CT Scan/IVP Consent Form: Risks, Benefits, & Alternatives

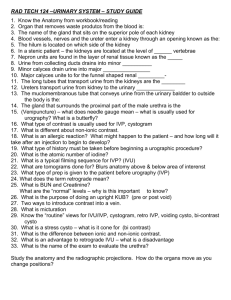
Name of Practice
COMPUTED TOMOGRAPHY (CT)
SCAN OR INTRAVENOUS
Medical Record # ___ _______________________
Name: __________________________________
Date of Birth: ____________________________
PYELOGRAM (IVP)
Website Sample CONSENT FORM
Sex: M F
A.
Interpreter Needs/Signature
Is an Interpreter service required? Y N
Interpreter’s statement:
I have translated this consent to the patient and/or his or her legal representative.
Name of interpreter: ______________________________
Signature : __________________________________ Date: _____________________
B.
Condition and Treatment
The doctor has explained you have the following condition:
_____________________________________________________________________________________________
This condition requires the following procedure: Right Side Left Side Not applicable
_____________________________________________________________________________________________
What is a CT scan? It is a computer processed x-ray that produces pictures that are “slices” of the area that is scanned. This allows the user to see inside without cutting.
What is an IVP? This is an x-ray that provides pictures of the kidneys, bladder, ureters and the urinary tract. The
IVP can show the size, shape and position of the organs and look at how the kidneys are functioning. An iodine dye is injected through an IV catheter so the areas are easier to see. You must tell the nurse/physician if you are allergic to shellfish which contains iodine.
C.
Benefits of Treatment
An IVP is done to look for problems within the urinary tract, bleeding, kidney stones, cause of recurring urinary tract infections, tumors or the cause of ongoing back pain.
D.
Alternatives
Your doctor has discussed alternative options with me and I have had the benefits and risks of these alternatives explained to me.
E.
Risks
It is important to tell your doctor if you are or might be pregnant. X-rays to a fetus may have consequences to the unborn child.
If you are allergic to iodine (found in shellfish) which is used in the contrast material you may experience an allergic reaction. The reactions may be mild from itching, to hives, shortness of breath, difficulty swallowing or respiratory distress/failure. Report any of these symptoms immediately to the technician!
Pain, bleeding, bruising, redness or swelling at the IV site.
The IV dye that contains iodine may cause kidney damage in those with poor kidney function. It is important to tell your nurse/physician if you have diabetes, or are taking medication for diabetes or
have had kidney problems in the past.
1
F.
Consent From Patient or Legal Representative
My medical condition and the proposed treatment, including alternatives, as well as additional treatment if the doctor finds something unexpected has been explained to me. I understand the risks, including the risks specific to me.
I understand there is no guarantee the procedure will improve my condition.
I understand I must tell the technician or nurse if I have any of the above reactions to the iodine dye during the procedure.
I understand I must tell the nurse/physician or technician before the CT scan if I am or think I may be pregnant,
breast feeding or have had any kidney problems or if I am taking any medications for diabetes.
I GIVE CONSENT FOR Dr. OR THEIR DESIGNEES _________________________TO PERFORM A CT SCAN WITH A
POSSIBLE IVP.
I have had all my questions answered to my satisfaction and have read the above information. IF YOU HAVE ANY
QUESTIONS ABOUT THE PROCEDURE, INCLUDING THE RISKS, ASK YOUR DOCTOR BEFORE SIGNING THIS
CONSENT FORM. YOU MAY REVOKE THIS CONSENT AT ANY TIME FOR ANY REASON.
_______________________________________ _________________ _______________
Patient/Legal Representative Signature Time Date
_______________________________________
Witness Signature
_______________________________________
Physician’s Signature
____________________
Time
_____________________
Time
_______________
Date
________________
Date
2