Ophthalmic Physiol. Opt. 4, 133–137 (1984). 36. L. R. Stark, N. C. Strang, and D. A. Atchison, “Dynamic accommodation response in the presence of astigmatism,” J. Opt. Soc. Am. A 20, 2228–2236 (2003). 37. M. Alpern, “Variability of accommodation during steady fixation at various levels of illuminance,” J. Opt. Soc. Am. 48, 193–197 (1958). 38. A. Mira-Agudelo, L. Lundstrom, and P. Artal, “Temporal dynamics of ocular aberrations: monocular vs binocular vision,” Ophthalmic Physiol. Opt. 29, 256–263 (2009). 39. T. Iwasaki and S. Kurimoto, “Objective evaluation of eye strain using measurements of accommodative oscillation,” Ergonomics 30, 581–587 (1987). 40. D. R. Iskander, M. J. Collins, M. R. Morelande, and Z. Mingxia, “Analyzing the dynamic wavefront aberrations in the human eye,” IEEE Trans. Biomed. Eng. 51, 1969–1980 (2004). 41. B. Winn, J. R. Pugh, B. Gilmartin, and H. Owens, “Arterial pulse modulates steady-state ocular accommodation,” Curr. Eye Res. 9, 971–975 (1990). 42. T. Geacintov and W. S. Peavler, “Pupillography in industrial fatigue assessment,” J. Appl. Psych. 59, 213–216 (1974). 43. H. S. Rigby, B. F. Warren, J. Diamond, C. Carter, and J. W. B. Bradfield, “Colour perception in pathologists: the Farnsworth–Munsell 100-hue test,” J. Clin. Pathol. 44, 745–748 (1991). 44. M. Collins, B. Davis, and J. Wood, “Microfluctuations of steady-state accommodation and the cardiopulmonary system,” Vis. Res. 35, 2491–2502 (1995). 45. M. Emoto, T. Niida, and F. Okano, “Repeated vergence adaptation causes the decline of visual functions in watching stereoscopic television,” J. Display Technol. 1, 328–340 (2005).