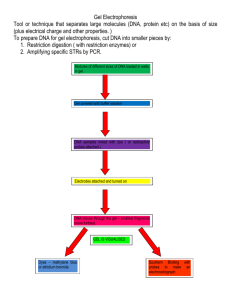
This in situ gel floating drug delivery system which undergoes sol to

TITLE PAGE
1.
Sustained release floating in situ gel-review
2.
AUTHORS:
Vyoma shah S, Master of Pharmacy (M.Pharm), affiliated to shree dhanvantary
Pharmacy college Email Id: vyoma13shah@gmail.com
Manish goyani B. Master of Pharmacy (M.Pharm), affiliated to shree dhanvantary
Pharmacy college. Email Id: smgoyani@gmail.com
Department of Pharmaceutics, shree dhanvantary Pharmacy college, kim, Gujarat
Address:-
24-Shree laxmi bunglows, Nr- Pragti Nagar Society,
Vesu , surat
Tel No. 9033128683,
Email Id: vyoma13shah@gmail.co
ABSTRACT
In recent years oral dosage form, liquid dosage forms are more prone to low bioavailability because of their quick transit from the stomach. In sustained release formulation of an oral liquid formulation among that Floating in situ gel is most beneficial for prolonged gastric residence time of drugs in GI tract. which helps to reduce dose frequency, improve patient compliance and convenience, The formation of gels depends on factors like temperature change, pH change, ionic cross linking and ultra violet irradiation, from which the drug gets released in a sustained manner. The oral delivery of drugs having narrow absorption window in the gastrointestinal tract with conventional dosage forms due to incomplete drug release and short residence time at absorption site. To overcome this drawback and to improve the oral absorption of these drugs, in situ gel is most beneficial.
Gel dosage forms are widely used as drug delivery systems to sustained drug release.
Based of manufacturing, this formulation is less complex, lowers the investment and manufacturing cost. This article contains approaches, biodegradable polymers, marketed preparations, and patents.
Key Words:
In situ gel, sustained release, biodegradable polymers, floating drug delivery.
INTRODUCTION. (1-2)
In situ gelling system is a polymeric drug delivery system by using biodegradable polymers which have sol to gel transition properties like gellan gum, sodium alginate,
Xyloglucan, low methyl pectin, chitosan, poly DL-lactide-coglycolide and poly caprolactone. This system remains in solution form at room temperature and converted in to gel form when it contact with the biological fluid by several stimuli like change in temperature, pH and ionic cross-linking. In situ gelling formulation administered through different routes like oral, ophthalmic, nasal, parentral and vaginal. Gastro retentive systems such as floating systems, mucoadhesive, high-density, expandable systems have been developed, thaus they provide sustained delivery of drugs with prolonged gastric residence time. Gastro-retentive floating system help to increase the bioavailability of drug compared to conventional dosage form Gel formed from in situ gelling system, being less dense than gastric fluids, it floats over the stomach and produce gastric retention of drug. Gastro-retentive in situ gelling floating system helps to achieve combined advantages of both
•
Solutions - such as ease of administration.
•
Floating gels - prolonged residence time in gastrointestinal tract.
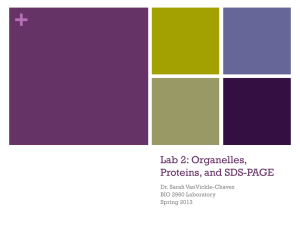
FIGURE 1:- FORMATION OF IN SITU GEL
GASTRO RETENTIVE DRUG DELIVERY SYSTEM
Gastro retentive drug delivery is an approach to prolong gastric retention of drugs, thereby used as site specific drug delivery for gastrointestinal tract.
APPROACHES FOR GASTRO RETENTIVE DRUG DELIVERY SYSTEM (2-4)
1. High density system
2. Low density system/ Floating system
I) Effervescent system/gas generating system
II) Non effervescent system a) Swelling or expanding system b) Inherently low density system
3. Mucoadhesive system
4. Modified shape system
5. Magnetic system
1. High density system
This system has a density larger than gastric juice (> 1.4 g/ml), due to which it settles down to the bottom of the stomach, below the pylorus and release the drug in the controlled manner. EX:-Iron oxide, barium sulphate and titanium oxide.
2. Low density or floating system
They have bulk density less than the gastric juice so remains buoyant in the stomach. This system is also called as hydrodynamic ally balanced system.
I) Gas generating system: This system not only increases the size of the system but also decreases its density, provides floating properties.
Types of gas generating system: i) Conventional matrix tablet ii) Layered matrix tablet iii) Core-coated tablets iv) Ion resin complexes
II) Non effervescent system a) Swelling or expanding system: This system uses a gel forming or swellable hydrocolloid such as cellulosic e.g. HPMC; polysaccharides e.g. guar gum and synthetic polymer eg: carbomer and PEO. This system swells on contact with gastric fluid and due to air entrapment and become larger in size which is high enough to prevent its exit from pyloric sphincter of the stomach. b) Inherently low density system: It can be achieved in two ways: a. Hollow microsphere/ microballoons. b. Low density materials: Low density polymers are used in this system to prepare floating drug matrices e.g. polypropylene foam powder, matrix forming polymers. This system provides excellent in vitro floating behaviour.
3. Mucoadhesive system
Bioadhesive polymers are used in this system like carbomer, chitosan for coating of dosages form or it adhere to the gastric mucosa. An advantage of this system is the intimate contact with mucosa leading to short pathways for locally acting drugs like drugs against H.Pylori
.
4. Modified shape system
This system unfolds to a larger size which limits its passage through pyloric sphincter. In this case drugs are incorporate in geometric shape like tetrahedron, cloverleaf disc, ring, spiral etc. This system consists of one erodible polymer, one non-erodible and drug incorporate in the polymer matrix.
5. Magnetic system
It involves incorporation of small magnet inside the matrix system and application of another magnet on the abdomen region externally. The real applicability of such systems is doubtful because the desired results can be achieved only when magnet position is selected with very high precision.
BENEFITS OF GASTRORETENTIVE DRUG DELIVERY SYSTEM (GRDDS):
1. The GRDDS are advantageous for drugs absorbed through the stomach e.g. ferrous salts and for drugs meant for local action in the stomach and treatment of peptic ulcer disease e.g. antacids.
2. The efficacy of the medicaments can be increased utilizing the sustained release.
3 .
When there is vigorous intestinal movement and a short transit time as might occur in certain type of diarrhoea, poor absorption is expected under such circumstances it may be advantage drug in gastro retention to get a relatively better response.
4 . GRDDS provides advantages such as the delivery of drugs with narrow absorption windows in the small intestinal region. e.g. verapamil Hydrochloride.
5. The GRDDS are not restricted to medicaments, which are principally absorbed from the stomach. Since it has been found that these are equally efficacious with medicaments which are absorbed from the intestine e.g. Chlorpheniramine maleate.
6. Improvement of bioavailability : Furosemide has poor bioavailability because its absorption is restricted to upper GIT. This was improved by formulating its floating dosage form. The floating system containing furosemide exhibit 42.9% bioavailability as compared to 33.4% shown by commercial tablet and 27.5% shown by enteric coated tablet.
7. Reduction in plasma level fluctuations: The reduced plasma level fluctuations results from delayed gastric emptying. For example bioavailability of standard madopar was found to be 60-70%, and the difference in the bioavailability of standard and HBS formulations was due to the incomplete absorption.
8. Reduction in the variability in transit performance: Floating dosage forms with sustained release characteristics are useful in reducing the variability in transit performance. For example formulating tacrine as Hydro dynamic balance system (HBS) dosage form reduces its gastrointestinal side effects in Alzheimer’s patients.
9. Enhancement of therapeutic efficacy: Floating systems are particularly useful for acid soluble drugs that are poorly soluble or unstable in intestinal fluids. For example bromocriptine used in the treatment of Parkinson’s disease have low absorption potential that can be improved by HBS dosage form and thus itstherapeutic efficacy could be enhanced.
10. Eradication of Helicobacter pylori: H.pylori
is responsible for chronic gastritis and peptic ulcers. This bacterium is highly sensitive to most antibiotics, and its eradication from patients require high concentrations of drug to be maintained within gastric mucosa which could be achieved by floating system.
POTENTIAL DRUG CANDIDATES FOR FLOATING DRUG DELIVERY
SYSTEM (3)
Drugs which are locally active in the stomach e.g. misoprostol, antacids etc.
Drugs which have narrow absorption window in gastrointestinal tract (GIT) e.g. L-
DOPA, P-amino benzoic acid, furosemide, riboflavin etc.
Drugs those are unstable in the intestinal or colonic environment e.g. captopril, metronidazole.
Drugs that disturb normal colonic microorganism e.g. antibiotics against
Helicobacter pylori.
Drugs that exhibit low solubility at high pH values e.g. diazepam, chlordiazepoxide, and verapamil hydrochloride.
DIFFERENT APPROACHES FOR IN SITU GELLING SYSTEM. (5-7)
1. Temperature-sensitive.
2. pH-sensitive.
3. Ion-sensitive.
4. Dilution-sensitive.
5. Electrical signal-sensitive.
6. Light-sensitive.
7. Glucose-sensitive.
1. Temperature-Sensitive.
Temperature is one of the most widely used stimuli for stimuli-sensitive in situ gels, because it is easy to control and has practical advantages both in vitro and in vivo. These formulations are liquid at room temperature (20-25°C) and undergo gelation when comes in contact with application site (35-37°C), due to an increase in temperature. Temperaturesensitive in situ gel undergo a volume phase-transition or a sol–gel phase-transition at a critical temperature, namely, lower critical solution temperature (LCST) or upper critical solution temperature (UCST). The LCST polymers exhibit a hydrophilic-to-hydrophobic transition with increasing temperature, whereas the UCST systems undergo the opposite transition. Typical LCST polymers include poly(N-isopropylacrylamide) (PNIPAM), poly(N,N-diethylacrylamide) (PDEAM), poly(vinyl ether) (PVE), poly(Nvinylalkylamide) (PNVAAM), polyphosphazene derivatives and poly(N-(2-
hydroxypropyl) methacrylamide mono/di lactate) (PHPMAM-mono/dilactate).
Poloxamers are the most commonly used thermosetting polymers in in situ gel forming drug delivery.
Three principle mechanisms have been proposed to explain the sol-to-gel transition after an increase in temperature.
Gradual dissolvation of the polymer,
Increased micellar aggregation, and
The increased entanglement of the polymeric network.
Thermo reversible gels can be prepared with naturally occurring polymers. Most natural polymer aqueous solutions form a gel phase when their temperature is lowered. Classic examples of natural polymers exhibiting a sol–gel transition include gelatin and carrageenan. At elevated temperatures, these polymers adopt a random coil conformation in solution. Upon cooling, a continuous network is formed by partial helix formation.
2. pH-Sensitiv. pH is another important environmental parameter for drug delivery systems, because the pH change occurs at many specific or pathological body sites, such as stomach, intestine, endosome, lysosome, blood vessels, vagina and tumor extracellular sites. These formulations are polymeric dispersion in aqueous system which undergoes spontaneous gelation in response to change in pH after application at the target site. Generally the ionic polymers like polyacrylamide, polyacrylic acid, and poly meth acrylic acid are used for the preparation of pH sensitive in situ gels. All the pH-sensitive polymers acidic or basic groups that either accept or release protons in response to changes in environmental pH.
Swelling of in situ gel increases as the external pH increases in the case of weakly acidic
(anionic) groups, but decreases if polymer contains weakly basic (cationic) groups.
3. Ion-Sensitive.
In this type of in situ hydrogels, the sol-to-gel transition is induced by the presence of mono or divalent cations such as Na + , K + , Ca ++ , and Mg ++ ions. Naturally occurring anionic polymers like gellan Gum, sodium alginate, carragenan, and xyloglucans are having the characteristics property of cationic-induced gelation. Gellan gum commercially available as Gelrite® is an anionic polysaccharide that undergoes in situ gelling in the presence of mono- and divalent cations, including Ca
2+
, Mg
2+
, K
+
and Na
+
.
4. Dilution-Sensitive.
This type of hydrogel contains polymer that undergoes phase transition in presence of higher amount of water. By having a system undergoing phase transition as a consequence of dilution with water a higher amount of polymer can be used. E.g:- Lutrol F68
5. Electrical Signal-Sensitive.
Hydrogels sensitive to electric current are usually made of polyelectrolytes such as the pHsensitive hydrogels. Electro-sensitive hydrogels undergo shrinking or swelling in the presence of an applied electric field. Chitosan gels as matrices can be used for electrically modulated drug delivery.
6. Light-Sensitive.
Light-sensitive hydrogels can be used in the development of photo-responsive artificial muscle or as the in situ forming gels for cartilage tissue engineering. Polymerizable function groups and their initiator like ethyl eosin and camphor Quinone can be injected in to tissue and applied electromagnetic radiation used to form a gel by enzymatic processes.
For that long ultraviolet wavelengths are used.
7. Glucose-Sensitive.
Intelligent stimuli-responsive delivery systems using hydrogels that can release insulin have been investigated. Cationic pH-sensitive polymers containing immobilized insulin and glucose oxidase can swell in response to blood glucose level releasing the entrapped insulin in a pulsatile fashion. Another approach is based on competitive binding of insulin or insulin and glucose to a fixed number of binding sites in concanavalin A, where insulin is displaced in response to glucose stimuli, thus functioning as a self-regulating insulin delivery system. An alternative route through phenylborate-poly(vinyl alcohol) polymers is also possible.
POLYMERIC SYSTEMS FOR ORAL ADMINISTRATION
Pectin:
Pectin is a complex polysaccharide comprising mainly esterified D-galacturonic acid residues in an a-(1–4) chain. The acid groups along the chain are largely esterified with methoxy groups in the natural product. The hydroxyl groups may also be acetylated.
Pectin gelation characteristics can be divided into two types: high-methoxy and lowmethoxy gelation. Gelation of high methoxy pectin usually occurs at pH < 3.5. Lowmethoxy pectin is gelled with calcium ions and is not dependent on the presence of acid or high solids content.
Gellan gum:
Gellan gum is an anionic deacetylated exocellular polysaccharide secreted by
Pseudomonas elodea with a tetrasaccharide repeating unit of one α-L-rhamnose, one β-Dglucuronic acid and two β-D-glucuronic acid residues. It is a water soluble polysaccharide.
It forms a gel via formation of double helices, followed by their ionic cross-linking.
Sodium alginate:
Sodium alginate is a salt of Alginic acid - a linear block copolymer polysaccharide consisting of β-D-mannuronic acid and α-L-glucuronic acid residues joined by 1,4glycosidic linkages. Aqueous solutions of alginates form firm gels on addition of di- and trivalent metal ions. The results indicated that the alginates form compact structures when the ionic radical of the cation are lower. Sodium alginate has been employed in the preparation of gels for the delivery of biomolecules such as drugs, peptides and proteins.
Xyloglucan:
Xyloglucan is a polysaccharide derived from tamarind seeds and is composed of a (1-4)-
β-D-glucan backbone chain, which has (1-6)-α-D xylose branches that are partially substituted by (1-2)-β-D-galactoxylose. Xyloglucan is composed of heptasaccharide, octasaccharide and nonasaccharide oligamers, which differ in the number of galactose side chains. Although xyloglucan itself does not gel, dilute solutions of xyloglucan which has been partially degraded by galactosidase exhibit a thermally reversible sol–gel transition on heating.
FORMULATION
To prepare a polymeric solution in deionised water
Finally, preservative add and stored the solution.
Heat the polymer solution at 60
0
C with stirring
Then cool the solution at 40
0
C calcium carbonate and drug dissolved in above polymeric solution with stirring
FORMATION OF IN- SITU GELATION MECHANISM (5-8)
These are aqueous liquid solutions before administration, but gel under physiological conditions. Several possible mechanisms lead to in-situ gel formation are :-
Ionic cross-linkage, pH change & temperature modulation. Polymer solutions of gellan, pectin & Na-alginate etc contains divalent- ions complexed with Na-citrate that are breakdown in acidic environment of stomach to release free divalent ions (ca+2).causes the in situ gelation of orally administered solution. It involves formation of double helical junction zones by aggregation of double helical segments to form dimensional network by complexation with cations & hydrogen bonding with water.
ADVANTAGES OF IN SITU FORMING POLYMERIC DELIVERY. (5- 7)
Ease of administration
To increase local bioavailability
Reduced dose frequency
Improved patient compliance
Its production is less complex and so lowers the investment.
APPLICATION OF STOMACH SPECIFIC FLOATING IN SITU GEL (2, 3, 5, 10, 11, 12)
To Increased absorption of Drugs which are mainly absorbed from upper part of stomach get prolonged contact time, at their site of maximum absorption. So to increase the extent of absorption
As the absorption of the drug from stomach is increased, bioavailability of the drug enhanced, remarkably. Increase in the gastric transit time also causes an increase in the bioavailability of drug.
As drug remains in the stomach till the complete release, frequency of the adverse effect on the colon is decreases.
Drugs which are absorbed from the stomach get enough residence time for absorption rate occurs. Furthermore, local action of the drug in prolonged, so less amount of dose is required.
APPLICABILITY OF IN SITU GEL DRUG DELIVERY (15-16)
A. Parenteral Delivery
One of the most obvious ways to provide sustained release medication is to place the drug in a delivery system and inject or implant the system into the body tissue.
Thermoreversible gels mainly prepared from poloxamers are predominantly used. The suitability of poloxamer gel alone or with the addition of hydroxypropylmethylcellulose
(HPMC), sodium carboxy- methylcellulose or dextran was studied for epidural administration of drugs in vitro. Pluronic F127 gels which contained either insulin or insulin-PLGA nanoparticles can be useful for the preparation of a controlled delivery system. Likewise, poloxamer gels were tested for intramuscular and subcutaneous administration of human growth hormone or with the aim to develop a long acting single dose injection of lidocaine. A new class of injectable controlled release depots of protein which consisted of blends of Pluronics with poly(D, L-lactide)/1-methyl- 2-pyrrolidone solutions is developed. Some other thermosensitive hydrogels may also be used for
parenteral administration. ReGel® (triblock copolymer PLGA-PEG-PLGA) was used as a drug delivery carrier for the continuous release of human insulin.
B. Ocular Delivery
The efficacy of ophthalmic hydrogels is mostly based on an increase of ocular residence time via enhanced viscosity and mucoadhesive properties. Since resulted swollen hydrogel is aqueous based, it is very comfortable in the human eye. Among these polymers, in situ gels are preferred since they are conveniently dropped in the eye as a solution, where undergo transition into a gel. Thermosensitive, specific ion sensitive or pH-sensitive hydrogels have been examined for their potential as vehicles for ocular drugs. Poloxamers as thermogelling polymers could be applicable for the development of effective ophthalmic drug delivery. In order to reduce the concentration of polymer and/or to achieve a phase transition temperature higher than room temperature (25°C) and gelling at precorneal temperature (35°C), the combining Pluronic® analogues or the addition of further polymer, e. g. poly ethylene glycol , Poly acralic acid, methylcellulose (MC),
HPMC, CMC is often necessary. An alternative in situ gelling material of natural origin, xyloglucan, was evaluated for the sustained ocular delivery of pilocarpine and timolol .
Ion-sensitive polymers belong to the mainly used in situ gelling materials for ocular drug delivery. Slightly viscous gellan gum solutions in low concentrations (<1%) show markedly increase in apparent viscosity, when introduced into presence of a physiological level of cations, without requiring more ions than 10–25% of those in tear fluid. The precorneal contact times for drugs can thus be extended up to 20-h. Gellan containing formulations of pilocarpine HCl allowed reduction of drug concentration from 2% to 0.5% obtaining the same bioavailability. The ability of gel formation at physiological Ca2+ levels was used in case of alginic acid as well. Presence of this polymer significantly extended the duration of the pressure reducing effect of pilocarpine to 10-h and carteolol to 8-h allowing only once a day administration in case of carteolol.
C. Rectal Delivery
The rectal route may be used to deliver many types of drugs those are formulated as liquid, semi-solid (ointments, creams and foams) and solid dosage forms (suppositories).
Conventional suppositories often cause discomfort during insertion. In addition, suppositories are unable to be sufficiently retained at a specific position in the rectum, sometimes they can migrate upwards to the colon, that makes them possible for drug to undergo the first-pass effect. Novel in situ gelling liquid suppositories with gelation temperature at 30–36°C were developed using poloxamer 407 and/or poloxamer 188 to
confer the temperature-sensitive gelation property. It is also possible to develop a vehicle for short chain fatty acid enemas using 18% poloxamer 407 solution. After gelation at
37°C, it allows control release of short chain fatty acids. Thermoreversible xyloglucan gels are useful for rectal drug delivery.
D. Vaginal Delivery
Formulations based on a thermoplastic graft copolymer that undergo in situ gelation have been developed to provide prolonged release of active ingredients such as nonoxynol-9, progestins, estrogens, peptides and proteins. A mucoadhesive thermo sensitive gel containing combination of poloxamers and polycarbophil exhibited increased and prolonged antifungal activity of clotrimazole in comparison with conventional Poly ethylene glycol based formulation.
E. Peroral Delivery
The pH-sensitive hydrogels have a potential use in site-specific delivery of drugs to specific regions of Stimuli-sensitive hydrogels in controlled and sustained drug delivery the GI tract. Hydrogels made of varying proportions of Poly acrylic acid derivatives and cross-linked Poly ethylene glycol allowed preparing silicone microspheres, which released prednisolone in the gastric medium and showed gastroprotective property. Cross-linked dextran hydrogels with a faster swelling under high pH conditions, likewise other polysaccharides such as amidaded pectins, guar gum and inulin were investigated in order to develop a potential colon-specific drug delivery system. The formulations of gellan gum and sodium alginate both containing complexed calcium ions undergo gelation by releasing of these ions in the acidic environment of the stomach. Such formulations were developed for oral delivery of paracetamol.
F. DERMAL AND TRANSDERMAL DELIVERY
Thermally reversible gel of Pluronic F127 was evaluated as vehicle for the percutaneous administration of indomethacin. In-vivo studies suggest that 20% w/w aqueous gel may be of practical use as a base for topical administration of the drug. Poloxamer 407 gel was found suitable for transdermal delivery of insulin. The combination of chemical enhancers and iontophoresis resulted in synergistic enhancement of insulin permeation.
G. NASAL DELIVERY
An in-situ gel system for nasal delivery of mometasone furoate was developed and evaluated for its efficacy for the treatment of allergic rhinitis. Gellan gum and xanthan gum were used as in situ gel forming polymers. In-situ gel was found to inhibit the increase in nasal symptoms as compared to marketed formulation nasonex (mometasone
furoate suspension 0.05%). Intact ciliated respiratory epithelium and normal goblet cell appearance indicated from histopathology of rat nasal cavity proved that these formulations were safe for nasal administration. The formulation was in solution form at room temperature that transformed to a gel form when kept at body temperature. Animal experiments demonstrated hydrogel formulation to decrease the blood-glucose concentration by 40-50% of the initial values for 4-5 hour after administration with no apparent cytotoxicity. Therefore, these types of systems are suitable for protein and peptide drug delivery .
EVALUTION OF IN SITU GEL.
(8-15)
Determination of drug content: Certain weight of formulation equivalent to an amount of drug has to be dissolved in a suitable medium, stirred for required time, filtered and analysed for drug content. pH determination: The pH of solution can be determined using digital pH meter and the favourable conditions that facilitate in situ gelling can be identified. The influence of pH on the gelation of sol can be determined by using the medium of various pH values.
In-vitro gelling capacity: In general the gelling capacity of an in situ gel forming system can be determined by formulating a colour solution of in situ gelling system for visual observation. By adding the in-situ gelling formulation to a medium (simulating gastric fluid), various parameters like the time taken for in situ gel formation, its stiffness and the duration for which formed gel remains intact, can be estimated.
In-vitro buoyancy studies: After adding a fixed volume of in situ gelling formulation to a medium (simulating gastric fluid), the parameters like the time taken for the system to float over the surface of medium (floating lag time) and the time the formed gel constantly float over the surface of the dissolution medium (floating time) can be estimated.
In-vitro drug release studies: The release rate of drug from in situ gel can be determined using USP dissolution rate testing apparatus I (basket covered with muslin cloth) at 50 rpm. 900 ml of 0.1 N HCl can be used as dissolution medium and temperature of 37+0.5 o C can be maintained. 5 ml samples can be withdrawn at various time points for estimating the drug release using UV-Visible spectrophotometer. Same volume of fresh medium has to be replaced every time the sample is withdrawn. The drug release studies from in-situ gel can also be done using plastic dialysis cell.
Measurement of rheological property of sol and gel: Viscosity of the solution prepared using various concentrations of gelling agents can be determined by viscometers like
Brookfield viscometer, Cone & plate viscometer etc., Viscosity of the formed gel can also be determined to estimate the gel strength.
Water uptake study: Once the sol is converted to gel, it is collected from the medium and the excess medium was blotted using a tissue paper. The initial weight of thus formed gel has to be noted. Again the gel has to be exposed to the medium/distilled water and the same process is repeated for every 30 min to note down the weights of the gel at each interval after removing the excess amount of medium/distilled water, using filter paper.
The weight gain due to water uptake has to be noted from time to time. Effect of pH, concentration of gelling agent/cross linking agent on viscosity, in-situ gelation character, floating ability and drug release can be studied for in-situ gelling type of floating formulations.
Gel strength: This parameter is evaluated by using rheometer with a specified amount of solution form gel were prepared in a beaker. This beaker is raised so pushing the probe of rheometer through the gel. The change in the load on the probe can be measured as a function depth of merge of the probe below the gel surface.
Spread ability
For the determination of spread ability, excess of sample was applied between the two glass slides and was compressed to uniform thickness by placing 1000 g weight for 5 min.
Weight (50 g) was added to the pan and the time required for separating the two slides, i.e. the time in which the upper glass slide moves over the lower plate was taken as measure of spread ability (S).
Spread ability (g.cm/s) (S) = M×L/T
Where M = weight tide to upper slide L = length moved on the glass slide T = time taken
Sol-gel transition temperature and gelling time: Sol-gel transition temperature is the temperature at which the phase transition of sol meniscus is first noted when it kept in a sample tube at a specific temperature and then heated at a specified rate. Gel formation is indicated by a lack of movement of meniscus on tilting the tube. Gelling time is the required for first detection of gel formation of sol formulation.
MARKETED PRODUCTS: (10)
Liquid Gaviscon
Topalkan
Conviron
COMMERCIAL FORMULATIONS OF IN-SITU Gel (11)
Timoptic-XE
It is a timolol maleate ophthalmic gel formulation of Merck and Co. Inc., This formulation is available in two dosage strengths 0.25% and 0.5% in market. The pH of the solution is approximately 7.0, and the osmolarity is 260-330 mOsm. Each ml of Timoptic-XE 0.25% contains 2.5 mg of timolol (3.4 mg of timolol maleate). Inactive ingredients include gellan gum, tromethamine, mannitol, and water for injection and the preservative used is benzododecinium bromide 0.012%. Timoptic- XE, when applied topically on the eye, reduces the elevated, as well as normal intraocular pressure, whether or not accompanied by glaucoma.
AzaSite:
AzaSite is a marketed product of InSite Vision. AzaSite is a topical ophthalmic solution of azithromycin formulated in DuraSite (polycarbophil, edetate disodium, sodium chloride).
AzaSite is supplied as a sterile aqueous ophthalmic formulation designed for topical administration. The recommended initial dose of the drug is in still 1 drop in the affected eye(s) twice daily, eight to twelve hours apart for the first two days and then in still 1 drop in the affected eye (s) once daily for the next five days.
Pilopine HS :
Pilopine HS is a marketed product of Alcon Laboratories Inc. Pilopine HS (pilocarpine hydrochloride ophthalmic gel) 4% is a sterile topical ophthalmic aqueous gel which contains more than 90% water and employs Carbopol-940, a synthetic high molecular weight cross-linked polymer of acrylic acid, to impart a high viscosity.
Akten™:
Akten™ is an HPMC-based gel of lidocaine hydrochloride for ocular surface anesthesia.
Akten™ contains 35 mg of lidocaine hydrochloride per mL as the active ingredient.
Akten™ also contains Hypromellose, Sodium Chloride, and Purified Water as inactive ingredients. The pH may be adjusted to 5.5 to 7.5 with Hydrochloric Acid and/or Sodium
Hydroxide. The recommended dose of Akten™ is 2 drops applied to the ocular surface in the area of the planned procedure. Akten™ may be reapplied to maintain anesthetic effect.
Virgan:
Vigran is an ophthalmic antiviral that is indicated for the treatment of acute herpetic keratitis. The recommended dosing regimen for Virgan is 1 drop in the affected eye 5 times per day (approximately every 3 hours while awake) unti the corneal ulcer heals, and then 1 drop 3 times per day for 7 days. Virgan (ganciclovir) contains carbomer 974. The
carbomers are polyacrylic acid derivatives that impart high viscosity to their aqueous solutions at neutral pH (above their pKa values) due to ionization and hydration of the carboxyl groups.
Cytoryn
This is one of the Macromed's products, which is a novel, peritumoral, injectable depot formulation of interleukin-2 (IL-2) for cancer immunotherapy using Regel drug delivery system. It is a free flowing liquid below room temperature that instantly forms a gel depot upon injection from which the drug is released in a controlled manner. Cytoryn enhances the immunological response by safely delivering four times the maximum tolerated dose allowed by conventional IL-2 therapy. Cytoryn also activates the systemic antitumor immunity. Regel system stabilizes and releases IL-2 in its bioactive form.
CONCLUSION:
This in situ gel floating drug delivery system which undergoes sol to gel system transition in acidic stomach conditions to provide stomach specific release of drug for longer period of time. Such systems provide the advantage of better absorption of drugs which are absorbed from the upper part of stomach, as the gel remains in the stomach for longer duration. This leads to less frequent dosing and improved efficiency of treatment. By understanding the floating and gel forming behaviour of polymers we can look forward to studies the diffusion controlled release of drug which improve the gastric retention and bioavailability of pharmacologically active agents.
REFERENCE
1.
Monika Prajapati, Vishwanath Agrahari, Udai Vir Singh Sara. Gastro retentive floating in situ gel: An overview. The Global Journal of Pharmaceutical Research 2012, 1309-1321.
2.
Singh BM, Kim KH. Floating drug delivery systems: an approach to oral controlled drug delivery via gastric retention. Journal of Controlled Release, 2000 , 300, 235–259.
3.
Nayak AK, Ruma Maji, Biswarup Das, Gastro retentive drug delivery systems: a review.
Asian Journal of Pharmaceutical and Clinical Research, 2010 , 3, 2-10.
4.
Praveen nasa, sheefali mahant, deepika Sharma.
Floating systems: a novel approach towards gastro retentive drug delivery systems. International Journal of Pharmacy and
Pharmaceutical Sciences, 2010, 2 , 2 7.
5.
AV Mayavanshi, SS Gajjar. Floating drug delivery systems to increase gastric retention of drugs: A Review. Research J. Pharm. And Tech, 2008 , 4, 346-348.
6.
Rathod H, Patel V and Modasia M. In situ gel as novel approach of gastro retentive drug delivery .
Int J of Pharm & life Sci. 2010 , 1, 440-447.
7.
Panwar AS, Manoj Sharma. in-situ oral gel an advancement in pud: a review.
International Journal of Pharmaceutical and Medical Sciences , 2012, 2 , 51-78
8.
Aman Kant, Suchetha Reddy. In situ gelling system-review.
Pharmacology online . 2011,
2, 28-44.
9.
V. Bhavani Prasad, G.S.N. Koteswara Rao, B. Roja Rani. In-vitro and in-vivo evaluation tests for floating drug delivery systems. Int J Pharm, 2012 , 2,645-655.
10.
Bhimani RD, Patel JK, Patel VP. Devlopment and evalution floting in situ gel of clarithromycin. Int J of Pharm Res, 2011 , 3, 32-35
11.
Shreeraj Shah, Pratik Upadhyay, Darsh Parikh, Jinal Shah. In Situ Gel: A Novel Approach of gastro retentive Drug Delivery. Asian Journal of Biomedical and Pharmaceutical
Sciences, 2012 ,2, 01-08
12.
Jayswal BD, Yadav VT, Patel KN, Patel BA and Patel PA. Formulation and Evaluation of
Floating In Situ Gel Based Gastro Retentive Drug Delivery of Cimetidine. Int J of Pharm
& life Sci. 2012 , 1, 327-337.
13.
Lovenish Bhardwaj, Pramod Kumar Sharma and Rishabha Malviya. A Short Review on
Gastro Retentive Formulations for Stomach Specific Drug Delivery: Special Emphasis on
Floating In situ Gel Systems. African Journal of Basic & Applied Sciences, 2011, 3,1-3.
14.
Ying-Chen Chen, Hsiu-O Ho, Tzu-Yu Lee, Ming-Thau Sheu. Physical characterizations and sustained release profiling of gastro retentive drug delivery systems with improved floating and swelling capabilities. int j of pharm, 2012 ,1-8.
15.
Sudipta Ganguly, Alekha K. Dash. A novel in situ gel for sustained drug delivery and targeting. International Journal of Pharmaceutics, 2004 , 2, 83–92.
16.
Nirmal H.B, Bakliwal S.R., Pawar S.P. In-Situ gel: New trends in Controlled and
Sustained Drug Delivery System, 2010, 1399-1408.
TABLE 1
LIST OF PATENT:
Sr.
No.
1
Patent No
US20050063980
2
3
4
US5360793
US20020119941
US20110082221
5
6
7
8
9
10
FIGURE 1
US6777000B2
EP0706372A1
US5318780
EP1372606A2
EP 1635872 A2
EP1635871 B1
Formulations Inventors
Gastric composition
Rafting formulation raft antacid
In situ gel formation of pectin
In situ gelling system as sustained delivery for eye.
In situ gel formation of pectin
In situ gel for therapeutic use
Medical use of in situ formed gel.
In situ gel formation of pectin
In situ gel formation of pectin
In situ gelling drug delivery system
Gillian E. ccleston et al.
William J. Brooks et al.
Yawei Ni et al.
Claire haug et al.
Yawei Ni et al
John calters et al.
Vigas et al.
M. Kenneth yates et al.
Paul Asthon et al.
Paul Asthon et al.