Methods Study site We studied canine cutaneous leishmaniasis
advertisement

Methods
Study site
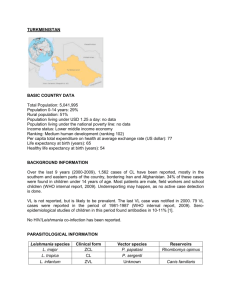
We studied canine cutaneous leishmaniasis exposure in dogs from 24 households at
Trinidad de Las Minas (8°46´32´´N; 79°59´45´´W), western Panama province, Republic of
Panama (Figure 1). In this area climate is unimodal, with rainy (April to November) and dry
(December to March) seasons, and rain ranging from 28 to 570 mm3 per month. Temperature is
nearly constant with a year-round 26°C average. We only surveyed the dog population from 24
households (out of 198 in the village) because our resources were constrained, especially the
number of light traps available for SF sampling. Nevertheless, all houses enrolled in the study
had confirmed SF presence (by the residents), had similar eco-epidemiological conditions and
householders provided written informed consent to participate in the study. We also want to
notice that assuming two dogs per house [1,2], i.e., an approximate dog population size of 396
dogs in the whole village, a sample size of 48 dogs is large enough to detect a seroprevalence of
at least 20% with a 10% precision, i.e., with 95% confidence intervals that spans from 10-30%
[3], prevalence values that have been previously recorded in Panama [1,2] and elsewhere
canine cutaneous leishmaniasis is endemic in the New World
[4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23].
Ethical approval
This study was evaluated and approved by the National Review Board, Comité Nacional
de Bioética de la Investigación, Instituto Conmemorativo Gorgas de Estudios de la Salud,
Panama City, Republic of Panama (561 /CNBI/ICGES/06).
Data Collection
Dog sampling how were the ectoparasites, lesson, physical condition data collected?
PCR, ELISA and IFAT procedures
Entomological, Epidemiological and Ecological variables at the household level
A series of variables, potentially associated with canine cutaneous leishmaniasis pathogen
exposure, were quantified for each one of the households (or their peridomiciliary environments)
enrolled in our study. In the next lines we briefly describe the entomological, epidemiological and
ecological variables that we measured during our study.
Entomological variables. SF were sampled once per month (April - June 2010) using modified HP light
traps [24] with an additional LED light [25]. Two traps were set from 6 pm to 6 am, at 2 m height in each
household, and at the same site during the three sampling periods. One trap was placed inside the main
room of the household (domicile) and the other trap over vegetation within a 50 m radius from the
house (peridomicile). SF were removed from the traps and stored at -20 °C to kill the sampless, which
were subsequently preserved in 70 % alcohol, separated by sex and identified to the species level based
on the male genitalia and female spermathecae following the taxonomic key of Young and Duncan [26].
For the analysis, we employed the average from the three monthly observations. A detailed inventory of
the collected sand flies and their diversity patterns is presented by Calzada et al [25].
Epidemiological variables. We recorded the number of humans, the number of humans with active and
parasitologically confirmed leishmaniasis lessons, the number of humans with past leishmaniasis lessons
in each household. A full and detailed description of epidemiological data collection and patterns of
clinical cutaneous leishmaniasis in humans is presented by Saldaña et al [27].
Ecological variables. For a each household we estimated: a housing destituteness index, which
quantified how different elements of housing construction and materials render houses differentially
suitable habitats for SF; a peridomicile index, that quantified the abundance and availability of adult SF
resting sites in a peridomicile; a vegetation index, that measured natural vegetation vertical structure;
the richness, i.e., number of species, of domestic and wildlife animals; an index of domestic animal
abundance, which weighted the abundance of different domestic species belonging to a household; and
an index of wild animal presence, which weighted the commonness of different wildlife species sighted
by householders. A detailed description of data collection, and the estimation of each index, is
presented by Chaves et al[28].
Statistical Analysis
ELISA seropositive assignation from the optical densities
We assigned as seropositive all dogs whose averaged optical density from the ELISA was above
the mean plus three standard deviations [29] of the distribution with the smallest mean (i.e., that of the
likely seronegative individuals) in a normal finite mixture model [for details see supplement S1]. This
method was chosen because of its robustness to small changes in antibody titres that can emerge from
seasonality and/or small variations in laboratory assay performance [30], problems already identified for
canine leishmaniasis serodiagnosis [31]. Parameters for the finite mixture model were estimated with
the command normalmixEM() of the library mixtools in the statistical package R version 2.15.3. For the
distribution with the smallest mean we estimated a mean (± S.E.) of 0.102 ± 0.038, which leads to a
seropositivity threshold of 0.216, i.e., any dog whose ELISA optical density was above this value could be
considered positive, Figure S1 shows the distribution of the optical densities from the ELISA test.
Sensitivity and specificity for the IFAT and ELISA as diagnostics of canine cutaneous leishmaniasis
caused by Leishmania (Viannia) panamensis
Sensitivity, the ability of a test to diagnose a true infection, and specificity, the ability of a test to avoid
false negative diagnostics (i.e., to not miss true positive infections), is generally assessed in the presence
of a “gold standard”, for example, the direct observation of a parasite or its DNA amplification via PCR
[32]. Nevertheless, canine cutaneous leishmaniasis is a system where a “gold standard” is likely not
plausible, given the limited tissues were positive PCRs could be expected, mainly cutaneous lessons [ref].
In fact, we tested parasite presence in blood samples using a PCR based on [brief Details about the pcr]
where all results were negative, probably because of the localized presence of parasites around sand fly
vector bites and/or cutaneous lessons [ref]. Therefore, we employed the method developed by
Dendukuri and Joseph [33] to estimate the sensitivity and specificity of two diagnostic tests in one
population, which employs a Bayesian framework for parameter inference, for details see Supplement
S2. For the analysis we assumed the following priors: uniform distributions for the covariance of positive
and negative tests, an uninformative beta distribution for the real prevalence in the population, beta
distributions with mode=0.90 and 5th percentile=0.70 for the specificity and sensitivity of the ELISA, a
beta distribution with mode=0.70 and 5th percentile=0.50 for the IFAT sensitivity, and a beta
distribution with mode=0.80 and 5th percentile=0.60 for the IFAT specificity. These distributions were
based on reported sensitivities for ELISA tests for canine cutaneous Leishmaniasis [ref] and on the
observation that ELISA tests tend to outperform IFAT tests [refs]. Posterior inferences were based on
100000 realizations that followed 10000 burned-in realizations for the Markov Chain Monte Carlo
(MCMC) stabilization. MCMC convergence was assessed by running multiple chains with dispersed
starting values. Following the recommendations of Branscum et al [32], we also performed a parameter
sensitivity analysis, described in the Supplement S2. The analyses described in this section were
implemented in the BUGS statistical software modifying the code presented by Branscum et al [32]
Risk factors associated with cutaneous leishmaniasis seropositivity in dogs
To estimate the impact of different risk factors on dog seropositivity patterns we investigated
the role of several entomological, ecological and epidemiological variables that were common to dogs
belonging to a given household. We also investigated the joint effect of these household-level covariates
with individually collected information from each dog health condition.
For the household analysis we employed maximum likelihood Binomial Generalized Linear
Models (Bin-GLMs) [34]. We first identified the best entomological covariate via an Akaike Information
Criterion (AIC) comparison [35] of models [or their simplifications] that considered one of the following
entomological variables: (i) total abundance of sand flies collected; (ii) abundance of domiciliary and
peridomiciliary sand flies; (iii) total abundance of Lutzomyia trapidoi and Lu. panamensis, the main
dominant vector species in the study area [25] and the whole republic Panama [36,37,38]; (iv)
abundance of domiciliary and peridomiciliary Lu. trapidoi and Lu. panamensis. We needed to perform
this preliminary selection of entomological variables given their lack of independence, i.e., some
variables are an additive function of the other variables, a fact that can lead to parameter estimation
identifiability [35]. We performed model selection via AIC, i.e., considered both model likelihood and
parameter number, because models were not always nested (i.e., with simpler models having a subset
of variables from a more complex model), therefore not comparable via likelihood ratio tests [39].
Following the selection of the best entomological covariate, we proceeded to incorporate all
epidemiological and ecological household level variables already described in the Entomological,
Epidemiological and Ecological variables at the household level section. We then selected the best
model following a procedure of backward elimination from a full model, which considered the best
entomological covariate plus all the ecological and epidemiological variables. All variables whose single
elimination decreased the simpler model AIC in relation to a model incorporating such covariates were
discarded at once [39]. Nevertheless, at the final stage of model selection we compared nested models
with non-significant factors, employing likelihood ratio tests if the AIC was not minimized by the most
simple model [39]. Given the spatial nature of the households, we performed a Moran I index test on
the residuals from the model selected as best, in order to ensure the spatial independence of the
residuals, an assumption for the proper use of Bin-GLMs [39].
For the individual based risk factor assessment we employed Logistic Generalized Estimating
Equations Models (Log-GEEM) [34,39]. We employed Log-GEEM given the nature of the data, where
dogs belonging to a same household are not independent observations, a fact constraining the use of
simpler regression tools [40]. We assumed independence in the correlation structure of the models,
provided the ability of GEE to obtain consistent estimates for the fixed effects even when the correlation
structure is incorrect [39]. For the inference we used a sandwich estimator to obtain robust standard
errors, provided that naïve standard errors are appropriate only when the correlation structure is
correct [34]. For the identification of significant risk factors for canine cutaneous leishmaniasis, we
began our analysis by building a full model that included the best entomological covariate selected for
the Bin-GLMs, all the epidemiological and ecological variables collected at the household level and
information on each dog health condition (physical condition, cutaneous lessons, de-worming and
ectoparasite presence), whether the dog sleeped inside the house and demography (i.e., sex and age).
This model was simplified using a procedure similar to the one employed for the Bin-GLMs, but
exclusively based on the quasilikelihood information criterion (QIC) [41], the GEE analog to AIC.
For the models we employed seropositivity results based on ELISA and the seropositivity by at
least one test (i.e., ELISA and/or IFAT) when fitting both the Bin-GLMs and Log-GEEMs. We did not
perform this analysis on the IFAT results given the low sensitivity of this technique (see Results section).
Bin-GLMs and Log-GEEMs were fitted with the statistical package R version 2.15.3.
Force of infection (λ) and basic reproductive number (R0) estimation
We estimated the force of infection (λ) assuming that seroconversion dynamics in susceptible
dogs followed an irreversible autocatalytic process [42,43], which can be described by the following nonlinear partial differential equation:
S (a, t ) S (a, t )
λ1 S (a, t )
t
a
(1)
where S is the fraction of susceptible dogs in a dog population that is composed by susceptible and
seropositive dogs. At any given time, denoted by t, equation (1) can be integrated as function of the age,
denoted by a, and assuming all dogs are born susceptible to become seropositive following the exposure
to canine cutaneous leishmaniasis pathogens, we can obtain the following function for the proportion of
seropositive dogs (S) as function of age (a):
S 1 e (a)
(2)
We thus employed our data on seroprevalence (S) and age (a) to estimate (λ) with equation (2). We
specifically employed maximum likelihood methods for the estimation [44], where we assumed that
seroprevalence was normally distributed, with a mean defined by equation (2) and a variance for the
deviations (error) from that mean. Supplement S3 has the R code we employed for the maximum
likelihood parameter estimation.
To estimate the basic reproduction number, R0, we first built a vertical [45] survival schedule, i.e.,
a survivorship curve based on the dog population age structure, in order to obtain estimate dog’s life
expectancy, i.e., the average lifespan [46] of dogs, at Trinidad de Las Minas. Briefly, a vertical survival
schedule assumes the age structure of a population to represent the survival schedule of a population at
equilibrium and with a pyramidal age structure, i.e., with a larger proportion of younger than older
individuals [45,47]. Because the dog population at Trinidad de Las Minas has a pyramidal structure, and,
on average, each household in rural Panama has a couple of dogs [2] it can be argued that dogs are a
stationary population fulfilling the assumptions for the sound estimation of a survival schedule, denoted
by l(a), based on the ratios of consecutive age clases:
l (a 1)
N (a 1)
N (a)
(3)
In (3) l(a+1) is defined as the probability of surviving from age a to a+1 [46]. Since individuals at
older ages, i.e., 8 or more years, were few, and their abundance did not monotonically decrease, we
followed the standard recommendation of smoothing the l(a) curve [47]. For the smoothing we
employed the lowess algorithm [39]:
~
l (a ) lowess l (a )
(4)
With the smoothed survival schedule we calculated dog’s life expectancy with the following equation
[45,47]:
~
e0 l (a)
(5)
0
And with e0, the force of infection (λ) and the smoothed survival schedule we estimated R0 as follows:
R0
e
e0
a
~
l (a)
(6)
0
Where (6) makes no specific assumptions about the mortality patterns in the dog population. A detailed
derivation of equation (6) and its comparison with expressions that made strong assumptions about
population mortality are presented in the Supplement S4.
Figure 1 Study Site. The upper part of the plot shows the location of Trinidad de Las Minas in El Cacao
county and Capira district and their location in Panama. The lower part shows the specific location of all
the houses where the dogs were censused. In the y and x axis 0.001 degree of latitude/longitude are
approximately 110 m.
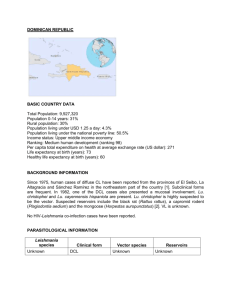
Figure 2 Seroprevalence and Dominant vector species abundance. In all panels symbol size is
proportional to abundance. (A) ELISA, circles are proportional to the number of dog (Dogs) and grey dots
to the number of ELISA seropositive dogs (ELISA +), symbol size in the inset legend corresponds to two
individuals. (B) Indirect Immuno Fluorescence, IFAT, circles are proportional to the number of dogs
(Dogs) and grey dots to the number of IFAT seropositive dogs (IFAT +), symbol size in the inset legend
corresponds to two individuals. (C) Lutzomyia trapidoi abundance, for symbol interpretation please
refer to the inset legend, where symbol size corresponds to two individuals. (D) L panamensis
abundance, for symbol interpretation please refer to the inset legend, where symbol size corresponds to
four individuals in the domiciliary environment and 20 individuals in the peridomiciliary environment.
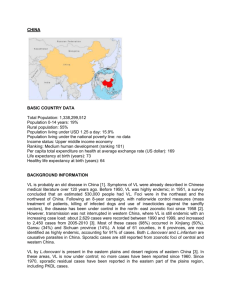
Figure 3 Force of Infection (λ) and basic reproduction number (R0) estimation (A) Age specific survival
(l(a)) schedule from a vertical life table (open circles). The solid line represents a lowess smoothed
survival schedule. Life expectancy (e0) was estimated with the lowess smoothed survival l(a) curve and
equation (5) (B) Age specific seroprevalence from ELISA (C) Age specific seroprevalence from IFAT, (D)
Age specific seroprevalence from based on seropositive counts from either the ELISA or IFAT. In B, C and
D λ was estimated via the maximum likelihood fitting of equation (2) to the seroprevalence data (open
circles). In C data from the observations depicted by black circles were not consider for parameter
estimation given their outlier behavior. For a full description of the maximum likelihood procedure
please refer to Supplement 3. R0 was estimated with equation (6).
Table 1 Demography, health condition and cutaneous leishmaniasis seropositivity in a dog populat ion in
Trinidad de Las Minas, Panama
Age years
Below
1
1-2
3-4
5 or
more
Total
(Females)
Poor
physical
condition
Ectoparasite
Presence
Deworming
Sleeping
inside the
house
Cutaneous
Lessons
ELISA+
IFAT+
%Seroprevalence*
12 (5)
8
12
6
1
0
4
1
33 (4)
16 (6)
12 (2)
6
4
15
10
5
7
1
1
7
4
6
7
2
4
38 (6)
67 (8)
11(4)
4
11
7
1
4
7
7
73 (8)
*The value inside parenthesis indicates the number of seropositives obatained by at least one method
Table 2 Sensitivity and specificity estimates for canine cutaneous leishmaniasis ELISA and IFAT diagnostic
tests. 95 % CI indicate the 95% Bayesian credible intervals.
Diagnostic Test Parameter
Sensitivity
ELISA
Specificity
Sensitivity
IFAT
Specificity
Mean
0.79
0.84
0.51
0.77
95% CI
0.67 0.90
0.62 0.97
0.38 0.63
0.48 0.95
Table 3 Parameter estimates for the best binomial generalized linear models explaining the odds ratio of
cutaneous leishmaniasis seropositivity in dogs at the household level. 95 % CI indicate the 95 %
maximum likelihood confidence intervals for the estimated odds.
Test
Parameter
Intercept
Lutzomia trapidoi abundance inside the
houses
Moran’s I test for spatial autocorrelation
in the residuals
Intercept
Lutzomia trapidoi abundance inside the
ELISA
houses
Moran’s I test for spatial autocorrelation
in the residuals
*statistically significant (P<0.05)
ANY
(ELISA or
IFAT)
Odds Ratio (95%
CI)
1
Estimate (±
S.E.)
---
---
2.98 (1.17-9.46)
1.09 (± 0.52)
0.036*
----
0.0041
0.363
1
---
---
2.28 (1.07 – 7.13)
0.948 (± 0.473)
0.033*
---
-0.085
0.568
P
Table 4 Parameter estimates for the best logistic generalized estimating equation models explaining
cutaneous leishmaniasis seropositivity in dogs. For the analysis houses were considered as the clustering
factor.
Test
Parameter
Intercept
Lutzomia trapidoi abundance inside
ELISA
the houses
Dog Age
Intercept
ANY (ELISA or
Lutzomia trapidoi abundance inside
IFAT)
the houses
Dog Age
*statistically significant (P<0.05)
Odds
Ratio
1
Estimate (± sandwich
S.E.)
---
---
3.39
1.22 (± 0.39)
3.122*
1.35
1
0.30 (± 0.09)
---
3.395*
---
3.56
1.27 (± 0.42)
3.035*
1.60
0.47(± 0.15)
3.058*
Z
Supplement S1 Seropositivity thresholds from mixture models
Standard methodologies for seropositivity were usually based on control groups, from which a threshold
for seropositivity was obtained by adding three standard deviations to their mean antibody titre [31].
Nevertheless, this method was prone to be biased and misclassify seropositive and seronegative
individuals because it is not robust to small changes in antibody titres that can emerge from seasonality
and/or small variations in laboratory assay performance [30]. To overcome the likelihood of
misclassification, a novel method based on a finite mixture model has been proposed to determine a
more sensitive threshold for seropositivity based on the distribution of titres, measured via optical
density in a spectrophotometer, in a population exposed to a pathogen [29,30]. Basically, the finite
mixture model assumes the statistical distribution (f(x)) of antibody titres, or optical densities, (x) in a
exposed population to be a mixture of the distribution of titres from positive (P(x)) and negative
individuals (N(x)) according to the following equation [29,30]:
f ( x) ( P( x)) (1 )( N ( x))
(S1.1)
Where π is the proportion of titres belonging to each category. Maximum likelihood estimates for the
means and standard deviations of P and N distributions can be estimated and a threshold for
seronegativity can be estimated as the mean of the distribution with the smallest mean (i.e., that of the
negative individuals) plus three standard deviations [29].
Supplement S2 The Dendukuri and Joseph method to estimate sensitivity and specificity of two
diagnostic tests in one Population
The Dendukuri and Joseph method is based on the Hui and Walter (HW) equations[48]. The HW method
allows the estimation of sensitivity and specificity of two diagnostic tests in two populations using the
number of double positives (i.e., positively diagnosed individuals by the two tests), double negatives,
and those positive by only one of the diagnostic tests (presented in Table S1 for our study data). Briefly,
the Dendukuri and Joseph [33] method modifies the HW equations to obtain estimates in the presence
of non-independent diagnostics, i.e., diagnostics whose sensitivity and/or specificity are likely correlated.
Given lack of degrees of freedom for maximum likelihood parameter estimation when the two tests are
performed on the same population (seven parameters on four observations), the subsequent nonidentifiability of the parameters, and the bias of the HW maximum likelihood estimator when diagnostic
tests are correlated [32,33,49], inferences for the Dendukuri and Joseph method require a Bayesian
framework for parameter inference.
Dendukuri and Joseph [33], as well as Branscum et al [32], also recognized the likely large influence of
the informative priors required for the estimation of identifiable parameters in their modified HW
equations. To better understand the role of the prior distributions on parameter estimates, Dendukuri
and Joseph [33] and Branscum et al [32] recommend to perform a sensitivity test increasing the range
for quantile distribution in the priors assumed for the specificity and sensitivity. To achieve such a goal
we decreased the value of the α parameter in the beta distribution defining the prior distribution for the
specificity of ELISA and IFAT, and the sensitivity of IFAT. Results are presented in Table S2.
Supplement S3 R code for the maximum likelihood estimation of the force of infection (λ) from an
age-specific seroprevalence curve
library(bbmle)
### Model fitting requires the use of the bbmle library
sero<-function(lambda,sd){
-sum(dnorm(seroprevalence,mean=(1-exp(lambda*age)),sd=sd,log=T))
}
###
###
###
###
###
###
sero is the maximum likelihood function to be optimized. Its parameters
are lambda which corresponds to λ in equation (2) and sd, which is the
standard deviation of the error.
For the maximum likelihood estimation we need a vector with age specific
seroprevalence and age to define the relations presented in equation 2.
the sum corresponds the log-likelihood expression for the model, i.e.,
(ω+1) ln(sd)
1
2
−𝜆𝑎
### L(S(a)|λ, var) = ∑ω
− 2 ∑𝑤
)) , where κ is a constant
a=0 κ −
𝑎=0 (𝑆(𝑎) − (1 − 𝑒
2
2sd
### from the normal distribution, ω is the maximum age in the dog population
### and sd2 is the variance of the error.
modelfit=mle2(sero,start=list(lambda=-.16,sd=0.14))
### mle2 is a command to fit the maximum likelihood model, with initial
### guesses for the parameters defined in “start=list(…)”
summary(modelfit)
### summary is a command that summarizes the output from the maximum
### likelihood estimation
confint(modelfit)
### confint is a command that estimates the 95% confidence intervals for the
### parameters in the maximum likelihood function
Supplement S4 Basic Reproduction number (R0) estimation when mortality is neither constant nor
negligible and the force of infection (λ) is age independent and assumed to be at equilibrium
Anderson and May [43] present that in a homogeneously mixed host population, under the assumption
of “weak homogenous mixing”, i.e., that new infections appear at rate proportional to the number of
susceptible hosts, R0 is inversely related to the fraction of susceptible hosts (x*) at equilibrium:
R0
1
S*
(S4.1)
The fraction of susceptible hosts (S*) at equilibrium can be decomposed as a function of the total
number of infected hosts ( X ) divided the total number of hosts ( N ), over all ages (a), as follows:
S*
X
N
0
0
X (a)da
(S4.2)
N (a)da
Where N is an age structured population that can be decomposed as follows:
N N (0)l (a)
(S4.3)
0
Which can be further simplified to:
N N ( 0) l ( a )
(S4.4)
0
Similarly, X is the age structured population of infected individuals that can be decomposed as follows:
X N (0) e al (a)
(S4.5)
0
Substituting (S4.4) and (S4.5) in (S4.2) and (S4.1) we have:
R0
e
e0
a
(S4.6)
l (a )
0
Where the numerator is the life expectancy in a population (e0), i.e., the expected time units a newborn
will survive until his/her death [46,50], which is defined by the following equation:
e0 l (a )
0
(S4.7)
Equation S4.6 can be approximated under two limit considerations[43]:
(1) When mortality is negligible up to the life expectancy age (e0, l(a< e0)=1), after which survival
becomes negligible(i.e., l(a> e0)=0):
e0
R0
w
e
a
l (a)
0
e0
1 e
1
e0
(S4.8)
Where S4.8 can be fairly well approximated by:
R0 e0
(S4.9)
Or can be re-expressed as the ratio between the age expected age for the first infection (A):
R0
e0
A
(S4.10)
Since under the static assumptions[43]:
A
1
(S4.11)
(2) When mortality is constant through all ages (l(a)=-exp(μa)):
R0
e0
e
a a
e0
(S4.12)
e
0
Since the life expectancy (e0) is also the inverse of (μ), the average mortality rate [46]:
e0
1
(S4.13)
And replacing S4.12 in S4.11 we have:
R0 1
e0
A
(S4.14)
And equation that has been used when estimating R0 for leishmaniasis transmission in dogs [23,51].
Nevertheless, none of those approximations are likely good to estimate R0 in populations where
mortality accelerates with age, a pattern observed in nature [46] or when mortality is, more generally,
not constant. In those circumstances, the best estimate would probably to use equation (S4.6) which
can estimate R0 in absence of the biases imposed by assumptions of equations (S4.10) and (S4.14).
Nevertheless, it is important to highlight that equation S4.6 assumes: (i) homogenous pathogen
exposure, (ii) no significant delay between infection and seropositivity, (iii) the force of infection is
constant and age independent, and (iv) infection and demographic patterns in the host population are
at equilibrium[43].
Figure S1 Smoothed density of optical densities for the ELISA test. In the x axis the native values are an
artifact of the smoothing used to obtain the probability density in the y axis.
Table S1 Cross-classified canine cutaneous leishmaniasis diagnostic test results from ELISA and IFAT.
Diagnostic ELISA
Test
+
+ 13 2
IFAT
- 11 25
Table S2 Diagnostic test sensitivity and specificity parameter estimate sensitivity to changes in the
prior distribution. In the table Prior indicates the parameters used for the Beta prior distribution,
Parameter the name of the parameter (rhoD is the correlation between positive results and rhoDc
between negative results), Test the name of the diagnostic test and 95 % CI, the 95 % Bayesian credible
intervals of the estimates. Further details about the senisitivity analysis are presented in Supplement S1.
Prior
Parameter Test
+
ELISA
Beta(α=15.034,β=2.559)
Sensitivity
+
IFAT
Beta(α=9.628,β=3.876)
+
ELISA
Beta(α=15.034,β=2.559)
Specificity
+
IFAT
Beta(α=10.034,β=2.559)
---rhoD
-----rhoDc
--ELISA
Beta(α=15.034,β=2.559)
Sensitivity
IFAT
Beta(α=9.628,β=3.876)
ELISA
Beta(α=15.034,β=2.559)
Specificity
IFAT
Beta(α=5.034,β=2.559)
---rhoD
-----rhoDc
--ELISA
Beta(α=15.034,β=2.559)
Sensitivity
IFAT
Beta(α=6.628,β=3.876)
ELISA
Beta(α=15.034,β=2.559)
Specificity
IFAT
Beta(α=10.034,β=2.559)
---rhoD
-----rhoDc
--ELISA
Beta(α=15.034,β=2.559)
Sensitivity
IFAT
Beta(α=3.628,β=3.876)
ELISA
Beta(α=15.034,β=2.559)
Specificity
IFAT
Beta(α=10.034,β=2.559)
---rhoD
-----rhoDc
--ELISA
Beta(α=15.034,β=2.559)
Sensitivity
IFAT
Beta(α=9.628,β=3.876)
ELISA
Beta(α=10.034,β=2.559)
Specificity
IFAT
Beta(α=10.034,β=2.559)
---rhoD
-----rhoDc
--ELISA
Beta(α=15.034,β=2.559)
Sensitivity
IFAT
Beta(α=9.628,β=3.876)
ELISA
Beta(α=5.034,β=2.559)
Specificity
IFAT
Beta(α=10.034,β=2.559)
---rhoD
-----rhoDc
--+
Results Presented in Table 1 of the main article
95 % CI
0.67 0.90
0.38 0.64
0.62 0.97
0.48 0.95
-0.59 -0.13
-0.39 0.77
0.69 0.95
0.36 0.63
0.60 0.97
0.24 0.90
-0.57 0.04
-0.71 0.65
0.68 0.88
0.36 0.61
0.63 0.97
0.62 0.97
-0.60 -0.18
-0.25 0.80
0.69 0.89
0.33 0.59
0.64 0.97
0.61 0.97
-0.61 -0.18
-0.24 0.80
0.67 0.89
0.39 0.67
0.43 0.96
0.61 0.97
-0.59 -0.10
-0.54 0.77
0.66 0.95
0.41 0.87
0.20 0.88
0.58 0.96
-0.56 0.49
-0.90 0.59
Table S3 Model Selection for the best binomial generalized linear model explaining the odds of
cutaneous leishmaniasis seropositivity by any test (ELISA or IFAT) in dogs at the household level. In the
table SFA = Sand Fly abundance, Total = domiciliary + peridomiciliary. The best model is bolded.
Model
Selection
Round
0
0
0
1
0
1
1
1
2
3
4
5
Model Structure
AIC
ΔAIC
Total SFA (C)
Domiciliary SFA (DC) + peridomiciliary SFA (PDC)
Total Lutzomyia panamensis abundance (pana) + Total Lutzomyia trapidoi
abundance (trapi)
trapi
Domiciliary pana (dpana) + peridomiciliary pana (ppana) + domiciliary
trapi (dtrapi) + peridomiciliary trapi (ptrapi)
dpana + dtrapi +ptrapi
dpana + dtrapi
dtrapi
dtrapi +Peridomicile index (pi) + Vegetation index (vi) + housing
destituness index (hdi) + number of humans with open Leishmaniasis
lessons (actL) + number of humans with past Leishmaniasis Lessons
(pasL)+ number of humans (H) + richness of domestic animals (da) +
richness of wildlife animals (wa) + index of domestic animal abundance
(ida) + index of wildlife animal presence (iwa)
dtrapi +vi+H+ida+iwa
dtrapi +vi+H+iwa
dtrapi +H
50.97
51.03
6.16
6.22
52.98
8.17
51.47
6.66
49.29
4.48
47.29
45.42*
46.09*
2.48
-----
50.57
5.76
45.60
45.60
44.81*
0.79
0.79
---
*These nested models were not significantly different (P>0.05). Therefore, the simplest (dtrapi as
unique covariate) model was selected as best.
Table S4 Model Selection for the best binomial generalized linear model explaining the odds of
cutaneous leishmaniasis seropositivity by ELISA in dogs at the household level. In the table SFA= Sand Fly
abundance and Total = domiciliary + peridomiciliary. The best model is bolded.
Model
Selection
Round
0
0
0
1
0
1
1
1
2
3
4
Model Structure
AIC
ΔAIC
Total SFA (C)
Domiciliary SFA (DC) + peridomiciliary SFA (PDC)
Total Lutzomyia panamensis abundance (pana) + Total Lutzomyia trapidoi
abundance (trapi)
trapi
domiciliary pana (dpana) + peridomiciliary pana (ppana) + domiciliary trapi
(dtrapi) + peridomiciliary trapi (ptrapi)
dpana + dtrapi + ptrapi
dtrapi + ptrapi
dtrapi
dtrapi + Peridomicile index (pi) + Vegetation index (vi) + housing
destituness index (hdi) + number of humans with open Leishmaniasis
lessons (actL) + number of humans with past Leishmaniasis Lessons (pasL)+
number of humans (H) + richness of domestic animals (da) + richness of
wildlife animals (wa) + index of domestic animal abundance (ida) + index of
wildlife animal presence (iwa)
dtrapi+ida+da
dtrapi+ida
50.52
51.91
4.51
5.90
52.05
6.04
50.45
4.44
49.58
3.57
47.59
46.28
46.01
1.58
0.27
---
61.91
15.90
47.88
47.25
1.87
1.24
Table S5 Model Selection for the best logistic generalized estimating equations model explaining dog
cutaneous leishmaniasis seropositivity by any test (ELISA or IFAT). The best model is bolded.
Model
Selection
Round
0
0
1
3
Model Structure
Total Lutzomyia trapidoi abundance (trapi)
Domiciliary Lutzomyia trapidoi abundance (dtrapi)
dtrapi+ Peridomicile index (pi) + Vegetation index (vi) + housing
destituness index (hdi) + number of humans with open Leishmaniasis
lessons (actL) + number of humans with past Leishmaniasis Lessons (pasL)+
number of humans (H) + richness of domestic animals (da) + richness of
wildlife animals (wa) + index of domestic animal abundance (ida) + index of
wildlife animal presence (iwa)+ poor physical condition (ppc) +age + sex +
sleep inside the house (sih) +cutaneous lessons (cul) + dewormed (dew)
+ectoparasites (ect)
dtrapi+age
QIC
ΔQIC
74
69
16
11
77
19
58
---
Table S6 Model Selection for the best logistic generalized estimating equations model explaining dog
cutaneous leishmaniasis seropositivity by ELISA. The best model is bolded.
Model
Selection
Round
0
0
1
2
Model Structure
Total Lutzomyia trapidoi abundance (trapi)
Domiciliary Lutzomyia trapidoi abundance (dtrapi)
dtrapi+ Peridomicile index (pi) + Vegetation index (vi) + housing
destituness index (hdi) + number of humans with open Leishmaniasis
lessons (actL) + number of humans with past Leishmaniasis Lessons (pasL)+
number of humans (H) + richness of domestic animals (da) + richness of
wildlife animals (wa) + index of domestic animal abundance (ida) + index of
wildlife animal presence (iwa)+ poor physical condition (ppc) +age + sex +
sleep inside the house (sih) +cutaneous lessons (cul) + dewormed (dew)
+ectoparasites (ect)
dtrapi+age
QIC
ΔQIC
74
67
12
5
85
13
62
---
Table S7 R0 estimates assuming an insignificant or a constant mortality
Mortality Assumption
Insignificant up to the life expectancy age (equation S4.10
in supplement S4)
Constant (equation S4.14 in supplement S4)
Diagnostic
ELISA
IFAT
Any (ELISA and/or IFAT)
ELISA
IFAT
Any (ELISA and/or IFAT)
R0
0.64
0.31
0.85
1.64
1.31
1.85
S.E.
0.085
0.024
0.086
0.085
0.024
0.086
1. Herrer A, Christensen HA (1976) Epidemiological Patterns of Cutaneous Leishmaniasis in Panama: III.
Endemic Persistence of the Disease. The American Journal of Tropical Medicine and Hygiene 25:
54-58.
2. Herrer A, Christensen HA (1976) Natural Cutaneous Leishmaniasis among Dogs in Panama. The
American Journal of Tropical Medicine and Hygiene 25: 59-63.
3. Sokal RR, Rohlf FJ (1994) Biometry: The Principles and Practices of Statistics in Biological Research.
New York, NY: W. H. Freeman. 880 p.
4. Santaella J, Ocampo CB, Saravia NG, Méndez F, Góngora R, et al. (2011) Leishmania (Viannia) Infection
in the Domestic Dog in Chaparral, Colombia. The American Journal of Tropical Medicine and
Hygiene 84: 674-680.
5. Aguilar CM, Fernandez E, Fernandez Rd, Deane LM (1984) Study of an outbreak of cutaneous
leishmaniasis in Venezuela: the role of domestic animals. Memorias Do Instituto Oswaldo Cruz
79: 181-195.
6. Falqueto A, Sessa PA, Varejão JBM, Barros GC, Momen H, et al. (1991) Leishmaniasis due to
Leishmania braziliensis in Espírito Santo state, Brazil: further evidence on the role of dogs as a
reservoir of infection for humans. Memorias Do Instituto Oswaldo Cruz 86: 499-500.
7. Falqueto A, Coura JR, Barros GC, Grimaldi Filho G, Sessa PA, et al. (1986) Participação do cão no ciclo
de transmissão da Leishmaniose tegumentar no município de Viana, Estado do Espírito Santo,
Brasil. Memorias Do Instituto Oswaldo Cruz 81: 155-163.
8. Quaresma PF, Rêgo FD, Botelho HA, da Silva SR, Moura AJ, et al. (2011) Wild, synanthropic and
domestic hosts of Leishmania in an endemic area of cutaneous leishmaniasis in Minas Gerais
State, Brazil. Transactions of the Royal Society of Tropical Medicine and Hygiene 105: 579-585.
9. Quaresma PF, Carvalho GMdL, Ramos MCdNF, Andrade Filho JD (2012) Natural Leishmania sp.
reservoirs and phlebotomine sandfly food source identification in Ibitipoca State Park, Minas
Gerais, Brazil. Memorias Do Instituto Oswaldo Cruz 107: 480-485.
10. Santos JMLd, Dantas-Torres F, Mattos MRF, Lino FRL, Andrade LSS, et al. (2010) Prevalência de
anticorpos antileishmania spp em cães de Garanhuns, Agreste de Pernambuco. Revista da
Sociedade Brasileira de Medicina Tropical 43: 41-45.
11. Figueredo LA, de Paiva-Cavalcanti M, Almeida EL, Brandão-Filho SP, Dantas-Torres F (2012) Clinical
and hematological findings in Leishmania braziliensis-infected dogs from Pernambuco, Brazil.
Achados clínicos e hematológicos em cães infectados por Leishmania braziliensis de
Pernambuco, Brasil 21: 418-420.
12. Dantas-Torres F, de Paiva-Cavalcanti M, Figueredo LA, Melo MF, da Silva FJ, et al. (2010) Cutaneous
and visceral leishmaniosis in dogs from a rural community in northeastern Brazil. Veterinary
Parasitology 170: 313-317.
13. Brandão-Filho SP, Brito ME, Carvalho FG, Ishikaw EA, Cupolillo E, et al. (2003) Wild and synanthropic
hosts of Leishmania (Viannia) braziliensis in the endemic cutaneous leishmaniasis locality of
Amaraji, Pernambuco State, Brazil. Transactions of the Royal Society of Tropical Medicine and
Hygiene 97: 291-296.
14. Dantas-Torres F (2007) The role of dogs as reservoirs of Leishmania parasites, with emphasis on
Leishmania (Leishmania) infantum and Leishmania (Viannia) braziliensis. Veterinary Parasitology
149: 139-146.
15. Zanzarini PD, Santos DRd, Santos ARd, Oliveira Od, Poiani LP, et al. (2005) Leishmaniose tegumentar
americana canina em municípios do norte do Estado do Paraná, Brasil. Cadernos De Saude
Publica 21: 1957-1961.
16. Santos GPLd, Sanavria A, Marzochi MCdA, Santos EGOBd, Silva VL, et al. (2005) Prevalência da
infecção canina em áreas endêmicas de leishmaniose tegumentar americana, do município de
Paracambi, Estado do Rio de Janeiro, no período entre 1992 e 1993. Revista da Sociedade
Brasileira de Medicina Tropical 38: 161-166.
17. Heusser Júnior A, Bellato V, Souza APd, Moura ABd, Sartor AA, et al. (2010) Leishmaniose
tegumentar canina no município de Balneário Camboriú, Estado de Santa Catarina. Revista da
Sociedade Brasileira de Medicina Tropical 43: 713-718.
18. Reithinger R, Davies CR (1999) Is the domestic dog (Canis familiaris) a reservoir host of American
cutaneous leishmaniasis? A critical review of the current evidence. The American Journal of
Tropical Medicine and Hygiene 61: 530-541.
19. Cardenas R, Sandoval CM, Rodriguez-Morales AJ, Bendezu H, Gonzalez A, et al. (2006) Epidemiology
of American tegumentary leishmaniasis in domestic dogs in an endemic zone of western
Venezuela. Bulletin de la Societe de Pathologie Exotique 99: 355-358.
20. Marco JD, Padilla AM, Diosque P, Fernández MM, Malchiodi EL, et al. (2001) Force of infection and
evolution of lesions of canine tegumentary leishmaniasis in Northwestern Argentina. Memorias
Do Instituto Oswaldo Cruz 96: 649-652.
21. Castro EA, Thomaz-Soccol V, Augur C, Luz E (2007) Leishmania (Viannia) braziliensis: Epidemiology of
canine cutaneous leishmaniasis in the State of Paraná (Brazil). Experimental Parasitology 117:
13-21.
22. Padilla AM, Marco JD, Diosque P, Segura MA, Mora MC, et al. (2002) Canine infection and the
possible role of dogs in the transmission of American tegumentary leishmaniosis in Salta,
Argentina. Veterinary Parasitology 110: 1-10.
23. Reithinger R, Espinoza JC, Davies CR (2003) The transmission dynamics of canine american cutaneous
Leishmaniasis in Huánuco, Perú. The American Journal of Tropical Medicine and Hygiene 69:
473-480.
24. Pugedo H, Barata RA, França-Silva JC, Silva JC, Dias ES (2005) HP: um modelo aprimorado de
armadilha luminosa de sucção para a captura de pequenos insetos. Revista da Sociedade
Brasilera de Medicina Tropical 38: 70- 72.
25. Calzada JE, Saldaña A, Rigg C, Valderrama A, Romero L, et al. (2013) Changes in phlebotomine sand
fly species composition following insecticide thermal fogging in a rural setting of western
Panamá. PLoS One 8: e53289.
26. Young DG, Duncan MA (1994) Guide to the identification and geographic distribution of Lutzomyia
sand flies in Mexico, the West Indies, Central and South America (Diptera: Psychodidae).
Gainesville, FL: Associated Publishers. 881 p.
27. Saldaña A, Chaves LF, Rigg CA, Wald C, Smucker JE, et al. (2013) Clinical Cutaneous Leishmaniasis
Rates Are Associated with Household Lutzomyia gomezi, Lu. panamensis, and Lu. trapidoi
Abundance in Trinidad de Las Minas, Western Panama. The American Journal of Tropical
Medicine and Hygiene 88: 572-574.
28. Chaves L, Calzada J, Rigg C, Valderrama A, Gottdenker N, et al. (2013) Leishmaniasis sand fly vector
density reduction is less marked in destitute housing after insecticide thermal fogging. Parasites
& Vectors 6: 164.
29. Stewart L, Gosling R, Griffin J, Gesase S, Campo J, et al. (2009) Rapid Assessment of Malaria
Transmission Using Age-Specific Sero-Conversion Rates. PLoS ONE 4: e6083.
30. Bretscher M, Supargiyono S, Wijayanti M, Nugraheni D, Widyastuti A, et al. (2013) Measurement of
Plasmodium falciparum transmission intensity using serological cohort data from Indonesian
schoolchildren. Malaria Journal 12: 21.
31. Dye C, Vidor E, Dereure J (1993) Serological diagnosis of leishmaniasis: on detecting infection as well
as disease. Epidemiology & Infection 110: 647-656.
32. Branscum AJ, Gardner IA, Johnson WO (2005) Estimation of diagnostic-test sensitivity and specificity
through Bayesian modeling. Preventive Veterinary Medicine 68: 145-163.
33. Dendukuri N, Joseph L (2001) Bayesian approaches to modeling the conditional dependence
between multiple diagnostic tests. Biometrics 57: 158-167.
34. Faraway JJ (2006) Extending the Linear Model with R: Generalized Linear, Mixed Effects and
Nonparametric Regression Models Boca Raton: CRC Press.
35. Faraway JJ (2004) Linear Models with R. Boca Raton: CRC Press.
36. Christensen HA, Fairchild GB, Herrer A, Johnson CM, Young DG, et al. (1983) The ecology of
cutaneous leishmaniasis in the republic of Panama. Journal of Medical Entomology 20: 463-484.
37. Christensen HA, de Vasquez AM, Petersen JL (1999) Short report epidemiologic studies on cutaneous
leishmaniasis in eastern Panama. The American Journal of Tropical Medicine and Hygiene 60:
54-57.
38. Miranda A, Carrasco R, Paz H, Pascale JM, Samudio F, et al. (2009) Molecular Epidemiology of
American Tegumentary Leishmaniasis in Panama. The American Journal of Tropical Medicine
and Hygiene 81: 565-571.
39. Venables WN, Ripley BD (2002) Modern applied statistics with S. New York: Springer.
40. Chaves LF (2010) An Entomologist Guide to Demystify Pseudoreplication: Data Analysis of Field
Studies With Design Constraints. Journal of Medical Entomology 47: 291-298.
41. Pan W (2001) Akaike's Information Criterion in Generalized Estimating Equations. Biometrics 57:
120-125.
42. Muench H (1959) Catalytic models in epidemiology. Cambridge, MA: Harvard University Press.
43. Anderson RM, May RM (1991) Infectious diseases of humans: dynamics and control. Oxford: OXford
University Press.
44. Bolker BM (2008) Ecological Models and Data in R. Princeton Princeton University Press.
45. Southwood TRE (1978) Ecological Methods. London: Chapman & Hall. 524 p.
46. Carey JR (2003) Longevity: the biology and Demography of life span. Princeton, NJ, USA: Princeton
University Press.
47. Krebs CJ (1998) Ecological Methodology: Benjamin Cummings. 624 p.
48. Hui SL, Walter SD (1980) Estimating the error rates of diagnostic tests. Biometrics 36: 167-171.
49. Johnson WO, Gastwirth JL, Pearson LM (2001) Screening without a "gold standard": The Hui-Walter
paradigm revisited. American Journal of Epidemiology 153: 921-924.
50. Carey JR (2001) Insect biodemography. Annual Review of Entomology 46: 79-110.
51. Quinnell RJ, Courtenay O, Garcez L, Dye C (1997) The epidemiology of canine leishmaniasis:
transmission rates estimated from a cohort study in Amazonian Brazil. Parasitology 115: 143156.