FIRST SEIZURE REFERRAL FORM
advertisement

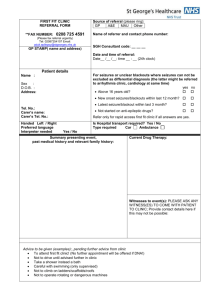
First seizure referral form Please send if you have a patient with a first seizure and a suspected diagnosis of epilepsy PATIENT DETAILS Name Date of Birth Hospital Number Address (use label) *Contact Number * essential as appointments are at short notice REFERRAL DETAILS Date Referer Area/ Contact number DETAILS Description of what occured, treatment given, response, medical history, medications and any other relevant details Please send fax to: FAO Rebecca Case/Sarah Kerley Epilepsy nurse specialists Wessex Neurological Centre Southampton General Hospital Telephone: 023 8120 8623 Fax number: 023 8120 8793 Or email form to: epilepsyspport@uhs.nhs.uk