CUSP for Safe Surgery: Improving Patient Safety
advertisement

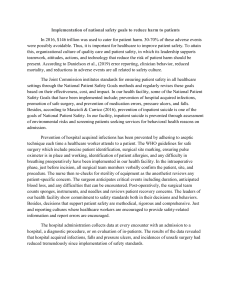
Science of Improving Patient Safety Fact Sheet: CUSP for Safe Surgery Why the science of safety matters1 1 in 25 people will undergo surgery 7 million (25%) in-patient surgeries followed by complication, including surgical site infections 1 million (0.5 – 5%) deaths following surgery 50% of all hospital adverse events are linked to surgery AND are avoidable Why medical errors happen Patient safety is a property of the healthcare system; not individuals Systems do not catch mistakes before they reach the patient Defects in the healthcare system that lead to complications vary widely among hospitals Surface defects that are leading to complications 1. Tap into the wisdom of frontline 2. Audit local performance to staff. Ask frontline staff how the next identify opportunities to improve. patient will be harmed and what we can do to prevent it. 3. Create your own ‘bundle’ of care and focus on improving the system to prevent complications. Consider your work area: What system-level factors put patients at risk? Remember that every system is perfectly designed to achieve the results it gets!! Work with your teams to apply principles of safe design The 3 principles of safe design you can apply in your units: 1. 2. 3. Standardize care and reduce complexity: Make it easier for providers to do the right thing Create independent checks (at least two sets of eyes trained differently to look at the same picture) Learn when things go wrong by asking: a. What happened? b. Why did it happen? c. What will we do to prevent this from recurring? d. How will we know that our intervention worked? Theseii.principles apply to technical and team work! Tap into the wisdom of your team members for best results. Where’s the evidence? Colorectal NSQIP SSI Rate at Hopkins2 Quarter 4 CUSP kickoff Antibiotic deficiencies addressed 42% Quarter 3 Skin preparation protocol Pre-op wash clothes Quarter4 Briefing/Debriefing Mechanical bowel prep with oral Quarter1 Pre-op warming Enhanced sterile technique 29% 26% Intervention checklist 24% 21% 21% 20% 19% 18% 17% 16% 15% Goal 15% 17% 12% 19% 14% This approach has also been used to achieve large sustainable reductions in CLABSI 3,4 and VAP5! What now? Educate staff on the Science of Safety (watch the video here!) Use the Perioperative Staff Safety Assessment to ask staff how the next patient will be harmed, why will the next patient develop an SSI, and what they think we can do to prevent it. You may be surprised by the answers you get! References 1. 2. 3. 4. 5. http://www.who.int/patientsafety/challenge/safe.surgery/en/ Wick et al. Implementation of a Surgical Comprehensive Unit-Based Safety Program to Reduce Surgical Site Infections. J Am Coll Surg. 2012;215 (2). Pronovost P, Needham D, Berenholtz S, et al. An Intervention to Decrease Catheter-Related Bloodstream Infections in the ICU. N Engl J Med. 2006; 355:2725-2732. Pronovost P, Goeschel C, Needham D. Sustaining Reductions in Catheter Related Bloodstream Infections in Michigan Intensive Care Units: Observational Study. BMJ 2010;340:c309. Berenholtz S, Pham J, Thompson D, et al. Collaborative Cohort Study of an Intervention to Reduce Ventilator-associated Pneumonia in the Intensive Care Unit. Infect Control Hosp Epidemiol. 2011; 32(4):305–314.