Blood-Borne Viruses Guidance
advertisement

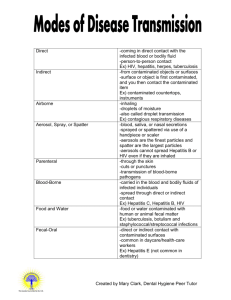
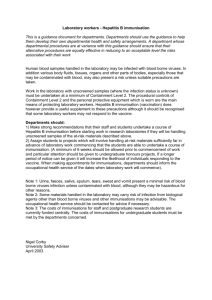
Blood-Borne Viruses Guidance Blood-borne viruses (BBVs) may cause severe disease in some people and few or no symptoms in others. The virus can spread to another person, whether or not the infected person has symptoms. The main blood-borne viruses of concern are: Hepatitis B and Hepatitis C which cause Hepatitis, a disease of the liver Human Immunodeficiency Virus (HIV), which causes acquired Immune Deficiency Syndrome (AIDS) These viruses are carried in the blood of infected people (who may not know they are infected). They can also be found in other body fluids, for example, semen, vaginal secretions and breast milk. Body fluids such as urine, faeces, saliva and vomit may contain the virus but are unlikely to carry an infection risk unless they are contaminated with blood. However, care should still be taken, as the blood may not be visible. It is important to remember that the precautions referred to in this document need to be applied in proportion to the risk experienced by staff. As with all health and safety requirements, staff / employees includes those such as agency and voluntary workers. Acquired Immune Deficiency Syndrome (AIDS) is a term that is used to describe the late stage of HIV. This is when the immune system has stopped working and the person develops a life-threatening condition, such as pneumonia (infection of the lungs). The term AIDS was first used by doctors when the exact nature of HIV was not fully understood. However, the term is no longer widely used because it is too general to describe the many different conditions that can affect somebody with HIV. Specialists now prefer to use the terms of advanced or late-stage HIV infection. HIV is not passed on easily from one person to another, especially compared to other viruses. That’s because HIV is present in body fluids. So for HIV to be passed on, the body fluids of someone who is already infected have to get into an uninfected person’s body and then into their bloodstream. The body fluids that contain enough HIV to infect someone are: Seminal fluid Vaginal fluids, including menstrual fluids Breast milk Blood The mucous found in the rectum Pre-cum (the fluid that the penis produces for lubrication before ejaculation) Other body fluids, like saliva, sweat or urine, do not contain enough of the virus to infect another person. 1 So the main ways that HIV can be transmitted are: Through sexual intercourse and other sexual activities From mother to baby From blood to blood The most common way to become infected with HIV is through sexual contact. HIV is not passed on through normal social contact, including: Through unbroken, healthy skin Kissing Sharing cups, plates, cutlery or linen, such as towels Using the same toilets and swimming pools. Caring for someone living with HIV or AIDS does not put you at risk, and neither does mouth-to-mouth resuscitation. You cannot breathe it in or get infected by mosquitoes or other animals. There is, therefore, a virtually insignificant risk of contract HIV at work, even in what may be through of as higher risk areas. Scope Most staff and service users will only be exposed to common airborne infections such as colds and influenza. However, some staff may be at risk of exposure to BBVs, such as: Health care workers and those delivering personal care Staff of special schools / residential accommodation for those with challenging behaviours e.g. human biting resulting in breaking the skin and drawing blood. Staff exposed to violence resulting in skin breakage Staff at risk from sharps injury (skin puncture), by coming into contact with things such as used hypodermic needles, broken contaminated glass or contaminated machinery / motor vehicles. Staff regularly exposed to bodily fluids as part of their normal duties, including handling of clinical waste, contaminated laundry, waste/refuse of unknown origin, sewage e.g. refuse workers, house clearance workers. First Aiders / Appointed Persons. Staff who work with people who have severe learning disabilities or known drug offenders. 2 NB: Of course some first aiders and carers will feel vulnerable to the potential risk of exposure to BBVs. However if universal precautions are taken, which should always be the case, the risk is significantly reduced to an acceptable level. Examples of universal precautions include: Good hand washing and care of the hands. Ensuring cuts and breaks in the skin on the first aiders hands and arms are covered with a waterproof dressing. Using protective clothing i.e., disposable gloves. Minor wounds should be cleaned and dried using clean water and disposable paper towels or tissues. A first aid plaster or dressing (individually wrapped) can be applied if desired. Larger wounds should be washed with water; a suitable dressing or pressure pad can be applied if needed. Disposable gloves should be worn where possible, but in an emergency first aid care should not be withheld because gloves are not available. This list corresponds with the groups included in Health and Safety Executive guidance and the Immunisation Against Infectious Disease 2006 document from the Department of Health. However, this list is not intended to be comprehensive. In order to determine staff at risk of exposure to Hepatitis B specifically, a risk assessment should be completed. KCC is committed to the health, safety and welfare of its employees and recognises the duty of care owed to others not in its employment. In turn it also recognises the duty of care owed by others to our employees and volunteers while working on our premises. The why, what and how Urine, faeces, saliva, sputum, tears and vomit carry a minimal risk of BBV infection, unless they are contaminated with blood. Care should always be taken however, as the presence of blood is not always obvious. BBVs can also remain infectious in dried blood and liquid for several weeks. BBVs cannot be spread in swimming pools, sharing toilets, crockery, or by daily workplace activities, such as shaking hands or working with others. Accidents with blood-contaminated needles in healthcare workers are probably the most common method of occupational transmission of BBV. Contraction of BBV can be prevented by safe working practices. For most people, simple measures such as being careful when cleaning up spilt blood and keeping wounds covered are all that are required. However, any incident in which blood from one person may have penetrated the skin of another person (e.g. by biting or from a 3 contaminated needle), or as a result of contamination of the mucous membranes (eyes, nose and mouth), should be reported to the officer in charge or the headteacher. Hepatitis B, Hepatitis C and HIV can be spread through: Unprotected sexual contact with an infected person. The injection of infected blood into an uninfected person’s bloodstream (e.g. drug users sharing needles, needlestick injuries, contaminated needles used for tattooing and ear piercing). Contamination of open wounds and biting. A mother to her unborn child. An accident form HS157 must be completed to record the incident and first aid action taken as described in part 5 of this document. Hepatitis There are several types of Hepatitis, but Hepatitis B and C are blood-borne viruses. Not all those with acute Hepatitis will have symptoms. Depending on the type, a certain number will go on to develop chronic infection but even then some may experience only mild symptoms or no symptoms at all. After the virus enters the body, the incubation period is one to six months. Many people have their virus in their bodies for a long time (sometimes for life) and never have any symptoms. These people are carriers and may be unaware that they carry the virus. Most carriers are infectious, whereas some get rid of the virus after several years. About 25% of carriers develop serious liver disease. Hepatitis B, sometimes called Hep B or HBV, is a liver disease. The virus circulates in the blood stream and causes inflammation of the liver, possibly leading to jaundice in rare cases. A sudden inflammation of the liver is known as acute Hepatitis. Where inflammation of the liver lasts longer than six months the condition is known as chronic Hepatitis. Cirrhosis of the liver can also occur if the liver is damaged longterm, which in turn can develop into liver cancer in some people. There is a vaccine that can protect people from Hepatitis B. It is suitable for protecting the small number of people at greatest risk of contracting the disease. Hepatitis C, sometimes called Hep C or HCV, is also a liver disease. The effects vary from one individual to another. While many people will remain symptom free, some will develop cirrhosis and a few will develop liver cancer. Hepatitis C is spread in the same way as Hepatitis B. Unlike Hepatitis B, there is no available vaccine for Hepatitis C, so universal infection control measures should be followed at all times. Hepatitis C can now be treated and around 55% of those individuals are cured. 4 Acquired Immune Deficiency Syndrome (AIDS) A great deal of information has been issued by central government on the subject of AIDS. The disease is principally transmitted either sexually or by the injection of contaminated blood. In the normal working environment, the risk of AIDS being transmitted is very small. Even for staff caring for children or adults who carry the antibodies of these diseases, who could therefore be infectious, the risks are extremely small provided simple routine hygiene precautions are taken. AIDS is caused by the virus HIV which attacks the body’s immune system. This can leave the body open to a wide variety of infections and can lead to death. However, many people who carry the virus (and are therefore HIV Positive) remain entirely healthy. Information and Training Heads of establishments and other managers are responsible for seeing that full information about the nature of these diseases and the measures necessary to control them are made available to all staff, and that staff receive appropriate training via a competent person. Heads of establishments and other managers are responsible for seeing that good hygiene practices are regularly followed in all KCC premises, and that staff are allowed adequate time for carrying out the recommended procedures. Employees need to know: If they could be exposed to blood-borne viruses and how; The risks posed by this exposure; The main findings of the risk assessment; The precautions they should take to protect themselves and other employees, contract staff, volunteers or visitors; and What procedures to follow in the event of an emergency. Risk assessment for Blood-Borne Viruses Managers should firstly consider if their team are exposed to blood-borne viruses through their work activities, remembering to consider volunteer activities. A list of occupational staff groups at possible risk of contraction has been produced for that purpose (Appendix 2). The list is designed to identify KCC staff members who are at greater risk than others within the organisation. If your team is not covered by this list and you believe them to be at risk, please contact either Staff Care Services (Occupational Health) or the Health and Safety Advice Line for further information and guidance. No KCC employee would be classed as being at ‘high risk’ on a national scale, as those most at risk are emergency staff, hospital staff, dentists and similar occupations. 5 For teams identified on the list, a risk assessment should be completed. A generic risk assessment form has been created to identify further procedures (Appendix 3). When completing the risk assessment, the following factors should be considered: Where the infection is likely to be present e.g., needles, waste? Ways in which employees/volunteers may be exposed e.g., first aid, handling contaminated items? What information is given to employees/volunteers about BBVs? Estimate the level of exposure considering: How often staff / volunteers are likely to come into contact with blood? How many different peoples’ blood are they likely to come into contact with? How good are existing measures e.g., universal hygiene precautions? Guidance on completing a risk assessment is available from SafetyNet or contact the Health and Safety Advice Line. It is recommended that staff members who are identified as being in the moderate / high risk categories on the risk assessment be vaccinated against Hepatitis B. First Aid Treatment For all BBV contamination accidents / injuries, including: Where a needle or other sharp object punctures the skin. Where BBV contamination of an open wound, eyes, mouth or other mucous membrane has occurred. Where a human bite or scratch puncturing the skin has occurred. The injured person MUST: Wash splashes off the skin with soap and running water. If the skin is broken, gently encourage the wound to bleed. Do NOT suck the wound – rinse thoroughly under running water. Wash out splashes in the eyes with plenty of tap water – do not swallow the water. Cover the wound with a waterproof dressing. Seek medical attention as soon as possible e.g. from an A&E department or their own doctor ideally within 1 hour and not more than 48 hours. Inform the manager / team leader / head teacher. Complete an accident/incident form (HS157). Inform the Occupational Health Unit and the Health and Safety Advice Line. 6 The Manager MUST: If possible, obtain a blood sample with full consent from the source, where known, of the needlestick. If the service user is known to be Hepatitis B or HIV positive or the injured person (recipient) is a known non-responder to Hepatitis B vaccine (not immune), the recipient must attend the local A&E department or GUM clinic for post exposure prophylaxis treatment – ideally within 1 hour and not more than 48 hours. Special consideration for first aiders If you are a first aider in the workplace, the risk of being infected with a BBV while carrying out your duties is small. There has been no recorded case of HIV or Hepatitis B being passed on during mouth-to-mouth resuscitation. The following precautions can be taken to reduce the risk of infection: Cover any cuts or grazes on your skin with a waterproof dressing; Wear suitable disposable gloves when dealing with blood or any other body fluids; Use suitable eye protection and a disposable plastic apron where splashing is possible; Use devices such as face shields when you give mouth-to-mouth resuscitation, but only if you have been trained to use them; Wash your hands after each procedures. As a first aider it is important to remember that you should not withhold treatment for fear of being infected with a BBV. Associated procedures and documentation The documentation below refers to related guidance and legislation. Related Guidance HSE INDG342 – Blood-borne viruses in the Workplace (http://www.hse.gov.uk/pubns/indg342.pdf) SafetyNet guidance: Safe Disposal of Discarded Needles and Syringes Universal Precautions for the Control of Infection Guidance on MRSA First Aid Use of gloves (SC) Infection Control - Prevention of Healthcare-associated Infection in Primary and Community Care (NICE) Infection Control Guidance for Care Homes (Department of Health) 7 Guidance on Communicable Disease and Infection Control in Schools and Nurseries (Kent Health Protection Unit) Guidelines for Infection Prevention and Control in the Community (Kent Health Protection Unit) Legislation The Health and Safety at Work Act 1974 The Management of Health and Safety at Work Regulations 1999 The Personal Protective Equipment Regulations 1992 The Control of Substances Hazardous to Health Regulations 2002 Reporting of Injuries, Diseases and Dangerous Occurrences Regulations (RIDDOR) 2013 The Health & Safety (First-Aid) Regulations 1981 Frequently asked questions How can I prevent exposure to blood-borne viruses? Exposure to blood-borne viruses can be prevented by adhering to infection control procedures as outlined in the Universal Precautions for the Control of Infection guidance. Managers must remember that vaccination is not the ultimate protection and the emphasis must be on behaviour. A safe and effective vaccine for the prevention of Hepatitis B infection is available, that said, immunisation should not be relied upon as a primary control to prevent exposure. There are currently no vaccines available against Hepatitis C or HIV, although there are measures that can be taken following exposure, which may prevent the development of infection. Studies have indicated, however, that antiviral therapy does not prevent acquisition of infection following Hepatitis C exposure, although there is evidence that therapy given shortly after acquisition is more successful, in terms of a sustained viral response, than therapy given later. Such treatment should be seen as distinct from post-exposure ‘prophylaxis’. The procedures for management of incidents involving exposure to a blood-borne virus can be found at Appendix 5. What is the procedure for vaccination against Hepatitis B? Hepatitis B immunisation is recommended for all employees whose work tasks involve exposure to blood, blood-stained body fluids or tissues and there is a risk of injury e.g. puncturing / breaking of the skin, splashing into the eyes or mouth. Immunisation can also be recommended based on a risk assessment. Where universal hygiene precautions are deemed to be insufficient to bring the risk of BBV contamination down to an acceptable level, Hepatitis B immunisation is 8 advised. This provides effective protection but should not be regarded as a substitute to safe working practices. Should vaccination be recommended by the risk assessment, the line manager should approach a healthcare provider (see Appendix 1). The vaccinations are given at 0, 1 and 6 months with a blood test at 8 months, following the first injection. It is very important to attend for this blood test as this is the only means of determining your level of immunity (protection) and whether or not the vaccine has worked. A booster injection is given 5 years after the initial injection if your level of immunity is adequate (the timing and need for a Hepatitis B booster injection is subject to change and advice must always be sought via your care provider). The cost of the vaccination can be claimed back from KCC and it is the responsibility of managers to make provision for the cost of immunisation in their budgets. It may also be possible to negotiate a slightly reduced price for each individual as part of a ‘bulk purchase’. Following guidance issued by the General Practitioners Committee (GPC) to its members not to vaccinate their patients for occupational purposes as it is the employer’s responsibility; most GPs will not issue vaccinations. However, many GPs still do so. It should also be noted that some people do not respond to the vaccine. First aid measures described above must be followed and the injured person must seek further advice and prophylaxis treatment via the local A&E department. The Hepatitis B Immunisation Programme and schedule can be found at Appendix 4. What is the procedure for post-exposure injections against Hepatitis B? Any staff that have been exposed to any blood-borne virus should be given a postexposure prophylaxis (PEP) treatment / advice within 48 hours, and preferably within one hour of exposure. Staff who may have been exposed to a blood-borne virus must contact their local hospital immediately and report the type of injury and donor status of infection (if known). What is the procedure for Hepatitis B booster injections? Current medical advice on the necessity of booster injections varies, with some studies showing that they are not necessary to ensure long-term protection against Hepatitis B. A booster injection is usually given 5 years after the initial vaccination. The need for a booster injection depends on your level of immunity following Hepatitis B vaccination. Your level of immunity is measured by a blood test after you have completed the course of vaccination, and is usually at 8 months following your first injection. 9 Individuals should seek current guidance from their care provider and with reference to Department of Health, Hepatitis B, Chapter 18, “The Green Book”. How do you test for blood-borne virus? BBVs are detected by a blood test. The test looks for antibodies to the virus which are produced by the body’s immune system in response to the virus. The most common test for HIV is a blood test, although newer tests can detect HIV antibodies in mouth fluid. If staff are concerned they may have contracted a bloodborne virus as a result of occupational exposure they must consult either occupational health or their local A&E (in the interim). Another place staff can access testing is their local Genito Urinary Medicine (GUM) clinic. What general precautionary measures should I take for personal hygiene? To avoid contraction of BBVs, personal hygiene measures should be followed at all times. More in-depth guidance on this area is available in the SafetyNet document Universal Precautions for the Control of Infection. Where can we get further guidance on blood-borne viruses? Other external documents on specific areas of risk can also be found in ‘Associated procedures and documentation’ section of this document, and online. The British Liver Trust website (www.britishlivertrust.org.uk) contains lots of useful information on diseases related to liver disease. What general precautionary measures should I take for personal hygiene? To avoid contraction of BBVs, personal hygiene measures should be followed at all times. More in-depth guidance on this area is available in the SafetyNet document Universal Precautions for the Control of Infection. Where can we get further guidance on blood-borne viruses? Other external documents on specific areas of risk can also be found in ‘Associated procedures and documentation’ section of this document, and online. The British Liver Trust website (www.britishlivertrust.org.uk) contains lots of useful information on diseases related to liver disease. 10 Where can I obtain further advise? NHS Choices - http://www.nhs.uk/nhs-direct/Pages/NHS-Direct-legacyenquiries.aspx Public Health England 03442 257968 KCC Staff Care Services (Occupational Health) – 03000 411411 Health and Safety Advice Line 03000 418456 11 Appendix 1 Health care providers Provider Tel No. Address Dartford & Gravesham NHS Trust 01322 428100 Darent Valley Hospital Darenth Wood Road Dartford Kent DA2 8DA Queen Mary’s Hospital Sidcup 0208 302 2678 East Kent Hospitals NHS Trust 01227 766877 Maidstone & Tunbridge Wells NHS Trust 0845 155 1000 Medway NHS Trust 01634 830000 Queen Mary’s Hospital Frognal Lane Sidcup Kent DA14 6LT East Kent Hospital Trust Headquarters Kent and Canterbury Hospital Ethelbert Road Canterbury Kent CT1 3NG Trust Headquarters Jenex House Church Street Maidstone Kent ME14 1DS Medway Maritime Hospital Windmill Road Gillingham Kent ME7 5NY Last Reviewed: April 2014 NB: Immunisation programmes must be provided by appropriately qualified providers e.g. Occupational Health services or GPs. For further information on national standards for immunisation, please click on the following link. Note: Staff Care Services, KCC Occupational Health are now able to provide the vaccination programme for Hepatitis B. There will be a charge for this service. 12 Appendix 2 Occupational staff groups at possible risk of contracting a Blood-borne virus (BVV) NB: Staff groups include volunteers Directorate Occupational group SC Older People/Learning Disability/Assessment & Enablement Services BBV hazard a) Contact with body fluids e.g. urine, faeces Carers Agency staff Drivers/escorts Care Centre Staff Community Support Workers including Occupational therapist Technicians Personal Assistants Therapy Staff b) Handling sharps e.g. needles c) Human biting & scratching resulting in breaking of the skin d) Handling contaminated laundry e) Disposal of Clinical Waste f) Contamination of open wounds whilst handling: Blood-stained body fluids Cleaning of vehicles Children’s Social Services a) Human biting & scratching resulting in breaking of the skin Children’s services provider unit staff Pupil referral unit staff Caretakers b) Contamination of open wounds whilst handling: Blood-stained body fluids Disposal of clinical waste Handling sharps e.g. needles Disposal of contaminated waste Attend local A&E clinic as soon as possible (ideally within 1 hour and no later than 48 hours): 13 Seek specialist advice / treatment from microbiologist / virologist Ensure blood sample collected for storage Directorate Occupational group BBV hazard GT a) Handling sharps e.g. needles Fixed site needle exchanges Community teams Kent Scientific Services a) Contamination of open wounds whilst handling: Laboratory staff Blood-stained body fluids Disposal of clinical waste Handling sharps e.g. needles Disposal of contaminated waste Community Safety a) Contact with sharps b) Human biting & scratching resulting in breaking of the skin Community wardens c) Contamination of the eyes or mouth of body fluid e.g. sputum, vomit d) Contamination of open wounds whilst handling: Blood-stained body fluids Waste Management a) Contact with sharps Waste site staff b) Human biting & scratching resulting in breaking of the skin c) Contamination of the eyes or mouth of body fluid e.g. sputum, vomit d) Contamination of open wounds whilst handling: Blood-stained body fluids Country Parks a) Contact with sharps b) Human biting & scratching resulting in Country park rangers 14 breaking of the skin c) Contamination of the eyes or mouth of body fluid e.g. sputum, vomit d) Contamination of open wounds whilst handling: All Blood-stained body fluids a) Puncturing of the skin whilst handling: First Aiders (Please see Page 3 re: universal precautions) Blood-stained body fluids Sharps b) Other first aid responsibilities 15 Appendix 4 Hepatitis B Immunisation Programme Introduction Under Control of Substances Hazardous to Health (COSHH) Regulations 2002 requirements: If a risk assessment shows that there is a risk of exposure to biological agents, and effective vaccines exist, then provision should be made to determine whether an employee is already immunised, and vaccination should be offered to those not already immunised. As with all control measures, vaccination needs to be checked and reviewed and boosters provided where deemed necessary. It is recommended that immunity of employees is assessed before or after vaccination to provide an indication as to the necessity and effectiveness of the vaccination and inform the risk assessment as to whether additional control measures are required for that individual or work activity. Final decisions on immunisation should be made on the basis of a local risk assessment. In settings where the client’s behaviour is likely to lead to significant exposures on a regular basis (e.g. biting), the Department of Health “The Green Book” indicates that it would be prudent to offer immunisation to staff even in the absence of documented Hepatitis B transmission. Employees are at liberty to refuse vaccination, but any refusal should be considered as part of the risk assessment - since additional controls may be necessary - and considered with regards to the type of work assigned to the individual. Immunisation programmes must be provided by appropriately qualified providers e.g. occupational health services or GPs. 16 Immunisation Schedule Generally the schedule for Hepatitis B, consists of three doses, with or without a fourth dose. Time Description Rationale Written consent sought. Medical history and Primary vaccine1 Month 1 Primary vaccine 2 Month 2 Primary vaccine 3 Month 6 Determines individual response to vaccine and measures antibody titre level i.e. immune / nonimmune Post vaccine blood test Post vaccine (reinforcing) booster dose Non-responders - (non immune) - will be followed up on an individual basis and further vaccination or blood tests may be offered. Month 8 In accordance with “The Green Book” and if no post exposure vaccine given prior to this date. Year 5 Managers may only be informed if an employee is immune or non-immune. No individual blood tests results or reasons for further blood tests will be provided to protect and maintain the medical confidentiality of the individual. 17 Appendix 5 Flow Chart - Guidance on management of incidents involving potential exposure to a blood-borne viruses Incident / accident potentially involving BBV: Skin puncture from sharp Human bite or scratch braking the skin Blood/body fluid splash or contamination of open wound, eyes or mouth. First Aid treatment: Encourage wound to gently bleed under running water / wash wounds copiously with running water Do not scrub or suck site Contact OH provider: Determine current immune status of the recipient (injured person): Immune or Non - immune Attend local A&E clinic as soon as possible (ideally within 1 hour and no later than 48 hours): Seek specialist advice / treatment from microbiologist / virologist Ensure blood sample collected for storage Individual prophylaxis treatment and follow up care is determined by specialist: Inform OH provider18/ GP of outcome. Complete Accident/Incident Form (HS157) RIDDOR reporting if appropriate