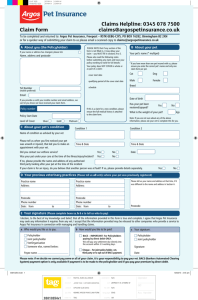
Click here for the printable form.
advertisement

MY VET ANIMAL HOSPITAL WELCOME TO MY VET ANIMAL HOSPITAL! Thank you for your interest in our practice. Please complete this information form to facilitate the check-in process at your first visit. You can complete the automated form online and submit or bring a printed copy in for your first appointment. Please be sure to contact our Client Care Coordinator today to schedule your appointment! CLIENT INFORMATION (Primary Caregiver) Last Name:_______________________________First Name:_________________________ Address:___________________________________________Apt/Unit Number:__________ City:_____________________ State:________ ZIP Code:____________ Primary Phone:________________________ Secondary Phone:_______________________ Email:____________________________________ *Please note the primary contact will receive calls with results and reminder emails* **Your email address will be kept private and will only be used in correspondence regarding your pet's medical needs including yearly vaccination reminders, Exam Report Cards, and invoices** ADDITIONAL CLIENT INFORMATION: Partner/Spouse Last Name:______________________ First Name:______________________ Address:________________________________________ Apt/Unit Number:_______________ City:_____________________ State:________ ZIP Code:____________ Primary Phone:_______________________ Secondary Phone:_________________________ Email:____________________________________ PATIENT(S) INFORMATION: Pet's 1 Pet's 2 Name Gender (including spayed or neutered) Species (Canine or Feline) AAHA Accredited: We’re Setting the Standard of Veterinary Excellence "Best Vet," in Chicago Reader's Best of Chicago 2010 info@myvetanimalhospital.com | www.myvetanimalhospital.com Pet's 3 MY VET ANIMAL HOSPITAL Breed Color Date of Birth Previous Veterinarian Existing Medical Conditions Current Medications/Dosage Current Diet TREATMENT I, the undersigned owner or agent of the owner, am responsible for seeking veterinary care for the pet(s) identified above and certify that I am eighteen years or over. I agree that after consultation with me, the hospital's doctors may prescribe medication to treat, hospitalize, sedate, anesthetize, or perform surgery on my pet. Initial______ PAYMENT I understand that an estimate of the fees for veterinary services will be provided to me at my request and that I am encouraged to discuss all fees related to it before services are rendered and during my pet's ongoing medical treatment. I agree to assume financial responsibility for all fees and will provide payment via cash, credit card, or Care Credit at the time of service. Initial______ SOCIAL MEDIA I, hereby grant My Vet Animal Hospital permission to use, reuse, publish, broadcast, in any and all media my name and the photographs or video footage taken of me and/or my pet in which I may be included with others. I release My Vet Animal Hospital from any demands arising out of the use of photographs, video, and audio material including without limitation, all claims for libel or invasion of privacy. Initial______ Client Signature:____________________________________________ Date:_____________ AAHA Accredited: We’re Setting the Standard of Veterinary Excellence "Best Vet," in Chicago Reader's Best of Chicago 2010 info@myvetanimalhospital.com | www.myvetanimalhospital.com