aHUS/DDD Genetic Evaluation Pre

[Date]
[Insurance Company]
[Address 1]
[Address 2]
[City State Zip]
Re: [Patient Name]
Insurance ID: [ID #]
DOB: XX/XX/XXXX
To whom it may concern,
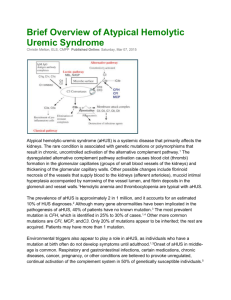
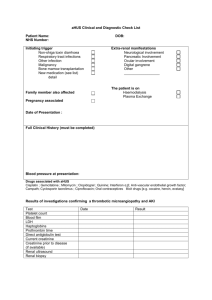
This letter is sent in request of coverage for comprehensive genetic testing for atypical hemolytic uremic syndrome (aHUS) for [Patient Name], XX/XX/XXXX, a [Age] year old [gender]. This patient presents with [Symptomatology, such as anemia, thrombocytopenia, organ dysfunction, especially renal impariment OR describe family history], raising concern for an underlying genetic cause of aHUS. Molecular diagnostic testing is necessary as determination of a pathogenic genetic variant will direct appropriate medical management for this individual and his/her family. aHUS is a disease characterized by non-immune hemolytic anemia, thrombocytopenia, and end-organ dysfunction, most commonly renal impairment. Many cases of aHUS are caused by uncontrolled activation of the complement system; both familial and sporadic forms of aHUS can be caused by complement-related genetic mutations.
1
Loss of function mutations in inhibitors of the complement system, including complement factor H (CFH), complement factor I (CFI), membrane cofactor protein (MCP/CD46), complement factor H-related proteins (CFHR1, CFHR3, CFHR4,
CFHR5), thrombomodulin (THBD), and C4b binding protein (C4BP), as well as gain of function mutations in complement factor B (CFB) and complement component 3 (C3) are associated with aHUS. Mutations in the epsilon isoform of diacyl glycerol kinase (DGKε) have also been associated with aHUS.
2 Multiple mutations , including novel sequence variants, have been reported in individuals with aHUS 3,4,5 , supporting the utility of comprehensive testing for genetic causes of aHUS, as opposed to single gene analysis or targeted testing for previously reported variants.
Short-term response to plasma therapy, outcome after kidney transplant, and overall prognosis have been shown to correlate with the gene affected 3 , therefore, genetic testing of aHUS patients is useful to guide clinical management.
The following testing is required:
Test name: aHUS/DDD Genetic Evaluation (1200)
CPT code: 81479
Ordering Physician: [Provider Name]
Provider Institution: [Ordering Institution]
Diagnosis code: [Diagnosis code]
The testing will be drawn and billed through [Ordering/billing institution]. This test is performed by BloodCenter of
Wisconsin, a fully licensed, CLIA-certified, CAP-accredited clinical laboratory approved for high complexity testing; this test is not an experimental or an investigational assay. .
From BloodCenter of Wisconsin
Created: 04/04/2014
If additional information is required, please contact us at [Phone number]. Thank you for your time and attention to this matter.
Sincerely,
[Name of Ordering Physician]
References:
1. Loirat, C. and Frémeaux-Bacchi, V: Atypical hemolytic uremic syndrome, Orphanet Journal of Rare Diseases 2011, 6:60 doi:10.1186/1750-1172-6-60
2. Lemaire, M, et al: Recessive mutations in DGKE cause atypical hemolytic-uremic syndrome Nature Genetics May 2013,
Vol 45 No. 5: 531-536
3. Noris, M, and Remuzzi, G: Atypical Hemolytic–Uremic Syndrome, N Engl J Med 2009; 361:1676-1687
4. Moore, I, et al.: Association of factor H autoantibodies with deletions of CFHR1, CFHR3, CFHR4, and with mutations in
CFH, CFI, CD46, and C3 in patients with atypical hemolytic uremic syndrome Blood January 14, 2010 vol. 115 no. 2 379-387
5. Bu, F., et al. Comprehensive Genetic Analysis of Complement and Coagulation Genes in Atypical Hemolytic Uremic
Syndrome. J Am Soc Nephrol 25: 55–64, 2014. doi: 10.1681/ASN.2013050453
From BloodCenter of Wisconsin
Created: 04/04/2014