Current IRB Protocol approved for OPQC by CCHMC
advertisement

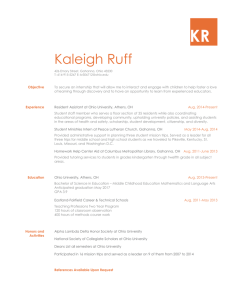
12/20/2013 I. ABSTRACT The Ohio Perinatal Quality Collaborative (OPQC) is a learning network that implements ongoing quality improvement collaborative projects with perinatal health care practitioners and providers in Ohio including physicians, nurses, other clinicians, parents, payers and policy makers. The OPQC mission is “through collaborative use of improvement science methods, reduce preterm births and improve perinatal and newborn outcomes in Ohio as quickly as possible.” OPQC membership is at the institution level; each participating institution identifies a lead physician and nurse manager as well as additional clinical faculty and staff who work as members of local sitespecific and topic-specific improvement team(s). The James M. Anderson Center for Health Systems Excellence at Cincinnati Children’s Hospital Medical Center (CCHMC) serves as the administrative hub and data coordinating center for the OPQC, meaning that the contract funding is issued to the Anderson Center at CCHMC, central project management staff are employed by the institution, and data sets are submitted to the Anderson Center for analysis. The Division of Biomedical Informatics at has received separate funding to develop and administer the perinatal quality improvement database. Participant sites share limited data sets containing patient-level data with the Anderson Center. The purpose of this data sharing is to facilitate quality improvement activities. In addition, the network has a research interest in understanding whether and how the use of improvement science and collaborative projects is able to improve outcomes at a population level. Encrypted data is transferred electronically via a secure, password-protected, web-based extranet from participating institutions to the Anderson Center. The HIPAA-specified, “limited data set” procedures are used as part of all OPQC improvement projects. The Anderson Center’s data team uses statistical process control (SPC) methods and develops run charts and control charts that contain only aggregate and de-identified data. Site-specific graphs are provided to each of the participating institutions. Each improvement team has visibility only to their sitespecific graphs and to graphs that include aggregate data for the all sites participating in a given project. While the Anderson Center will receive limited data sets, the graphs produced and returned to teams contain only de-identified aggregate data. OPQC will also continue to work with the Ohio Department of Health Office of Vital Statistics to secure access to de-identified birth registry data for specific projects as needed. Page 1 of 19 Version 1 12/20/2013 OPQC will continue to engage in multiple simultaneous improvement projects with new projects starting and old projects ending depending on success achieved and resources available for taking on new projects. All projects will use only limited data sets. Improvement efforts will occur concurrently with care. For example, if projects are designed to assure that physician orders are reliably followed, improvement efforts will occur simultaneously during the care of the patients for whom these orders are made. Lessons learned as part of OPQC improvement efforts will be published in peer-reviewed journals. II: BACKGROUND Evidence-based guidelines exist to address factors that can improve pregnancy outcomes. These guidelines are not implemented consistently. Ohio ranks 40th in Black prematurity rates (2010) and 47nd in infant mortality (2011) and 49th in Black infant mortality (2011). In Ohio, 60-70% of deaths in the first year of life are associated with extreme prematurity (<29 weeks gestational age). In addition to the markedly elevated mortality risk, it is estimated that 50% of lifelong handicapping conditions including blindness, deafness, developmental delay and cerebral palsy, with onset in infancy, is associated with extreme prematurity. Only 1% of births are extremely premature (<28 weeks), but these births account for approximately 25% of spending for perinatal care in Ohio. Unexplained variation in risk-adjusted prematurity rates in Ohio strongly suggests that opportunities for prevention exist. There is much to learn about the causes of preterm birth, yet there is substantial evidence to support a variety of interventions to reduce prematurity, including use of progesterone in women with a prior preterm birth, appropriate management of uterine malformations, management of inter-pregnancy interval for women with prior preterm birth, use of effective smoking cessation programs, and appropriate use of ovulation induction and assisted reproductive technologies. Quality improvement activities have been shown to be effective in increasing the use of evidencebased clinical practices (Horbar, 2000; Horbar, Carpenter, & Buzas, 2004; Horbar, Rogowski, & Plsek, 2001; Iams & Donovan, 2011; Kaplan, Lannon, Walsh, & Donovan, 2011) and improving clinical outcomes. These methods include the use of benchmarking, collaborative learning, using common metrics, and application of rigorous improvement methods such as the Associates for Page 2 of 19 Version 1 12/20/2013 Process Improvement “Model for Improvement” (Langley, Nolan, Nolan, Norman, & Provost, 1996). III: PURPOSE OF STUDY The purpose of OPQC is to improve perinatal newborn and infant outcomes in Ohio. OPQC will enhance existing quality improvement activities at participating practitioner sites by helping develop capacity to promote quality improvement, by helping develop and apply comparable quality measures, and by helping establish collaborative relationships and a broad-based coalition that will support these goals. IV. SIGNIFICANCE OF STUDY IN RELATION TO HUMAN HEALTH Quality Improvement projects led by OPQC can lead to a simultaneous decrease in rates of prematurity and infant mortality and neurodevelopmental, sensory and physical morbidity in Ohio over time, a decrease in the length of stay in the neonatal intensive care unit (NICU), and enhance the parents’ experience of their infant’s care and therefore decrease subsequent acute care health care use for surviving infants. In addition, lessons learned by OPQC and research focused on understanding the mechanisms of improvement and organizational behavior change in QI projects can help improve collaborative projects throughout the healthcare system V. PREVIOUS WORK DONE IN THIS AREA Over the last five years, OPQC has successfully implemented the following quality improvement projects, each of which followed a modified BTS methodology (as described in the Methods section): 1. Decreasing Late-Onset Infections in Infants born 22 – 29 weeks gestation This project aimed to decrease infections in neonates born at 22 to 29 weeks gestation, through three specific changes to practice – implementing an evidence-based catheter insertion bundle, implementing an evidence-based catheter maintenance bundle, and increasing the use of human milk as medicine in this population. A total of 24 teams/sites participated in this initiative. Our work and that of others suggests that reductions in infection are not seen consistently until reliability of processes is achieved and maintained. As maintenance bundle reliability increased Page 3 of 19 Version 1 12/20/2013 from <30% to 80% in the first phase of OPQC (2008-2010), we documented a 20% decrease in infections in this population from 18% to 14% (Kaplan, et al., 2011). We estimate that since OPQC work began in in 2008, 390 infections have been averted in these tiny babies, resulting in an approximate cost savings exceeding $6,500,000. Having attained consistent level 1 reliability of the catheter maintenance bundle, OPQC focused on attaining level 2 reliability (>95%) with monthly action calls, and active support to teams through December 2013. OPQC will then transition this project to a “sustain” mode. Research has shown that without ongoing monitoring and periodic refreshers teams lose their impact within 90- 120 days of the work. Thus it is important to continue monitoring and periodic check-ins. With a transition to sustain mode, infection data will continue to be monitored on a quarterly basis by OPQC leadership to ensure that improvements are sustained. 2. Decreasing Non-Medically Indicated Scheduled Births Prior to 39 Weeks Gestation Since 2008, OPQC has worked to reduce unnecessary scheduled births at 360/7 to 386/7 weeks gestational age in the obstetrical units of 20 of the largest hospitals in Ohio with the 20 chartermember OB teams. Following execution of an initial successful project in the 20 largest maternity hospitals in Ohio with sustained decreases observed, OPQC received additional funding from the Ohio Department of Health (ODH), Ohio Medicaid and the Center for Disease Control and Prevention (CDC) to 1) design a systematic implementation plan to engage all Ohio maternity hospitals in application of the successful scheduled delivery changes; 2) pilot this plan with a small number of maternity hospitals and 3) disseminate this work to remaining Ohio maternity hospitals. This project also involved the development of a plan to utilize the state regional BEACON (Best Evidence for Advancing Childhealth in Ohio Now) Quality Improvement Coordinators (QICs) in recruitment, outreach, and performance feedback efforts. In coordination with the Ohio Department of Health, and with the help of two BEACON QICs, OPQC recruited 15 hospitals in Ohio for a pilot dissemination project (January 2012 – December 2012). We developed and implemented a collaborative learning effort for these maternity hospitals, which included an initial Learning Session, data feedback using birth certificate data, and regular webinars. Selection criteria for the pilot sites ensured that this cohort included many of the hospitals with the highest number of Medicaid births, as indicated from birth certificate data, as well as geographic diversity. The pilot project concluded in December 2012. Page 4 of 19 Version 1 12/20/2013 Lessons learned from the pilot project were used to shape the recruitment strategy, dissemination plan, and project curriculum for a dissemination project. Recruitment strategy involved targeting the remaining non-OPQC maternity hospitals in the state of Ohio, which were been divided into three approximately equivalent cohorts; a letter was sent on behalf of OPQC leadership, ODHVital Statistics leadership, and the Ohio Hospital Association leadership to CEOs included in the first and second wave of dissemination hospitals, followed up with recruitment phone calls. The final wave of sites is on target to complete the improvement project by April 2014. Since the original “39-Weeks” project kick-off in 2008, over 36,200 births that would have been expected to occur prior to 39 weeks gestation have shifted to >39 weeks gestation. A total of 105 sites have participated in the quality improvement initiative. 3. Increasing the use of Antenatal Corticosteroids (ANCS) in women at risk for preterm birth. Maternal administration of antenatal corticosteroids (ANCS) to reduce the frequency and severity of complications of prematurity for infants born between 24 and 34 weeks of gestation has been recommended for almost 40 years yet gaps exist. This project focused reducing perinatal morbidity and mortality by ensuring >90% of infants born between 240/7th and 340/7th weeks of age receive ANCS. BTS methods were used to engage 19 OPQC maternity hospitals. VI: SELECTION OF PARTICIPANTS Patient Subject Selection Individual patients are not targeted or recruited to participate in OPQC efforts. Rather, populations of patients for whom evidence-informed care processes will improve care will benefit from OPQC improvement efforts. Participating sites will decide on aspects of care to improve. Populations of patients (pregnant women and infants) whose outcomes might benefit from that improved care will be targeted for care improvements. Practice sites will target groups of patients that meet improvement project eligibility criteria. As new improvement objectives are developed, different improvement projects will have different eligibility requirements. Because practice sites are working collaboratively, the same eligibility criteria will be used across sites for each improvement project. Page 5 of 19 Version 1 12/20/2013 Practice Site Selection All perinatal practice sites in Ohio may voluntarily choose to participate in OPQC improvement projects. Each site will be responsible for obtaining local IRB approval for participation or will agree to allow CCHMC to serve as the IRB of record; each site will sign data sharing agreements as appropriate. VII. RECRUITMENT Patient Subject Recruitment Individual patients are not targeted or recruited to participate in OPQC improvement efforts. All patients who meet pre-specified, project-specific criteria will be included in improvement projects. Because all OPQC improvement projects are evidence-informed and apply only interventions that have been endorsed by professional and governmental organization as the standard of care, none of the interventions are experimental. Individual patient-level consent will not be obtained. OPQC adds proven-effective quality improvement methods, rapid data analysis and collective experiential learning to accelerate quality improvement at participating sites. Practice Site Recruitment All perinatal practice sites in Ohio may voluntarily choose to participate in OPQC improvement projects. VIII. RANDOMIZATION Patients will not be randomized. IX. STUDY PROCEDURES OPQC will be directly engaged in facilitating the implementation of perinatal quality improvement activities at participating provider sites in Ohio. OPQC will support ongoing development of a multidisciplinary stakeholder group consisting of leaders from hospitals with neonatal care units in the state, key obstetrics leaders, and representatives from the Ohio Department of Health, the Ohio Chapters of the American Academy of Pediatrics (AAP) and American College of Obstetricians and Gynecologists (ACOG) and existing family support groups in each of the participating NICUs. The OPQC Steering Committee with representatives from perinatal caregivers from across the state will review and endorse recommendations and Page 6 of 19 Version 1 12/20/2013 measures for improving care at the participating sites. Participating providers will report on their performance monthly throughout the project period. Improvement teams from participating provider groups, together with clinical experts, quality improvement experts and peers at other provider sites will exchange data about results. An organizational team at each site will plan specific changes they will make at the local level. Lessons learned among the various participating provider sites will be shared using the OPQC communication infrastructure (e.g. face-to-face meetings twice/year, monthly webinars, listserv). OPQC technical staff will provide regular coaching on data collection and reporting, improvement methods and spread strategies by teleconference on a monthly basis. A full time OPQC Project Manager will be responsible for managing timelines for improvement at each site. With the leadership of the OPQC Steering Committee, the data management team funded by the state and based at CCHMC will collate monthly reports from each provider site. OPQC sites will participate in statewide improvement collaborative meetings each year. OPQC will produce and distribute monthly reports from participating provider sites that include aim statements, key driver analyses and annotated run charts. Selected improvement projects will be implemented by provider sites that agree to participate. For example, sites may decide to improve the delivery of pulmonary surfactant to eligible infants. Participating sites will submit both individual patient process and outcome data that are relevant to the project to OPQC via a secure, password-protected web site. Consistent with the HIPAAspecified Limited Data Set, the only protected health information (PHI) that will be collected and retained at the Anderson Center will be dates of service. Patient-level data will be aggregated to provide site-specific progress reports back to the site where the improvement project is being conducted. Unless there is specific written agreement from the site, reports that are shared with other participating sites will not identify the site from which the data derive. Team Composition A multidisciplinary team will be formed at each participating clinical site. Each team will consist of a physician, possibly with the involvement of additional physicians, as well as ancillary support staff. Specific team members will vary depending on the site, and may include an advanced practice nurse, clinic nurse, birth registrar, nutritionist, or administrative staff. This team will 1) collect and transmit clinical data and information about care processes, and 2) Page 7 of 19 Version 1 12/20/2013 participate in an improvement collaborative to test how to best implement identified standards of care. Progress towards OPQC goals will be measured by collecting data from each practice site. Data will be collected as an integral part of the routine patient care. The OPQC improvement community Teams will participate in an improvement collaborative that will include face-to-face learning sessions and webinars that includes training in quality improvement methods, review of identified “best practice” clinical process standards for prenatal and neonatal care, and assistance to teams in planning how to implement the strategies. Teams will share what they have learned and analyze their progress, with input from colleagues and guidance from the project team. Collaborative teams will confer on a regular basis during active projects. Measurement of performance is a key step in making improvements. Measurement defines gaps to be overcome and permits assessment of whether changes are making a difference. Collaborative teams will be asked to review data on their own performance regarding care processes; discussion of data will compare practice performance with established goals and identify problems or barriers that may impede improved performance and the potential benefits of a systems approach to providing care. Teams will be asked to submit a report each month outlining changes, barriers encountered and date on performance measures. In addition, team performance will be tracked monthly and each team’s progress assessed to better target ongoing improvement activities. Interaction will be managed through an extranet web-site devoted specifically to this project. Support will be provided on an ongoing basis to practice sites as they work to understand current clinical routines and learn about barriers to improvement, and then test and implement new approaches to care. Consultation, monitoring and feedback will be provided by OPQC project staff and faculty. Information gathered from each site by progress reports will be used to assess the status of each site and to guide the assistance that takes place during conference calls and learning sessions. X: VULNERABLE POPULATIONS Patient Subjects All patients who meet clinical condition eligibility criteria will have equal probability of participating. No patients will be excluded based on vulnerability characteristics. Because this is Page 8 of 19 Version 1 12/20/2013 a population-based project, we expect that all population subgroups at each site will be proportionately represented. XI: SURVEYS OR QUESTIONNAIRES Not applicable. XII: BLOOD Not applicable. XIII: METHODS OPQC employs improvement science methods that have been developed and endorsed by the Institute for Healthcare Improvement (IHI) on all of the above referenced projects. These methods are based on the work of leaders in the field of quality improvement, most notably W. Edwards Deming, as well as the Associates in Process Improvement (API) (who serve as senior fellows of the IHI). These methods include The Model for Improvement, the Breakthrough Series Model (BTS), and the use of statistical process control methods. Two of the leading texts for implementing quality improvement methods in practice were authored by the API: The Improvement Guide and Quality Improvement through Planned Experimentation; in addition, the API/IHI have written IHI White Papers on the Breakthrough Series Method and Spread which provide models for the work of OPQC. In addition, Lloyd Provost, MS, partner in API, senior fellow IHI, winner of the American Society for Quality’s Deming Medal in 2003, serves as consultant for OPQC. OPQC uses an adapted Breakthrough Series Model (BTS) for engaging and working with teams. This method is based on improvement science as well as continuing education principles and adult learning. It was designed to overcome barriers and to accelerate translation of evidence into practice by engaging multiple teams to learn from each other and from recognized experts to make improvements in a specific topic area. Figure 1 outlines the structure of the BTS model. Page 9 of 19 Version 1 12/20/2013 Figure 1: The Institute for Healthcare Improvement Breakthrough Series Model The Learning Model - BTS Collaborative Expert Planning Group Meeting Participants P Prework Change Concepts Refine Collaborative Design P D A S S Action Period 2 LS2 D A S Action Period 1 LS 1 P D A Action Period 3 LS 3 Closeout Supports Visits E-mail Documents Phone Assessments Institute for Healthcare Improvement Specifically, the BTS model promotes use of the Model for Improvement, including rapid PlanDo-Study-Act (PDSA) cycles, in which teams are taught to address problems as they arise by testing interventions and subsequent modifications in small steps to achieve desired change. OPQC brings teams together in face-to-face sessions (Learning Sessions) at regular intervals to review individual and aggregate data, learn from teams that have been successful at making changes and achieving improved outcomes, and with expert guidance, apply the IHI Model-forImprovement to test specific strategies. We then support teams with (1) monthly webinars to review and interpret hospital-specific and aggregate control charts, (2) testing of strategies to improve care at the physician, hospital and patient level and (3) individual and group coaching. Each project undertaken by OPQC is guided by a Change Framework. The Change Framework is a set of materials and ideas that direct and enable Collaborative teams to implement breakthrough change in their setting. It has three main elements: 1) the project’s specific aim, 2) a conceptual framework or Key Driver Diagram (KDD) and 3) a set of measures that enable teams to track progress to Collaborative aims. A KDD describes features of the ideal system for the topic and a set of changes or strategies that have proven effective in achieving improvements. Outcome measures will change over time based on areas of focus of a given project Page 10 of 19 Version 1 12/20/2013 Sites will submit project-relevant data that is collected during each patient visit or hospitalization to the OPQC’s data submission web site, a secure, password-protected system. Participating sites will enter patient data into the OPQC website. OPQC will use these data to perform analyses and create reports that will be provided to each center on a regular basis. To optimize the collection, transmission and analysis of data, we will use internet-enabled data collection and reporting tools. Data will be evaluated on receipt to ensure that it is valid prior to incorporation into the aggregate study database. Available tools allow rapid feedback of performance data, preparation of progress reports over the internet and communication among teams. Charts of key clinical care process and outcome measures will be provided to each site on a monthly basis, and will allow each site to benchmark its program against the aggregate collaborative data. Data elements included in the OPQC database will be selected to support specific improvement projects. Multiple improvement projects will be conducted simultaneously and sequentially over time. Although the data elements used to support individual quality improvement projects will vary over time and different improvement projects will use different data elements, the data will be de-identified using the HIPAA-specified “limited data set” rules. Thus the following data elements will be excluded from the study database: names, postal address information, other than town or city, state, and ZIP Code, license plate numbers, telephone numbers, fax numbers, electronic mail addresses, social security numbers, medical record numbers, voiceprints, health plan beneficiary numbers, account numbers, certificate/license numbers, vehicle identifiers and serial numbers, device identifiers and serial numbers, web universal resource locators (URLs), internet protocol (IP) address numbers, biometric identifiers, including fingerprints and full-face photographic images and any comparable images. All OPQC improvement projects will include “balancing measures” which assess whether improvements to one part of the system cause unintended consequences in other parts of the health system. For example, despite evidence to the contrary, neonatologists have traditionally been very cautious about beginning feedings in the first days of life for infants born 22 – 29 weeks gestation for fear of precipitating a catastrophic bowel illness called necrotizing enterocolitis (NEC). NEC causes death in half of those who contract it and severe and prolonged illness in survivors. Therefore in our recent “Decreasing Late Onset Infections Project” we tracked the incidence of necrotizing enterocolitis as a balancing measure to ensure that no harm had been triggered by the earlier and more aggressive feeding practices implemented to decrease infection rates. OPQC demonstrated that rates of NEC actually decreased. Page 11 of 19 Version 1 12/20/2013 To assess the impact of OPQC on the increased use of best care practices, we will need to account for what sites are already doing. Therefore, we will collect data from each center to determine the degree to which sites are already using any of the care processes and strategies to be evaluated in this project. We will collect information about diagnosis and patient factors that may influence the success of sites’ efforts or confound our ability to measure it. Two projects planned for 2014 include a new Progesterone Project and a new Neonatal Abstinence Syndrome (NAS) Project. These quality improvement projects will follow the methods and processes as described above. Progesterone Project Women who have a prior spontaneous preterm birth and/or who have a short cervix face increased odds of preterm birth (PTB). Progesterone is known to reduce PTB significantly in women with these risk factors, and, as is customary for OPQC projects, has been endorsed by authoritative organizations as “standard practice” (in this case, the American College of Obstetricians and Gynecologists and the Society for Maternal Fetal Medicine). The aim of the project will be to reduce preterm birth in Ohio <37 weeks from 10.6% to 9.75% and births <32weeks from 2.1% to 1.9% through increasing the number high-risk Medicaid women receiving Progesterone therapy (including injectable 17-alpha-hydroxyprogesterone and vaginal progesterone). This will be accomplished by designing and implementing a quality improvement (QI) collaborative, working with insurers and policy makers to remove administrative barriers to timely receipt of Progesterone therapy for at risk women, and partnering with patients and families to ensure that messaging and interventions implemented at the local level are appropriate for the target population. The Progesterone Project will initially involve the 20 charter member OB sites that have worked with OPQC since 2008, and will also involve 20 – 40 outpatient clinics that are affiliated with those sites, with staged dissemination to all OPQC maternity participants over the next 2 years as requested by the Ohio Departments of Health and Medicaid, sponsors of this project. Neonatal Abstinence Syndrome (NAS) Project Neonatal Abstinence Syndrome (NAS) is a significant and increasing public health issue, with estimates that one infant is born addicted to narcotics every hour in the United States. Tiny newborns with NAS suffer withdrawal only hours after entering the world-- nausea, vomiting, Page 12 of 19 Version 1 12/20/2013 and tremors. These early signs may be unrecognized as NAS prior to discharge. If unidentified and untreated infants can develop excessive weight loss, grand mal seizures and may die. By increasing identification of and compassionate withdrawal treatment for full-term infants born with Neonatal Abstinence Syndrome (NAS), we will improve health outcomes and reduce length of stay by 20% across participating sites by June 30, 2015. We will disseminate an evidence-based protocol for treatment of infants with NAS to all Level 2 and Level 3 NICUs in Ohio using a modified Break Through Series model (as described above) and we will increase the identification of mothers and newborns exposed to narcotics at Level 1 hospitals. In addition, we will utilize a primary prevention campaign strategy with the goals of 1) focused public health messaging to physicians, emergency rooms and dentists on the hazards of prescribing narcotics during pregnancy, and 2) focused messaging to non-pregnant women in Medication assisted treatment settings on the wisdom of preventing pregnancy during the recovery process. Funding for this work is provided by the Ohio Department of Health, the Ohio Department of Medicaid, and the Ohio Government Resource Center (see funding proposal for additional detail). XIV: POTENTIAL BENEFITS Attempts to implement new approaches will lead to new knowledge and innovations in the care delivery process. A final component of the project will be to document and spread lessons and principles of better care through the OPQC network. We will refine a set of tools for use by subsequent collaborative improvement efforts, enabling the dissemination of this model to other centers and other health conditions and populations. This project will build capacity to accelerate the uptake of evidence-based findings and tools for care of children and make continuous improvement a key part of the fabric of participating practice sites XV: POTENTIAL RISKS, DISCOMFORTS, INCONVENIENCES, AND PRECAUTIONS Improving the processes of care is an integral part of every day practice. Often these changes in care practice are made informally using trial and error methods on small numbers of patients. The Ohio Perinatal Quality Collaborative improvement projects use formal methods such as clearly pre-specifying the intervention, measuring both characteristics of the intervention and outcomes and reporting results transparently to ascertain the effect of change on the outcome of interest. There are no known additional risks or discomforts resulting from participation in this process. Page 13 of 19 Version 1 12/20/2013 During practice site conference calls, members of the collaborative may discuss areas of their practices that require improvement, potentially introducing some anxiety. However, since we are not reporting on individual provider data, but rather practice level data (aggregate), we expect the risk to the individual to be minimal. In our experience, clinicians are most often reassured to find that colleagues share the same barriers and challenges to care and to have expert and colleague support in implementing improvements. XVI: RISK/BENEFIT ANALYSIS Recommendation for how the study should be classified is minimal risk with the potential for direct benefit to the subjects. XVII: WITHDRAWALS Not applicable. XVIII: DATA SAFETY & MONITORING This quality improvement project includes review of patient’s medical records. There are no known risks or discomforts resulting from participation in this study. The project team will review unanticipated problems during our monthly conference call. XIX: PRIVACY All practice sites participating in the OPQC will obtain IRB approval for participation. All data to be transmitted outside the practice sites will be consistent with a Limited Data Set. XX: CONFIDENTIALITY The OPQC is a statewide organization. All participating sites will provide limited patient-level data sets to OPQC on a monthly basis using a secure, encrypted, web-based interface. The only HIPAA identifier that will be collected will be dates and this would be consistent with a Limited Data Set. The OPQC office is at the Anderson Center at Cincinnati Children’s Hospital Medical Center. Data without patient identifiers will be stored by OPQC in a secure, passwordprotected, electronic database. The results of this study may eventually be published and Page 14 of 19 Version 1 12/20/2013 information may be exchanged between medical investigators, but patient confidentiality will be maintained. XXI: PAYMENT FOR STUDIES Patients and families will not be financially compensated. XXII: PROCESS OF OBTAINING INFORMED CONSENT Practice sites will not seek written informed consent of their patients because this work simply refines existing efforts to improve care. XXIII: ASSENT & PARENTAL PERMISSION Practice sites will be responsible for informing all patients of ongoing, systematic efforts to improve care. XXIV: WAIVER OF CONSENT Waiver of informed consent is requested. This is a data collection project with practice improvement measures being part of the database. It does not involve direct contact with patients or families. It is important to emphasize that a project such as this, which strives to assess the clinical care processes and outcomes at a program level, would be impossible to accomplish if individual consent were required from every patient. In addition, participation in the research is minimal risk. The data set transmitted to the OPQC database would constitute individually identifiable data according to 45CFR46, however the only identifiers will be gestational age at birth and month and year of service, and therefore this date set would be consistent with minimal risk. Given the nature of this project it is not practical for the clinical staff to obtain consent for the registry in the course of their regular work. Those actively implementing the individual QI projects (clinical staff) in the hospital will likely not be associated with this QI research registry and obtaining informed consent would likely impact the conduct/validity of the individual QI projects. This waiver of consent is not likely to affect participant/parent rights. In the event it is determined relevant, additional information would be provided to the patients at the direction of the IRB. Page 15 of 19 Version 1 12/20/2013 Appendix HIPAA-specified Limited Data Set Protecting Personal Health Information in Research: Understanding the HIPAA Privacy Rule NIH Publication Number 03-5388 DEPARTMENT OF HE ALTH & HUMAN SERVICES USA Limited Data Set – Refers to PHI that excludes 16 categories of direct identifiers and may be used or disclosed, for purposes of research, public health, or health care operations, without obtaining either an individual’s Authorization or a waiver or an alteration of Authorization for its use and disclosure, with a data use agreement. Data Use Agreement – An agreement into which the covered entity enters with the intended recipient of a limited data set that establishes the ways in which the information in the limited data set may be used and how it will be protected. The Privacy Rule permits a covered entity, without obtaining an Authorization or documentation of a waiver or an alteration of Authorization, to use and disclose PHI included in a limited data set. A covered entity may use and disclose a limited data set for research activities conducted by itself, another covered entity, or a researcher who is not a covered entity if the disclosing covered entity and the limited data set recipient enter into a data use agreement. Limited data sets may be used or disclosed only for purposes of research, public health, or health care operations. Because limited data sets may contain identifiable information, they are still PHI. A limited data set is described as health information that excludes certain, listed direct identifiers (see below) but that may include city; state; ZIP Code; elements of date; and other numbers, characteristics, or codes not listed as direct identifiers. The direct identifiers listed in the Privacy Rule’s limited data set provisions apply both to information about the individual and to information about the individual’s relatives, employers, or household members. The following identifiers must be removed from health information if the data are to qualify as a limited data set: 1. Names. 2. Postal address information, other than town or city, state, ZIP Code, and license plate numbers. Page 16 of 19 Version 1 12/20/2013 3. Telephone numbers. 4. Fax numbers. 5. Electronic mail addresses. 6. Social security numbers. 7. Medical record numbers. and voiceprints. 8. Health plan beneficiary numbers. 9. Account numbers. 10. Certificate/license numbers. 11. Vehicle identifiers and serial numbers, 12. Device identifiers and serial numbers. 13. Web universal resource locators (URLs). 14. Internet protocol (IP) address numbers. 15. Biometric identifiers, including fingerprints 16. Full-face photographic images and any comparable images. A data use agreement is the means by which covered entities obtain satisfactory assurances that the recipient of the limited data set will use or disclose the PHI in the data set only for specified purposes. Even if the person requesting a limited data set from a covered entity is an employee or otherwise a member of the covered entity’s workforce, a written data use agreement meeting the Privacy Rule’s requirements must be in place between the covered entity and the limited data set recipient. The Privacy Rule requires a data use agreement to contain the following provisions: • Specific permitted uses and disclosures of the limited data set by the recipient consistent with the purpose for which it was disclosed (a data use agreement cannot authorize the recipient to use or further disclose the information in a way that, if done by the covered entity, would violate the Privacy Rule). • Identify who is permitted to use or receive the limited data set. • Stipulations that the recipient will Not use or disclose the information other than permitted by the agreement or otherwise required by law. Use appropriate safeguards to prevent the use or disclosure of the information, except as provided. Page 17 of 19 Version 1 12/20/2013 For in the agreement, and require the recipient to report to the covered entity any uses or Disclosures in violation of the agreement of which the recipient becomes aware. Hold any agent of the recipient (including subcontractors) to the standards, restrictions, and conditions stated in the data use agreement with respect to the information. Not identify the information or contact the individuals. If a covered entity is the recipient of a limited data set and violates the data use agreement, it is deemed to have violated the Privacy Rule. If the covered entity providing the limited data set knows of a pattern of activity or practice by the recipient that constitutes a material breach or violation of the data use agreement, the covered entity must take reasonable steps to correct the inappropriate activity or practice. If the steps are not successful, the covered entity must discontinue disclosure of PHI to the recipient and notify HHS. Section 164.512 of the Privacy Rule also establishes specific PHI uses and disclosures that a covered entity is permitted to make for research without an Authorization, a waiver or an alteration of Authorization, or a data use agreement. These limited activities are the use or disclosure of PHI preparatory to research and the use or disclosure of PHI pertaining to decedents for research. Page 18 of 19 Version 1 12/20/2013 References Horbar J, Carpenter J, Buzas J, al e. Collaborative quality improvement to promote evidence based surfactant for premature infants; a cluster randomized trial. British Medical Journal. 2004;329:1004-10. Horbar J, NIC/Q 2000: Establishing habits for improvement in neonatal intensive care units P-, 2003. NIC/Q 2000: Establishing habits for improvement in neonatal intensive care units. Pediatrics. 2003;111:397-410. Horbar J, Rogowski J, Plsek P. Collaborative quality improvement for neonatal intensive care. Pediatrics. 2001;107:14-22. Iams JD, Donovan EF. Spontaneous Late-Preterm Births: What Can Be Done to Improve Outcomes? Semin Perinatol. 2011 Oct;35(5):309-13. Kaplan HC, Lannon C, Walsh MC, Donovan EF; Ohio Perinatal Quality Collaborative. Ohio statewide quality-improvement collaborative to reduce late-onset sepsis in preterm infants. Pediatrics. 2011 Mar;127(3):427-35. Epub 2011 Feb 21. Langley G, Nolan K, Nolan T, Norman C, Provost L. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. San Francisco; 1996. Page 19 of 19 Version 1