doc - Stanford University
advertisement

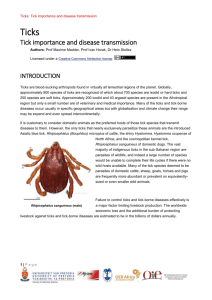
Alex Heaney Parasites and Pestilence 3/10/12 1 Ticks as Disease Vectors and African Tick Bite Fever Ticks are second only to mosquitoes as vectors of human infectious disease throughout the world. (Paddock, 2010) They can carry over 15 different pathogens, and cause over 16 human diseases. Consequently, ticks are extremely important transporters of human disease. This paper first discusses mechanisms and implications of ticks as human disease vectors and then delves into a specific African disease called African Tick Bite Fever. The goal of the paper is to provide information about ticks and African Tick Bite Fever, but also to illuminate gaps in our knowledge that should be addressed. Ticks are members of the arthropoda group of animal parasites. The arthropoda group also includes insects, spiders, and mites. There are two types of ticks that can be vectors for human disease: hard ticks and soft ticks. Significant differences exist between these two classes of ticks. Hard ticks have a hard scutum on their backs, which looks like a plate of armor, and they are generally very sexually dimorphic. Hard ticks tend to live in open environments and feed only when they need a blood meal to continue their life cycle. They can have one, two, or three hosts and generally live from several months to three years. Hard ticks take several days for one feeding, and can expand to 100 times their original size after a meal. In contrast, soft ticks do not have a hard scutum, and do not display sexual dimorphism. They tend to live in sheltered environments, and continually take blood meals from different hosts during their lives. Amazingly, soft ticks can live up to 10 years. Their blood meals are much shorter than hard tick blood meals, on the Heaney 2 order of minutes to hours, and they do not show dramatic increases in size after blood meals. Hard ticks are the vectors for diseases such as Lyme disease and Spotted Fever Rickettsiosis, while soft ticks are the vectors for Relapsing Fever Borreliosis and Q fever (Parola, 2001). The rest of this paper will focus on hard ticks, as they are the vectors for the diseases that will be discussed. Understanding the life cycle of ticks is vital to understanding their mechanisms for transmitting disease. The life cycle of a hard tick can include one, two, or three hosts. With three hosts, the tick life cycle generally takes around three years from the larva hatching to the death of the adult. First, a six legged larva hatches from an egg in the summer months. These larva are generally the size of a period on this page. In august, the larva seek a blood meal from a small mammal host such as a squirrel or a rodent. Once they obtain this blood meal, they fall off the host and live in the soil or vegetation for the winter. In the spring, the larva molts into an eight-legged nymph. This nymph seeks a blood meal from a slightly larger mammal such as a rabbit. Again, this nymph falls off the host and lives in the soil until the fall. At this point, the nymph finally molts into an adult tick. This eightlegged adult seeks a blood meal from a large mammal such as a cow or deer, and once the blood meal is obtained the female lays thousands of eggs in the soil and dies. (Parola, 2001) There are several important pieces of this life cycle. First, at each of the feeding times, obtaining a blood meal is essential for the tick’s survival. If the tick fails to find a host at any of these important developmental times, it does not enter the next stage of development and dies as a result. This has interesting implications Heaney 3 for vector control. If one of the host populations were theoretically wiped out, the ticks would not be able to obtain a blood meal and would therefore die. Another thing to note about the life cycle is that each tick feeds on different animals, but humans can be infected at any of the feeding stages of a tick. If ticks are questing on the low vegetation waiting for a horse to walk by, they will not reject a human if he or she walks by instead. So although ticks generally feed on domestic and wild animals, they are able to feed on humans and that facilitates disease spread. Lastly, ticks can carry diseases throughout their entire lives. There are three ways that a tick can become infected with a pathogen. First, they can feed on a host animal that is infected and ingest the pathogen in the host’s blood. Second, ticks can perform transovarial transmission for most diseases. This means that mothers can pass on the pathogen to their offspring. Third, co-feeding, or multiple ticks feeding at once on the same host, can cause infection. Thus, ticks can carry diseases at every point of their lives and each time a tick needs a blood meal, humans are at risk for catching the disease. (CDC on ticks) When it is time for the tick to have a blood meal, it has a couple methods for seeking out and attaching to a host animal. First, the tick can get to the top of low vegetation, like tall grass or weeds, and stick up its front legs. This is called questing. When a mammal brushes by this questing tick, the tick will grab on to the fur and therefore attach to the animal. (Vredevoe, 2011) Simultaneously, the tick is using chemical stimuli such as CO2, NH3, phenols, humidity, and aromatic chemicals to determine the location of mammals. The ticks also use airborne vibration and body temperatures to seek out mammal hosts. (Parola, 2001) Once the tick has arrived on Heaney 4 a host, it inserts a mouthpiece into the skin called the hypostoma. The hypostoma has hooks that, once inserted into the skin, serve to anchor it in place. This is the first of several mechanisms ticks use to remain on the host during their blood meals. (Parola, 2001) After the tick has inserted its hypostoma into the skin, it starts to secrete several different substances. First, it secretes a cementing substance that glues the hypostoma into place. At this point, there are hooks and cement keeping the tick’s mouthpiece lodged into the host’s skin. Second, the tick secretes immunosuppressive and anti-inflammatory chemicals that serve to help the tick go unnoticed by the host. If the host were to have an immune reaction or an inflammatory response, it is likely that the tick would be noticed and removed more quickly. Lastly, the tick is secreting an anticoagulant, which prevents the blood from clotting. This allows blood to flow freely into the tick and throughout the body. All of these secretions help the pathogen establish a foothold in the host. The longer a tick is connected to the skin, the more pathogens will be transferred into the host. Also if the blood is clotting near the tick’s mouth the pathogen will not be able to readily enter or travel though the host. (Sanson, 2011) Ticks can carry bacteria, viruses, and protozoa as pathogens for human disease and these pathogens are generally found in tick saliva. Once the hypostoma is in place, the tick begins it’s blood meal. Two to 15 days are required for a complete blood meal in a hard tick. Length of feeding depends on feeding stage, species of tick, type of host, and site of attachment. First there is a slow feeding period, and then around the third day the tick begins the rapid engorgement period. Heaney 5 In this time, the tick can increase to 100 times its original size. During feeding there are alternating periods of sucking blood and salivation. The periods of salivation allow the pathogen to enter the body and infect the host (Parola, 2001). Once the pathogen has entered the body, it travels through the blood stream and replicated in different cells of the host. In the past 20 years there has been a dramatic increase in the reported occurrence of tick borne diseases in the US. The rates of the most prevalent tick borne diseases in the US (Lyme Disease, Rocky Mountain Spotted Fever, and Ehrlichiosis) have all shot up over the past twenty years. Because of this increase in disease cases, an overall shift to increased awareness and worry about tick borne disease has occurred. Lyme disease is now the most commonly reported vector borne disease in the US, with about 10 cases for every 10,000 people annually. In addition, RMSF now has a higher rate of prevalence and a steeper increase in cases than ever before in recorded history. (Paddock, 2010) Although these facts are striking, the trends are not solely a result of an increase in prevalence of these diseases. The dramatic increase in reported cases can also be explained by an increase in disease recognition. Before 20 years ago, scientists did not have the knowledge or the tools to diagnose these diseases. Scientists are now identifying more pathogen species carried by ticks. Since 1984, 10 new strains of the rickettsiae bacteria have been recognized. More diagnostic techniques have recently been developed that will be discussed later in the paper, and vaccine research is currently being done. (Paddock, 2010) Heaney 6 Another interesting epidemiological trend is that tick borne disease prevalence varies in different populations. Within the US, as increased prevalence of Rocky Mountain Spotted Fever has been shown within American Indian Populations when compared to the national population. Not only is it much higher, but there has been a significant increase in reported cases of RMSF within American Indians starting in 2000, while there was only a slight national increase (Paddock, 2010). The author of this paper attributed this increase to cultural, racial and socioeconomic homogeneity existing among the American Indian population, but realistically this could also have been caused by many other factors. For example, there could have been a change in climate or environment for these people that fostered the transmission of Rock Mountain Spotted fever. Similarly, the specific tick vector could have been introduced into their environment. Several general hypotheses for why incidences of tick borne diseases are increasing have been put forward although the exact mechanisms and effects have yet to be shown. It is thought that warming temperatures and higher humidity may cause more tick borne disease transmission. In theory, this would increase tick fitness and therefore pathogen transmission. More people living near ideal tick ecosystems would also lead to increased contact between ticks and humans and would then increase the number of humans becoming infected. Tick vectors could be more competent given competitive advantages by environmental and genetic changes. Lastly, globalization of the world allows people infected with diseases to travel and introduce them to new places. The tick vectors themselves could also be transported to non-endemic areas and increase disease prevalence. Heaney 7 A case study for how the prevalence of tick borne disease can increase due many different factors is Lithuania at the end of Soviet Rule. After the war, Lithuania saw increases in tick borne diseases and there are many proposed reasons for this increase. The overall cause and effect are socio-economic transition created by the war and high tick borne disease incidence respectively. One possible effect of this socio-economic transition is a decline in agriculture. This will come up again in the context of tick control, but the main idea behind it is that ticks need vegetation to perch on or “quest” in order to attach to their hosts. Agriculture usually implies ridding land of the long grasses or shrubs that ticks normally would perch on. So, if we see a decline in agriculture there will be a regeneration of the shrubs and consequently more places for ticks to quest. Also a regeneration of shrubs will help foster rodent populations, providing more hosts for the young ticks to feed on. Therefore, a decline in agriculture will lead to a higher TBD incidence. There are other mechanisms, many which are mentioned above, such as reduced industrial pollution, sudden temperature increases, more hosts, and increased human exposure to ticks. All of these mechanisms emphasize the complex regulatory influences on tick borne diseases and ticks as vectors (Paddock, 2010). Ticks transmit a great variety of pathogenic microorganisms than any other arthropod vector group (Sanson, 2011). As mentioned before, there are a plethora of bacteria, protozoa, and virus pathogens that ticks can transmit. The bacteria that are going to be the topic of the following portion of this paper are the Rickettsiae bacteria. There are many diseases caused by different strains of these bacteria, such Heaney 8 as Rickettsiosis, Rocky Mountain spotted fever, and African Tick Bite Fever. Now, the paper will investigate African Tick Bite Fever. The vector of African Tick Bite Fever is the Ambylomma hebraeum and the Amblyomma variegatum tick species. The disease is caused by Rickettsia africae and Rickettsia parkeri bacteria. These bacteria, just like the pathogens discussed earlier, reside in the salivary glands of the tick and are transmitted to the human during a blood meal. Inside the tick, these bacteria multiply in the ovaries and the saliva. (Parola, 2001) This is extremely important because it allows the tick to pass the infection on to its progeny and infect a host simultaneously. Once the bacteria has entered the human, it spreads through the lymphatics in the body and travels to the vascular endothelial lining cells of the central nervous system, the lungs and the myocardium. Once the bacteria reach these destinations, they divide rapidly and cause trauma in the body (Mandell, 2011). African Tick Bite Fever is mainly endemic to Sub-Saharan Africa, but sometimes found in the Americas and the Caribbean. The distribution of the diseases is proportional to the presence of the two tick vector species. Data shows that there is a 30-100% infection rate of these vectors with the Rickettsia africae bacteria in most endemic countries (Perry, 2004). Interestingly, there are hardly any cases of African Tick Bite Fever reported within Africa itself. Most of the reported cases are of travelers that have gone to endemic countries and then returned home with the disease. Eldryd Perry, in Principles of Medicine, suggests two possible explanations for this phenomenon. First, it could be that people living in endemic countries acquire the disease early in Heaney 9 life and that the severity of the symptoms at that age is not serious. This would result in few cases being reported, as few people would seek medical care. Second, African Tick Bite Fever can easily be misdiagnosed as malaria because both diseases are febrile and there is co-endemicity in many African countries. Lastly, it could be that scientists are not monitoring African Tick Bite Fever in Africa yet (Perry, 2004). Now, imagine you are a doctor in a French Clinic. A 69 year old man is admitted with a fever, and the first thing you notice is that he has multiple eschars on his right leg. He complains of a headache, cough, nausea, chills and back pain. He also has extremely swollen lymph nodes on his right leg near the eschar. When you ask him about his medical history he reports that he has just returned from a trip to Zimbabwe where he was visiting farms and other rural areas. (Brouqui, 1997) This is a classic case of African Tick Bite Fever. African Tick Bite Fever has an incubation period of around 1-2 weeks. At this point, all patients will present with an eschar and possibly a rash. The eschar is where the tick inserted its hypostoma. It is usually inflamed and has a black scab in its center. An eschar is a very strong sign that the patient may be infected with a tick-transmitted disease. The rash consists of small red bumps, and they start around the wrists and ankles and then spread up the limbs. In some forms of Spotted Fever Rickettsiosis there is always a rash, but people with African Tick Bite Fever only present with this rash 50% of the time. Usually, the patient will have enlarged lymph nodes around the site of the eschar. This is due to the path of the bacteria. As stated previously, the bacteria initially travel through the body via the Heaney 10 lymph nodes and this causes irritation and swelling of the lymph nodes (Mandell, 2011). Later in the disease, people with African Tick Bite Fever almost always present with general symptoms such as a fever, headache, nausea, malaise, vomiting, and abdominal pain. Generally, the immune system can combat this disease and there are no severe consequences. The morbidity rate is extremely low, and data shows that up to 80% of Africans in endemic areas have antibodies against this disease. (Perry, 2004) However, serious complications do occur rarely. Damage to the epithelial cells can occur due to the bacteria replicating within those cells. Vascular inflammation, pulmonary edema, and skin necrosis can also occur (Mandell, 2011). Thinking back to the French patient, you suspect African Tick Bite Fever based on his signs and symptoms but you must definitively diagnose him. Unfortunately, there are several problems with diagnosing African Tick Bite Fever. First, as mentioned earlier, there are many different diseases that are caused by Rickettsiae bacteria and all of these diseases present very similarly. Most of these “spotted fevers” present with a fever, a rash, eschars, and enlarged lymph nodes. Therefore, your patient with these symptoms could have numerous diseases and a diagnosis cannot be made based upon clinical signs and symptoms. Second, spotted fever rickettsiae pathogens causes an immune reaction in humans that can be difficult to distinguish using antibody-based laboratory techniques. In other words, the antibodies made in the bodies of people to combat two different Rickettsiae bacteria look very similar and are hard to distinguish in a lab setting. Third, African Heaney 11 Tick Bite Fever is a febrile disease and has overlapping endemicity with Malaria in many African countries. So, as stated earlier, ATBF can be misdiagnosed as malaria. Although this challenge does not apply to your patient, it does pose problems in African countries. Overall, these difficulties show that diagnosis of African Tick Bite Fever is very difficult if the diagnostician is lacking necessary laboratory tools. Therefore, if there were to be an outbreak of African Tick Bite Fever in rural Africa, diagnosis would be a significant challenge. (Perry, 2004) Luckily, you are in France and have access to more advanced equipment than the doctors in Africa might have. The right equipment can provide easy identification of the R. africae or R. parkeri bacteria. Preferred diagnostic techniques for this disease utilize a swab or a skin biopsy from the patient’s rash or eschar. The easiest and most preferred method is the polymerase chain reaction (PCR) test. This test looks for the specific DNA sequence of the bacteria within the patient’s skin sample. Second, you can use immunohistochemical detection to identify the bacteria. This involves visualizing the presence of specific antibodies that can bind to antigens on the bacteria surface. If the antibodies appear, that means the bacteria are present in the sample. Lastly, bacterial culture can be used to try and isolate the bacteria from the skin sample. Clearly, all of these techniques require intensive lab procedures and expertise. We are therefore currently lacking an easy and inexpensive way to diagnose this disease (Mandell, 2011). For your patient, you use the PCR method to identify rickettsia africae bacteria in his body. (Brouqui et al, 1997) Once he is diagnosed, the patient is given doxycycline (200mg/day) for 10 days and he remained well at a follow up visit 3 Heaney 12 weeks later. This is the general treatment for African Tick Bite Fever and it is very effective. It is given for 3-14 days or until the patient’s fever has been gone for 48 hours (Mandell, 2011). As mentioned earlier, it appears as if African Tick Bite Fever is primarily a traveler’s disease at this time. Because this is the case, methods for preventing infection when traveling to an endemic country are emphasized in the literature. First, and most obviously, one should continuously check himself or herself for ticks throughout the day. The less time a tick is feeding, the lower the probability of infection. Second, specific lotions have been created that act as barriers on the skin to prevent ticks from inserting their hypostoma. These are called DEET and KBR lotions, and they have significant but short lasting effects against questing A. hebraeum ticks. According to one study, the lotions must be more than 20% DEET or KBR to be effective. They are 90% effective when first applied, but decrease to only 50% effective after two hours. Therefore, constant application is also necessary for full protection with these lotions (Jensenius, 2005). The literature does not seem to contain any instances of widespread outbreaks of African Tick Bite Fever, so large scale public health interventions were also scarce. However, there are a few techniques that can be used to control the disease and they all work to disrupt the tick lifecycle. As already discussed in the previous example of Lithuania after wartime, agricultural activities and deforestation can interrupt the tick life cycle. Both deforestation and increased agriculture lead to cutting down vegetation on which ticks could quest. If the grass that used to aid ticks in finding hosts is cut down, they will not be able to get blood Heaney 13 meals as easily and their life cycle will halt. Further more, ticks live in the soil when they are not connected to a host and agriculture changes the composition of soil. This can lead to a less hospitable environment for soil dwelling ticks. Insecticides are another possible method for controlling tick populations. One article cites that Amitraz and Decamethrin were successful in reducing tick populations, but the details are unclear about how much should be used and where these insecticides were tested. These chemicals are probably not the best option for vector control because they are known to have a negative effect on the environment. Some can be poisonous to other animals and plants. (Kazar, 1991) Another intervention that has proven effective is the use of tail tags on cattle. The Amblyomma ticks tend to feed on cattle, so the use of tail tags is directly preventing the infection of cattle with rickettsiae bacteria. However, ticks can become infected if they feed on an infected cow and this newly infected tick could then attach to a human and infect the human. Therefore, this intervention indirectly protects humans from infection because the ticks are biting cattle less frequently and thus the proportion of infected ticks is decreasing. The tail tags work by mimicking a secondary mechanism that Amblyomma ticks use to connect to their host. This species of tick sends out specific chemicals when it attaches to a host. Those chemicals serve as summoning signals to other ticks nearby, and that results in multiple ticks feeding in the same place. Scientists isolated those chemicals and put them onto the tail tags, which are clasped around the cattle’s tail. So, if a tick is nearby it will pick up the chemical signals being emitted from the tag and migrate towards it. Once the tick crawls on the tail tag, a chemical called ascaricide kills it. Heaney 14 Tests have shown that these tail tags have excellent (99%) efficacy in controlling A. hebraeum ticks on cattle in Zimbabwe (Norval, 1996). Overall, there has not been a lot of research or interest in large-scale interventions against African Tick Bite Fever, most likely because it has not proven to be a very dangerous disease. Also, as mentioned above, cheap and easy diagnostic tools are not available. Therefore, if an epidemic were to occur, pursuing these methods of vector control and creating better diagnostic tools would be extremely important for controlling the outbreak. Heaney 15 Works Cited Centers for Disease Control and Prevention; Ticks (2011) <www.cdc.gov/ticks 2011> Grouqui, Philippe (1997). African Tick-Bite Fever; An Imported Spotless Rickettsiosis. Arch Intern Med,157(1),119-124 Jensenius, Mogens (2005) Repellent efficacy of four commercial DEET lotions against Amblyomma hebraeum (Acari: Ixodidae), the principle vector of Rickettsia africae in southern Africa. Transactions of the Royal Society of Tropical Medicine, 99 (9), 708-711 Kazar, J. (1991) Control of Rickettsial Diseases. European Journal of Epidemiology, 7(3), 282-286 Ndip, Lucy (2004) Detection of Rickettsia Africae in patients and ticks along the coastal region of Cameroon. American Journal of Tropical Medicine and Hygiene, 71(3), 363-366 Mandell, GL (2011). Principles and Practice of Infectious Disease. Churchill Livingstone Elsevier: Philadelphia, PA Norval, R.A.I. (1996) Efficacy of pheromone-acaricide impregnated tail-tag decoys for controlling the bont tick, Amblyomma hebraeum (Acari: Ixodidae), on cattle in Zimbabwe. Experimental and Applied Acarology, 20, 31-46 Paddock, Christopher (2010). Through a glass, darkly: The global incidence of tickborne diseases. Draft background paper written to stimulate discussion for the Institute of Medicine Committee on Lyme Disease and OTher Tick-Borne Diseases: The State of the Science Parola, Philippe (2001).Ticks and Tickborne Bacterial Diseases in Humans: An emerging Infectious Threat. Clinical Infectious Diseases, 32 (6), 897-928 Parry, Eldryd (2004) Principles of Medicine in Africa. New York, NY: Cambridge University Press Robinson, Jennilee (2009) New Approaches to Detection and Identification of Rickettsia africae and Ehrlichia ruminantium in Amblyomma variegatum, (Acari: Ixodidae) Ticks from the Caribbean. Journal of Medical Entomology, 46 (4), 942-951 Sanson, Tracy (2011) Tick-Borne Diseases. <emedicine.medscape.com> Heaney 16 Vredevoe, Larisa. Tick Biology, University of California Davis. <http://entomology.ucdavis.edu/faculty/rbkimsey/tickbio.html>