Jangsook Kim DDS
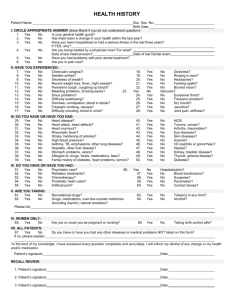
MEDICAL HISTORY
1.
2.
3.
4.
5.
6.
Have you been under care of a medical doctor during the past two years?
If yes, for what? ________________________ Physician’s Name ____________________________________
Are you taking any medication, drugs or pills, including regular dosages of aspirin?
If yes, please list all within the last 2 years, name and dosage _________________________________________
____________________________________________________________________________________________
Are you aware of having an allergic reaction to any medication or substance?
If yes, please list ______________________________________________________________________________
Have you been a patient in the hospital during the past five years?
If yes, please describe _________________________________________________________________________
Are you pregnant? Yes No Months? ____
Are you breastfeeding? Yes No
Taking birth control pills?
Have you ever had any unfavorable reaction to a dental treatment?
If yes, please explain _________________________________________________________________________
Yes
No
Yes
No
Yes
No
Yes
No
Yes
Yes
No
No
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
Yes
No
Indicate which of the following you have had, or have at present. Circle “yes“ or “no“ to each item
AIDS / HIV
Alcoholism
Allergies or hives
Anemia
Arthritis, rheumatism
Artificial joints
Asthma
Bleeding problems
Blood disease
Bruise easily
Cancer
Chemotherapy
Chest pain
Chronic cough
Cold sores, fever blisters
Congenital heart disease
Contact lenses
Cortisone Medicine
Diabetes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
Yes
No
Emphysema
Epilepsy or seizures
Fainting or dizzy spells
Glaucoma
Hay fever
Headache
Heart attack, surgery
Heart murmur
Hemophilia
Hepatitis A or B
High blood pressure
Kidney disease
Latex allergies
Liver Disease
Low blood pressure
Nervous disorders
Neurological disorders
Osteoporosis
Pacemaker
Penicillin allergies
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
No
Phen-fen use
Psychiatric care
Psychological care
Radiation therapy
Rheumatic fever
Sickle cell disease
Sinus trouble
Smoking
Stomach ulcer
Stroke
Swollen ankles
Thyroid problems
TMJ problems
Tuberculosis
Tumors
Ulcers
Venereal Disease
Yellow Jaundice
Do you have or have you had any disease, condition or problem not listed?
If yes, please list _________________________________________________________________________________
I understand the above information is necessary to provide me with dental care in a safe and efficient manner. I have answered
all questions to the best of my knowledge. Should further information be needed, you have my permission to ask the respective
health care provider or agency, who may release such information to you. I will notify the doctor of any changes in my health
or medication.
______________________________
Patient Name
__________________________
Signature
____________
Last updated
________________________
Dentist Signature
Please STOP !! These are for the future to update your medical history yearly.
2ND YEAR MEDICAL HISTORY UPDATE Has there been any change in your health since your last dental appointment?
If yes, please explain…………………………………………………………………………………………………………………
______________________________
Patient Name
__________________________
Signature
____________
Last updated
937 N. Lemon St Anaheim, CA 92805
__________________________
Signature
____________
Last updated
No
________________________
Dentist Signature
3RD YEAR MEDICAL HISTORY UPDATE Has there been any change in your health since your last dental appointment?
If yes, please explain …………………………………………………………………………………………………………………
______________________________
Patient Name
Yes
Yes
No
________________________
Dentist Signature
23501 Cinema Dr. Suite 114 Valencia, CA 91355
 0
0