Lean Six Sigma: Overview
advertisement

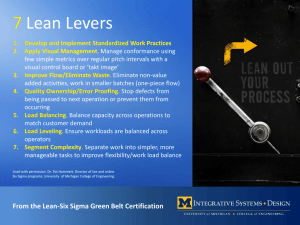
Session C9 #2287 Lean Six Sigma: The Pursuit of a Perfect Emergency Department Brandon D’Aloiso (bdd31@pitt.edu), Seth Young (say19@pitt.edu) Abstract— This paper will focus on the use of the Lean LEAN VS. SIX SIGMA Six Sigma principles in an emergency room setting. The current level of efficiency of emergency rooms will be examined and we will discuss the ways in which Lean Six Sigma principles can be implemented. Ways to lower infection rates and still keep wait times down will also be explored. Six Sigma methodologies are currently used in industry and are now being applied in hospital settings. Lean Six Sigma focuses on continuous improvement and waste reduction practices that can be used to achieve near perfection or “Six Sigma,” which is defined as six standard deviations from perfection. The focus of Lean, on the other hand, is on total elimination of waste, while still respecting the employees and their jobs by not firing personnel already in the system. The current status of emergency rooms is intolerable to patients and the need for reform practices, such as Lean Six Sigma, is apparent and growing. By bringing industrial engineers into the medical scene, hospitals can cut down on the level of waste tremendously. The goal of this paper will be to examine the intricate details of an emergency room, then move on to consider the implementation of a feasible solution that would ideally eliminate the current level of waste that could be life threatening. Lean and Six Sigma are two continuous improvement methodologies that are being used in conjunction with one another to lower waste and increase productivity in the business world. Those in the healthcare system however have taken notice of the effectiveness of these practices and have decided to attempt to implement these two systems into their own organizations. The use of Lean and Six Sigma in hospital settings is relatively new. Together, Lean and Six Sigma have been very successful in other settings. A hospital in New Jersey has been able to reduce the average time spent in their emergency department waiting for a doctor from four hours to about 38 minutes[1]. Using Lean and Six Sigma together has really allowed this hospital to reduce its waste, boost its productivity and still keep the whole process as safe, if not safer than it was before. What exactly are Lean and Six Sigma? Lean is a methodology pioneered by Taiichi Ohno of Toyota in 1988[2]. Ohno saw the ways in which he could boost his company’s productivity by eliminating all waste from his processes. Waste is defined below in greater detail, but for now we will consider waste to be all those things that do not contribute to the success of a process[2]. Waste can be anything from lag time between steps to an overstocked inventory in which the surplus expires or otherwise cannot be used[2]. Lean is focused on reducing the amount of waste present using flow charts and diagrams to allow a team of highly change-oriented individuals to identify waste in the process and think of ways in which these processes can be improved. These solutions to reduce waste can be anything from a checklist outlining the way to do a job correctly to a new step-by-step protocol to be used as a new standard, and even to something as simple as color-coding bins of supplies[1]. These practices not only allow for better productivity, but also, by allowing a team of employees to create these new systems and protocols it ensures that they will be successful because the employees have a vested interest in their implementation. Lean is only one half of the pair however; Six Sigma seems to be an opposing theory but together they are compatible. Six Sigma does not focus on the elimination of waste but instead it focuses on the minimization of defects. Six Sigma was created by the Motorola Company in 1986[1]. Six Sigma was developed for similar reasons as Lean and is used in similar situations. Six Sigma is defined as six standard deviations from the optimal product or having 3.4 defects per million production opportunities[3]. Six Sigma seems to be as near perfection as is possible and is something companies using the Six Sigma methodologies should strive Key Words— Continuous Improvement, Emergency Department, Healthcare, Lean, Six Sigma, Waste Elimination LEAN SIX SIGMA: OVERVIEW On average the wait time in emergency departments is alarmingly high. On top of that, the number of accidents by care professionals continues to rise. These issues are not due to a lack of knowledge or skill by the medical staff, but rather a faulty process by which they operate. Over recent years, hospitals, especially emergency departments, have been taking advantage of the combination of two continuous improvement processes, Lean and Six Sigma. These processes both address problematic areas within organizations. Lean practices focus on the elimination of waste, while Six Sigma’s goal is to reach six standard deviations from perfection. Six Sigma does this by reducing defects, making a process ideally near perfection. The use of these practices in conjunction with one another has shown continuous improvement in hospitals. By lowering the number of defects and by reducing the amount of waste the two practices have led hospitals to not only achieve higher efficiency and safety, but also be successful in a more cost effective manner. University of Pittsburgh Swanson School of Engineering April 14, 2012 1 Brandon D’Aloiso Seth Young implementation of Lean practices, to be successful, one must first identify all the different kinds of waste that are present in the setting they are looking to improve. If waste cannot be identified, then how can it be eliminated? Taiichi Ohno, the inventor of the Toyota Manufacturing System and creator of Lean Manufacturing, identified seven different categories of waste that can be applied to any setting[2]. These broad categories help review the entire system and see the waste that is present everywhere, not just in one specific setting. The following are types of waste as defined by Ohno: defects, overproduction, transportation, waiting, inventory, motion, and over processing. An eighth category, human potential, was added later on by other theorists of Lean. to reach. Companies hope to attain Six Sigma using the two processes of DMADV and DMAIC[3]. These processes are defined in greater detail later in the paper but both focus on improving the design of existing and brand new systems to reduce the overall number of defects in a company or processes’ output. Six Sigma methodologies include identifying a problem, collecting and analyzing data on it, finding ways to improve the process and controlling the end result[1]. The people that carefully follow these steps are on teams formed of many different levels of Six Sigma knowledge. The different levels of Six Sigma are outlined by a Belt Hierarchy similar to Karate Belts; black being the highest level of knowledge and white being the lowest[1]. Black belts are usually people who hold high positions within a hospital and white belts are people on staff not directly involved with the team but still following its directives. The middle belts, Green and Yellow, are the actual team members focused on improving the hospital by following the DMADV and DMAIC metrics[3]. The Green Belts are usually those put in charge of Six Sigma projects and the Yellow Belts are usually the staff members (nurses and doctors) consulted to work at implementing the Green Belts work[3]. By having a team follow both of these metrics, DMADV for new processes and DMAIC for preexisting processes, organizations can ensure a faster, more efficient, and overall more cost effective process. These continuous improvements combined with the waste reduction techniques from Lean can assure that a process is at its peak performance level. The promising accomplishments of Lean and Six Sigma together are what have led to its cross over into the health care sector. By combining Lean and Six Sigma, hospital executives can assure that their hospital is top notch. By using these two processes, hospitals are safer, faster, and more cost effective. This new level of efficiency must translate all the way down from the executives to the janitorial staff. The emergency department (ED) is where this new level of efficiency can most easily be seen. In the emergency department Lean Six Sigma can reduce wait times, lower infection rates, and boost productivity for emergency department staff. Lean helps ED staff have successful outcomes for patients by assuring that every moment spent in the ED is not wasted (time, talent, etc.) and that patients are safer by removing all waste in the form of time spent having to redo steps performed incorrectly. By using Lean and Six Sigma, emergency departments across the country will revolutionize the process of getting treatment to a level that is much more acceptable to patients. These two continuous improvement practices used in conjunction with one another are the best hope at achieving this goal for modern emergency departments. TABLE I A Summary of the Types of Waste Defects Overproduction Transportation Waiting Inventory Motion Over Processing Human Potential Types of Waste Mistakes Overdone Steps Transport time is Waste Wait time between Steps Surplus that Expires Unnecessary Movements Doing Non-Valued Work Doctors and Nurses Idle Defects A defect is typically the most recognizable type of waste because of the real possibility for danger. Especially within the healthcare realm waste can cause a lot of harm because it is dealing directly with people’s lives. The basic definition of a defect is any work related action that is not done correctly the first time[2]. A situation such as this is not only problematic, but can also lead to other forms or waste such as a loss of time while the action is repeated, or the constant need to check for errors; slowing down the process versus moving at full speed knowing everyone did their job correctly. Defects are a common type of waste especially in emergency departments. A few examples include carts missing items that were not restocked or the dispensing of the wrong dosage of medication. It is estimated by the Institute of Medicine that 400,000 preventable drug-related injuries occur every year, because of illegible handwriting, misplaced decimal points, and many other defects within the processes[2]. It is easy to blame the doctor or nurse in these situations because most of the time they are human errors. When studying Lean, however, one must look at the bigger picture to try and figure out why they made this mistake. Typically a flaw in the process, rather than human error, causes most defects and waste. WASTE IN THE EMERGENCY DEPARTMENT Lean, by definition, is the total elimination of waste. But what exactly is waste? When studying and looking at the 2 Brandon D’Aloiso Seth Young because employees have multiple responsibilities[2]. Lastly in the waste of time spent waiting are the employees. This statement may make it sound like doctors and nurses are not doing their job, but actually, because of the process defects or delays in processes further up the system, the employees are forced to waste time waiting around. Other reasons for this waste involve their contracts and unevenly distributed workload among the employees[2]. In the emergency department, the waste of time by employees usually depends on the number of patients they must care for; therefore if only five patients are in the ED then many of the employees sit around and wait for their services to be called upon. The amount of employees is necessary waste because at any moment’s notice a busload of injured victims in critical condition could come in and the employees must be there to aid the victims. Overproduction Another category of waste is overproduction, which may sound impossible in an emergency department that is typically spread thin and always running around to keep up with the fast pace environment. Overproduction, however, can also refer to doing more than what is required for a patient or completing it sooner than needed[2]. This type of overproduction happens every day in emergency departments across the country. In many hospitals, a blood test and tox-screen of every patient through the door is required. While this protocol is intended to speed up the process of patient care, in reality it does just the opposite. Usually only 10% of those pre-screening procedures were necessary in the diagnosis of the patient, thus requiring nurses to do unnecessary work, wasting time[2]. Instead nurses could either wait to draw blood or only draw the blood from those who will obviously need that blood test. As far as providing services earlier than needed, another example of this type of over production is delivering medications too early. These medications are then sent back to the pharmacy, wasting the transporters time with extra trips to and from the pharmacy, and the pharmacist’s time by forcing them to reprocess the medications that are returned[2]. Inventory Another form of waste is excess inventory. Inventory can be considered waste because money is tied up in stocking the storage closets. This excess inventory however is just sitting on shelves and not being used right away. While it can be argued that this stock is eventually used, it could be explored using Lean what the optimal inventory to have stocked is. This process would be delicate would need to be studied closely because a fluctuation of supplies used on a weekly or monthly basis. On one side, a hospital cannot have a huge excess of product that will expire[2]. On the other hand, too few of a product in such a case would cause costly “run outs” of a specific supply. A mistake in inventory stocking, though seemingly small, could end up being devastating to a patient’s health. The hospital may need to expedite an order and pay extra[2]. Both of those scenarios involve waste of profits. Thus managing the right amounts of supplies and medications in a hospital is extremely important for both patient care and the bottom line for the hospital. Transportation The waste of transportation is common among the movement of patients and medical supplies in an emergency department. Since every patient treated is evaluated on a case-by-case basis, there is little to no way to prepare for every scenario in each patient’s room. This disorder and randomness results in frequent runs to the supply closet to get supplies or trips down the hall to get the only ENT Cart in the department. In addition, there are also frequent trips transporting the patient to and from the MRI room to the Catheterization Lab, etc. This waste of transportation is due to the poor layout of a hospital, which can be prevented with the future use of transportation-friendly layouts in design plans for new hospitals or in renovations[2]. Motion When managers see their employees constantly running around to get the job done, the managers equate activity with a hard worker. In reality, it may be that the employees must include all of this extra motion simply to do their job, wasting motion. This type of waste is the unnecessary movement by employees in the system. Waste like this is severe for nurses in the Emergency Department. In fact, it is estimated that nurses walk an average of 3.5-4.5 miles per twelve hour shift[2]. This leads to fatigue of the nurses’ physical and mental health which could lead to defects in their work[2]. If hospitals were to implement Lean practices by restructuring their layout of a department and move commonly used equipment and supplies to a more central and convenient location it would cut down on wasted of motion. This organization would also increase the time employees have to complete their other value added tasks. Waiting Probably the most recognizable type of waste, and the one that causes the most frustration for patients, is the waste of time spent waiting for care. This category can be broken up into smaller components based upon who or what is waiting around. Patients spend time waiting for the nurse to admit them to a room in the emergency department, sometimes for several hours. They then must wait for the doctor to see them and diagnose their problem. Finally, after that, they must wait to be released by the nurse and discharged[2]. This allows for much improvement by Lean practices. Products can also be stuck waiting around. A few examples include tubes of blood waiting to be tested, instruments needing sterilized, and pharmacy orders that wait on a cart 3 Brandon D’Aloiso Seth Young employees to organize the improvement efforts throughout the organization[4]. When referring to the Six Sigma methodologies, one must first distinguish between the applications of the process. There are two methodologies, both of which are identical for several steps but differ slightly depending on whether the system to which it is being applied is already established and looking to improve upon their process, or if one is starting a new process from nothing. The processes for an established setting are: define, measure, analysis, improve, control. (DMAIC) The phases for a newly established process are: define, measure, analysis, design, verify. (DMADV) In both cases the first three phases are identical, with a slight difference in the last two phases. The first phase of either process is the define phase. The initial process goal is to hone in everyone’s attention on the problem and define the optimal goal at the end of the project. One way of going about this is to write a project charter which defines the step by step process as well as boundaries of this project. Also, within the charter includes the possible outcomes and opportunities of the process, as well as risks, and SIPOC diagrams (suppliers, inputs, processes, outputs, customers) which are also drawn up by the team to pinpoint the elements of the process[4]. The measure phase is the next step in the Six Sigma process. The primary goal is the collection of data and information. Once the data is collected, the team must set the target number that they wish to reach in order for the process to be considered a success. From there on out, data will be collected on a regular basis and will be compared to the reference data that was initially collected[3]. The main use of this data is to determine the fundamental causes of the problems in the system. In the analyze phase, team members carefully study the data with different Six Sigma tools that provide definitive statistics about the areas that need improvement. This step specifically requires the knowledge of current employees within the system that can determine the cause for inefficiency[3]. Then the team brainstorm ideas to improve upon that flaw that would hopefully yield more concise statistical data. Over Processing The waste of over processing, defined by Graban, is doing work that is not valued by the customer, or caused by definitions of quality that are not aligned with patient needs[2]. Basically, it is doing something to a higher level of quality than what the patient expects or requires from an employee. In a healthcare setting, one possible example would be some of the information filled out on forms by nurses that is never used as data or for anything else[2]. These unnecessary forms and information take crucial time out of a nurse’s rounds while she could be taking care of patients. Instead of doing value added tasks she is doing non-value added tasks. Human Potential The waste of talent, the category added later to the initial seven categories of waste defined by Ohno, is a waste of employee ideas. Some still do not recognize this as a practice of Lean, but it could turn out to be the biggest waste of any. Human potential is amazingly large. Human beings are capable of doing more than they realize they can do and have the ability to think for themselves to identify their own waste. Many managers tend to try and suppress their employees’ ideas in fear of losing control, but this will cause employees to resent their boss and lose their desire to work hard and be creative thinkers[2]. As much as Industrial Engineers can be extremely helpful in healthcare settings, they do not know all of the ins and outs of a process like the employees do. Since the nurses deal with the process in the Emergency Department on a daily basis, they too should be listened to in productivity and Lean meetings. Identifying the waste in any system is crucial for Lean practices to be successful. It is impossible to fix a problem without knowing exactly what to fix. These eight types of waste help to specify all of the different wastes in a situation, especially an Emergency Department. STEPS TO ACHIEVING SIX SIGMA: D.M.A.I.C. AND D.M.A.D.V. While Lean is all about the removal of Waste and NonValue Added Tasks, Six Sigma is about reducing Defets caused by this waste. When one studies Six Sigma in depth, they realize the necessity of sticking to the strict methodology when going about implementing the process in a desired system. Six Sigma methodologies are a structured and rigorous approach to improving the efficiency of a process by eliminating the sources of variation. If one does not follow the methodologies, the Six Sigma process has a great chance of failure due to a weak study of processes with inappropriate tools for collecting and analyzing data, as observed by Vest and Gamm in 2009. Chakravorty considered the cause of the failed Six Sigma process to be due to a lack of implementation models to guide the Figure 1 DMAIC and DMADV in Summary[5] 4 Brandon D’Aloiso Seth Young of DMADV and DMAIC (outlined above) to identify places to reduce waste and also create new protocols that cut down on errors. The creation of these protocols, however, will never be enough. At first, high goals must be set that seem near impossible. The employees should be constantly reminded of these goals and of the hospitals progress towards these goals. By effectively showing nurses and doctors that Lean Six Sigma really is doing what they never thought possible, there will be a higher adoption and acceptance rate among all hospital employees. Another important way to ensure that employees stick to the newly designed protocols is to have some sort of employee recognition program. By allowing patients and other employees[1] to recognize doctors, nurses, and other hospital staff in some sort of system that really does reward employees at some set rate, employees are encouraged to take better care of the patients. A final way that hospitals can ensure the implementation and retention of Lean Six Sigma methodologies is to advertise them all over the hospital. Granted, most of the finer details should be left out, but by making posters that encourage patients to ask caregivers to wash their hands, ask about their care, et cetera, the leaders of the Lean Six Sigma initiative can have their own “police force” in the patients. Also, by having a mantra or saying such as: “Reduce Delay by: Delivering the RIGHT care, at the RIGHT time, to the RIGHT patient,”[6] the Lean Six Sigma methodologies are something that doctors and caregivers can never get out of their minds. Lean Six Sigma has the potential to revolutionize healthcare and specifically the Emergency Department. By overcoming these basic obstacles and any others that might crop up along the way, emergency departments can drastically reduce wait times, boost patient satisfaction, and ultimately increase profit margins making a trip to the emergency room something that is a little easier for patients and friendlier to a hospitals accounting department. The fourth phase depends on the process. In the DMAIC process, the improve phase takes the suggested ideas in the previous phase and implements them into the process. This involves the black belt to inform the employees of the changes and to oversee that the transition runs smoothly[3]. Similarly in the final phase of DMAIC, the black belt continues to monitor the process in the control phase and sustain the gains. His or her job is to manage and take control of any obstacles that arise with the sudden change[3]. When looking at the DMADV process, the fourth step is the design phase. This phase is to design new methodologies that will enhance the original process. Also, it prevents problems by solving with data analysis to achieve the goal of better efficiency. The final step is the verify process which involves continual monitoring if the project is already in place, or simulation to ensure that the future project will operate smoothly[3]. If one wishes to implement the Six Sigma process in their line of work, then one must follow the methodologies precisely, in order for it to be effective. Due to the different stages of a project, there are different processes to follow for each, which vary only slightly in the last two phases. More and more emergency departments are looking to Six Sigma to improve their efficiency, because of its past success at other hospitals. IMPLEMENTING SIX SIGMA While all of the methodologies and tools seem to work in theory, often times they fail to take hold in the actual work force. Part of this problem is excuses and a lack of motivation on the part of the employees. Employees feel that they are doing the best they can and blame others for any failures. When someone comes in preaching “Near Perfection,” they are rightly skeptical. They have been through many training and improvement seminars and believe that this is just the newest annoyance that management is forcing upon them. Lean Six Sigma has a fail rate of 50% within the first three years [1] simply because the implementation does not maintain a firm hold in the dayto-day practices of the employees. In order to ensure that Lean Six Sigma takes root, an implementation team must be formed of the most highly motivated and dedicated employees; people that want to find ways to improve. This team will spearhead the effort towards having a working environment free of waste and operating at Six Sigma. This team will be the highest level of the hierarchy of improvement. For example, in a hospital this team should be those in management positions of the different departments and the executives of the hospital. From there, each representative should have their own smaller team within their departments. As in the case of the Emergency Department, one nurse or doctor from each shift should be present at meetings to discuss problems they see during their rounds. These teams should follow the processes LEAN SIX SIGMA: CASE STUDIES In order to garner a full understanding of what Lean Six Sigma does and how it works case studies are important to look at. An interesting case study done in St. Mary’s Hospital in Hoboken[7], New Jersey focuses on how Six Sigma was able to improve the outcomes for patients that presented abdominal pain to ED doctors. The team first focused on a problem and created the following problem statement: “Cases presenting to ED with acute abdominal pain experience a delay in diagnosis of appendicitis resulting in over use of services, misdiagnosis and a delay in surgical intervention.” Dr. Christopher Valerian, a Six Sigma Black Belt, spearheaded the team. The team took on this project with a goal of lowering the length of stay of patient from four to two days and determined that to achieve this goal they must have an early surgical intervention of about six hours while still in the Emergency Department. The problem 5 Brandon D’Aloiso Seth Young After the implementation of their protocols the team collected new data on length of stay (Figure 4) and hours until surgery (Figure 5) are as follows. As seen from the data, using Six Sigma they were able to get the average length of stay in the ED down to 2.6 days and the average hours until surgery were almost cut in half to about 10.8 hours[7]. The team came very close to their original goal and was successful thanks to Six Sigma. Not only did the team create great improvements for patients but also saved the hospital about $153,000.00 annually[7]. They also found that their new triage and registration processes were so successful that other hospitals took them on as well. From the data of the hospital it is pretty clear that Six Sigma is a successful continuous improvement program, but what about Lean? In the Annals of Emergency Medicine, an experiment was performed to see to what degree Lean Process Improvement actually boosts ED productivity using the variables of length of stay(LOS), patient satisfaction (PS), percentage of people who left without being seen (LWSD), time for test results to come back, and patient volume changes (PV)[8]. with just shortening the decision time however is the fact that it is unsafe for the patient. In addition to keeping the diagnostic and intervention process safe, the hospital ED would save money by shortening the length of stay of their patients and earn more money by allowing new patients to come in at a larger rate. The team collected and analyzed data on two factors; length of stay (LOS) (Figure 2) and hours from entering the ED to their surgery (Figure 3). As can be seen from the Valerian team’s data, the average number of hours until surgery was at 21.6 hours and the length of their stay was about 4 and a half to 5 days. The team next outlines their possible solutions. They suggest that by creating both a new triage process and a new door to surgery protocol they can shorten the time that the patient spends in the hospital before and after surgery to a minimum. Also the team suggests that the type and number of diagnostic tests that should be performed should be standardized in order to assure that the patient only has to wait for the required tests rather than waste time waiting on tests that were not necessary in the first place. Descriptive Statistics Descriptive Statistics Variable: LOS Variable: LOS Anderson-Darling Normality Test A-Squared: P-Value: 1 3 5 7 Mean StDev Variance Skewness Kurtosis N 9 Minimum 1st Quartile Median 3rd Quartile Maximum 95% Confidence Interval for Mu 0.361 0.412 Anderson-Darling Normality Test A-Squared: P-Value: 4.47619 2.50238 6.26190 0.538963 -2.4E-01 21 1.0000 2.0000 4.0000 6.0000 10.0000 1 2 95% Confidence Interval for Mu 3.3371 3 4 5 6 3 4 5 Mean StDev Variance Skewness Kurtosis N 6 Minimum 1st Quartile Median 3rd Quartile Maximum 95% Confidence Interval for Mu 5.6153 1.96577 3.6136 2.0 2.5 3.0 3.5 2.6735 3.39787 95% Confidence Interval for Sigma 95% Confidence Interval for Median 95% Confidence Interval for Median 1.00000 1.00000 2.00000 4.25000 6.00000 95% Confidence Interval for Mu 95% Confidence Interval for Sigma 1.9145 1.280 0.002 2.68182 1.61500 2.60823 0.721144 -7.8E-01 22 1.24250 6.0000 2.30794 95% Confidence Interval for Median 95% Confidence Interval for Median FIGURE 2 1.97268 3.02732 FIGURE 4 Pre-Six Sigma Data on the Variable Length of Stay[7] Post-Six Sigma Data on the Variable Length of Stay[7] Descriptive Statistics Descriptive Statistics Variable: Hours Variable: Hours Anderson-Darling Normality T est A-Squared: P-Value: 0 20 40 60 80 100 95% Confidence Interval for Mu 1.928 0.000 Mean StDev Variance Skewness Kurtosis N 21.6162 21.1075 445.528 2.87249 10.0976 21 Minimum 1st Quartile Median 3rd Quartile Maximum 4.500 9.705 17.080 25.540 100.830 Anderson-Darling Normality T est A-Squared: P-Value: 2.5 7.5 12.5 17.5 Mean StDev Variance Skewness Kurtosis N 22.5 Minimum 1st Quartile Median 3rd Quartile Maximum 95% Confidence Interval for Mu 12.008 10 20 30 95% Confidence Interval for Mu 31.224 8.3320 30.481 6 95% Confidence Interval for Median 95% Confidence Interval for Median 10.901 2.2000 5.9975 9.7100 15.1600 23.9200 95% Confidence Interval for Mu 95% Confidence Interval for Sigma 16.149 0.496 0.192 10.8036 5.5745 31.0752 0.577669 -2.7E-01 22 7 8 9 10 11 12 13 14 15 13.2752 95% Confidence Interval for Sigma 4.2888 20.635 7.9663 95% Confidence Interval for Median 95% Confidence Interval for Median FIGURE 3 Pre-Six Sigma Data on the Variable of Hours to Surgery[7] 6.1286 FIGURE 5 Post-Six Sigma Data on the Variable Hours to Surgery[7] 6 14.2254 Brandon D’Aloiso Seth Young THE ANSWER Lean Six Sigma has been tried and tested by the healthcare system in recent years, and has been successful in those trials. Because of the many different types of waste found in an emergency department, the need for creating Lean Healthcare systems is a necessity. Once a Lean system is created, it is up to Six Sigma to boost productivity of that system and ensure the safety of patients. The primary goal of this revolutionary process in emergency departments is not to increase profit, but rather to improve upon patients’ health by minimizing waste and defects, and by decreasing the overall time spent waiting. This proven and effective process is available to emergency departments immediately. An ED that is trying to reform its practices but chooses to dismiss Lean Six Sigma is being simply counterproductive. If emergency departments were to use Lean Six Sigma, a trip to the emergency room would no longer be seen as an inconvenient process but as a healing opportunity. Each of these hospitals were measured for these variables for one year before Lean was implemented and asked that in implementing Lean they hire a Lean consultant to hold a 3-5 day training session for the staff. While all different, each of the training sessions taught inherently the same content. The staff learned Lean to the same levels and was prepared to implement it to the same effectiveness. They were told that a third party data recorder would be in to collect the data for the study[8]. They were to proceed with Lean for one year or until it was no longer effective. A chart of the Pre-Lean and Post-Lean data is below (Table II). TABLE II Lean Healthcare Trial Results[8] REFERENCES [1] J. Arthur. (2011). Lean Six Sigma for Hospitals. New York, NY: The McGraw Hill Companies. [2] M. Graban. (2009). Lean Hospitals. New York, NY: CRC Press. [3] “Six Sigma Online.” Aveta Business Group Belt Certification. [Online] Availible: http://www.sixsigmaonline.org/six-sigma-white-belt-training/ [4] Z. Ben Atallah and A. Ramudhin, (2010, December). “Improving Healthcare Reliability by Integrating Six-sigma in a Buisness Process Medeling and Analysis Strategy.” International Conference on IEEM. [Online]. Available: http://www.engineeringvillage2.org/controller/servlet/Controller?CID=quic kSearchDetailedFormat&SEARCHID=19a02031351190876cMa04prod2da ta2&DOCINDEX=1&database=7&format=quickSearchDetailedFormat [5] T. Pyzdek. (2003). “Six Sigma Training From the Source.” [Online]. Available: www.sixsigmatraining.org/dmaicdmadv [6] (2012) UPMC Mercy Hospital. Pamphlet/Poster. [7]Valerian, Christopher. (2004). “Six Sigma in Healthcare: Redefining the Emergency Room Process.” Healthcare Information and Management Information System Society:The Virgina Chapter. [Online]. Available: http://www.vahimss.org/index.html [8] Z. Anguelov, E. D., A. Eller, S. Singh and Diana Vetterick (2009). "Use of Lean in the Emergency Department: A Case Series of Four Hospitals." The Annals of Emergency Medicine. [Online]. Availible: http://www.sciencedirect.com/science/article/pii/S019606440900287X The hospitals were able to revolutionize their practices in the ED and Lean is what helped them to do that. Seeing patient satisfaction levels dropping is never a good sign but as the data was collected over a wide range and in different types of hospitals (2 large, teaching hospitals, 2 acute care, smaller hospitals) this fall in data points for patient satisfaction can be related to many uncontrollable variables and is not something to be focused upon. As seen so far, Lean Healthcare and Six Sigma practices help hospitals and their emergency departments. To find research on Lean Six Sigma in Emergency Departments and to cite studies that relate to both methodologies used together would be very hard to do. A lot of the research done on this pairing so far does not relate to healthcare. The practices are out there and it has been implemented, but no major studies have been done to comment on Lean Six Sigma for Healthcare’s tested effectiveness. Lean has been proven to be effective and so also has Six Sigma. The two practices share the same goals, complement each other in their processes, and have the potential to revolutionize emergency departments everywhere that use them. Therefore, the effectiveness of Lean Six Sigma cannot be disputed as a pair; as long as implementation is successful and lasting, they will be successful in all applications. ADDITIONAL RESOURCES Z. Anguelov, E. D., A. Eller, S. Singh and Diana Vetterick (2009). "Use of Lean in the Emergency Department: A Case Series of Four Hospitals." The Annals of Emergency Medicine. [Online]. Availible: http://www.sciencedirect.com/science/article/pii/S019606440900287X J. Antony, B. Sezen, and M. Tanner. (2007). “An Overview of Six Sigma Applications in Healthcare Industry.” International Journal of Health Care. [Online]. Available: www.emraldinsight.com/0952-6862.htm. J. Arthur. (2011). Lean Six Sigma for Hospitals. New York, NY: The McGraw Hill Companies. Z. Ben Atallah and A. Ramudhin, (2010, December). “Improving Healthcare Reliability by Integrating Six-sigma in a Buisness Process Medeling and Analysis Strategy.” International Conference on IEEM. [Online]. Available: http://www.engineeringvillage2.org/controller/servlet/Controller?CID=quic kSearchDetailedFormat&SEARCHID=19a02031351190876cMa04prod2da ta2&DOCINDEX=1&database=7&format=quickSearchDetailedFormat M. Graban. (2009). Lean Hospitals. New York, NY: CRC Press. 7 Brandon D’Aloiso Seth Young R. Holden, (2011, March). “Lean Thinking in Emergency Departments: A Critical Review”, Annals of Emergency Medicine, [Online]. Available: http://www.sciencedirect.com/science/article/pii/S0196064410013223 R. Lazurus, Ian, and Wendy M. Novicoff. (2004). “Six Sigma Enter the Healthcare Mainstream” Managed Healthcare Executive. [Online]. Available: http://search.ebscohost.com/login.aspx?direct=true&db=bth&AN=1206264 5&site=ehost-live. M. McClay, (2010, January). "Improving The Hospital Discharge Process With Six Sigma Methods." Quality Engineering. [Online]. Available: http://web.ebscohost.com/ehost/pdfviewer/pdfviewer?sid=84dd5c5d-6b9a4a7c-88f3-5e2608a5fca3%40sessionmgr12&vid=2&hid=8 M. Pepper and T. Spedding. (2009, October). “The Evolution of Lean Six Sigma.” International Journal of Quality & Reliabiliy Management. [Online]. Available: www.emeraldinsight.com/0265-671X.htm. T. Pyzdek. (2003). “Six Sigma Training From the Source.” [Online]. Available: www.sixsigmatraining.org/dmaicdmadv “Six Sigma Online.” Aveta Business Group Belt Certification. [Online] Availible: http://www.sixsigmaonline.org/six-sigma-white-belt-training/ (2012) UPMC Mercy Hospital. Pamphlet/Poster. Valerian, Christopher. (2004). “Six Sigma in Healthcare: Redefining the Emergency Room Process.” Healthcare Information and Management Information System Society:The Virgina Chapter. [Online]. Available: http://www.vahimss.org/index.html ACKNOWLEDGMENTS In writing this paper we contracted the help of many individuals and we wish to thank them now; thank you Dr. Carter Davidson and Nurse Amy Gerwig. We could not have done this without your help. Also thank you to the librarians in the Falk Library and Bevier Engineering Library, your assistance in finding sources was very appreciated. Also, we would like to thank our session chair, Professor Vidic, and co-chair, Taylor Robinson for both of your help. Your guidance and feedback really has allowed us to do our best on this paper. Finally a large thank you goes out to Dr. Budny and his helpers behind the scenes who put together this wonderful opportunity. 8