A1. Methodological Appendix
advertisement

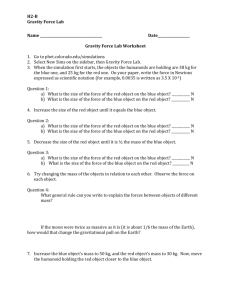
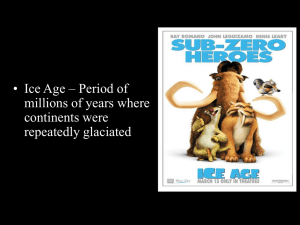
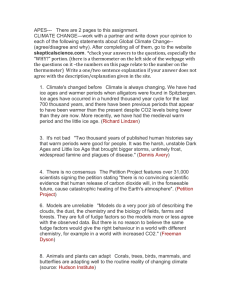
Supplementary Appendix to Health Reform and the Geography of the Primary Care Workforce A1. Methodological Appendix Comparison to Demand-Projection Models and Traditional Shortage Designation Methods The underlying trends affecting the primary care workforce (e.g., an aging population and coverage expansion under the ACA) are occurring simultaneously with shifts in technology, productivity, and delivery system reforms that seek to change practice patterns, redefine professional roles, and restructure provider reimbursement – all with the goal of stripping away volume-based utilization incentives in the fee-for-service (FFS) delivery system. Consequently, measures that rely on past utilization patterns as a proxy for future demand may provide an inaccurate assessment of needs moving forward. Similarly, population-to-provider ratios traditionally used to designate local workforce shortages do not include non-physician clinicians and are also based on historical physician supply data. For example, the primary designation threshold (3,000:1) used for primary care health professional shortage areas (PC-HPSAs) is based on the 75th percentile of 1974 population-to-provider ratio data. As summarized in a recent Institute of Medicine report, relying on demand-projection models and historical population-to-provider ratios is problematic because the underlying methodologies and assumptions of demand-projection models “have limited relevance to future health delivery systems.”1 These methodological limitations are only compounded by the additional assumption of traditional population-to-provider ratios that the only clinicians available to a given population are those located within the same jurisdictional boundaries (e.g., the county). For these reasons we sought to construct outcome measures of the geographic distribution of the primary care workforce that were not tied to historical utilization patterns or to historical population-to-provider thresholds, and that incorporated more realistic measures of local markets for primary care services. Specifically, our analytic strategy differed from other methods in three important ways. First, our designation methodology was based on relative cross-county comparisons based on the 2012 workforce, not historic population-to-provider thresholds. That is, we classified the bottom third of counties as “low accessibility” rather than use a specific cutoff threshold (e.g., 3,000:1). Second, as described in the text our overall workforce measure was based on registry data reported in the Area Health Resource File (AHRF) and included both physician and nonphysician clinicians including NPs, PAs and certified nurse midwives. Finally, as described below and in the text, our model did not impose a parametric assumption on patient travel, but rather incorporated local travel patterns non-parametrically based on travel flow data. 1 Jill Eden, Donald Berwick, Gail Wilensky. Graduate Medical Education That Meets the Nation’s Health Needs. 2014. 1 As a result of these differences, compared to traditional methodologies our measures will tend to show greater geographic accessibility in outlying areas adjacent to metro areas. This can be most readily seen in the figure below, which compares the distribution of the implied population-to-provider measures from our gravity model to the population-to-provider ratio for a given area. Because our model incorporates locally-observed travel patterns, it tends to even out wide distributions estimated using a simple population-to-provider formula. As expected, for rural areas with populations of similar size, these adjustments are greater in areas adjacent to metro areas. That is, this pattern reflects the fact that there is a greater extent of daily travel between those areas – and our model utilizes this information in assuming a greater extent of geographic accessibility to primary care clinicians in the metro areas. Specific methodological details on our compound gravity model and how it incorporates these travel patterns are provided in the sections below. Figure A1: Tot al Primary Care Clinicians – Dist ribut ion of Populat ion-t o-Provider Rat io Using Tradit ional Met hods (Red Line) and Travel-Weight ed Compound Gravity Score Model (Black Line), by Urban/ Rural Cat egory Not es: Out comes were generat ed using t radit ional county-based populat ion-t o-provider rat ios and a nonparamet ric compound gravity model applied t o Area Healt h Resource File (AHRF) and Census Bureau county t ravel dat a. 2 Unit of Measurement The county was our primary unit of analysis because our ability to incorporate local travel patterns into our estimates was limited to county-based travel data constructed by the Census Bureau. In addition, estimates on the uninsured were based on a Census Bureau model that combined detailed administrative and survey data to yield more accurate and reliable county insurance estimates. Consequently, any estimate on the uninsured below the county level would exhibit significant modeling uncertainty on an important dimension of our analyses (the number of uninsured people who may gain access to coverage under the ACA). Thus, while our county-based approach allowed us greater flexibility to incorporate more accurate information on patient travel and insurance coverage – particularly for rural counties -- a key limitation is that this approach may limit the utility of our measures for very large counties (e.g., Los Angeles county). FTE Adjustments Analyses of PCMD data focused on active office-based physicians with a listed specialty in family medicine, general practice, general internal medicine, pediatrics, obstetrics & gynecology and emergency medicine. We converted the AHRF’s total PCP measure to a full-time equivalent (FTE) basis using a local adjustment factor based on hours worked among physicians responding to the 2009-2011 American Community Survey. Specifically, we used self-reported labor force and weekly hours worked for physicians to tabulate the number of FTEs in each Public Use Microdata Area (single-county and contiguous-area groupings of roughly 100,000 people). We then mapped each county to its PUMA and applied the local FTE adjustment factor to workforce counts from the AHRF data. Following NRMC recommendations we included OB/GYNs at 0.25 FTE. Sensitivity analyses considered all PCMDs at 1.0 FTE (i.e., we used a total headcount measure with no adjustment for hours worked) and our main results and conclusions were similar under this change. Non-Parametric Compound Gravity Model Our outcome estimates are derived using a non-parametric gravity model. Gravity models allow for geographic accessibility estimates for a given area (e.g., county) that are based on a weighted sum of physician supply and population demand within a travel distance. In other words, model estimates are not restricted by jurisdictional boundaries (e.g., within county borders). Typically, gravity model weights are derived from parametric assumptions on patient travel preferences. These assumptions are fed into a travel decay function Wij=f(Distij) that defines the travel radius and, within that radius, the probability of seeing a clinician as a function of distance. For a given area i, the general form of the geographc accessibility (Ci) model is 3 Where sj is the supply of physicians in area j, D_j is the demand for physicians in area j, and Wij is the probability that a patient from area i visits a physician in area j. Patients for whom j=i are those who seek primary care services within the same county as their PCP. The demand facing physicians in each area j (Dj) is estimated as the population from area k in the catchment area multiplied by the share of the population from area k obtaining primary care services in area j. Wkj is the probability that a patient from area k obtains primary care services in area j: Simple Example Consider three counties near each other with population sizes A=10,000; B=20,000; and C=30,000, respectively. County A has 1 PCP, while county B has 4 and county C 20. Under traditional HRSA population-to-physician ratio criteria for defining a shortage area (population to provider ratio of 3,500:1 or greater), a simple ratio estimated for each county would reveal that counties A and B are shortage areas: county A has a ratio of 10,000:1 while B has a ratio of 5,500:1. population PCPs population.to.provider 1 10000 1 10000 2 20000 4 5000 3 30000 20 1500 In essence, these estimates are equivalent to fitting gravity model using a weight (W) matrix set to: A A 1 B 0 C 0 B 0 1 0 C 0 0 1 That is, patients are assumed only to obtain primary care services in their own county; the probability that patients obtain services outside of their own county (i.e., the value of the offdiagonal elements) is zero. 4 Parametric Travel Assumptions Estimates based on a simple county population-to-provider ratio may be misleading, however, because patients may cross county borders to visit a PCP. We can therefore define an alternative model that allows for patient travel if the travel time between population centers in each county is 25 minutes or less. Among those areas, travel probabilities decline according to an (assumed) exponential function. Suppose that counties B and C are less than 25 miles apart, but the distance between A and C, and A and B, is greater than 25 miles. We might summarize travel probabilities based on these parametric assumptions as: To extend the example from above, suppose that Distbc = 12 miles, and that counties A and B are greater than 25 miles apart. Applying this formula yields the following weight matrix A B C A 1 0.000 0.000 B 0 0.699 0.301 C 0 0.301 0.699 The gravity model in this case would yield an implied population to provider ratio for county B that is below the shortage cutoff of 3,500:1. This is achieved by distributing patients and PCPs more evenly across areas that are within the travel radius. That is, by assuming that patients in County B can access PCPs in county C, the implied ratio in county B declines while it increases slightly for county C. These results can be seen in the third column below: A B C population PCPs population.to.provider implied.pop.to.provider.25mi 10000 1 10000 10000 20000 4 5000 2901 30000 20 1500 1754 HPSA-PC designation criteria used by HRSA utilize a similar parametric assumption. For example, county population-to-provider estimates under the HRSA methodology are based on out-of-county PCPs in cases where the population centers between counties are less than 30 minutes travel time apart, and when primary care resources in an adjacent county are not already constrained. Non-Parametric Model Ideally, values of Wjk would not be based on strict parametric assumptions, but rather would be based on patient surveys on where people might obtain primary care services. Since such data 5 are not currently available in the U.S., our study utilized a proxy for patient travel based on observed county travel commuting patterns estimated in the American Community Survey (ACS) – the same data source as our underlying insurance and income data (the ACS is the primary data source for the Census Bureau’s Small Area Health Insurance Estimates Data). Specifically, the ACS asks detailed questions on employment and commuting behavior, and the Census Bureau uses this information to construct cross-county travel estimates for each area in the U.S. We obtained these estimates from the Census Bureau and used them to construct a nonparametric proxy for local travel patterns. The underlying idea in using travel flow data as weights (Wjk and Wij) is that county travel patterns can provide a better relative approximation to patient travel preferences when compared to the standard parametric approach, or to a simple approach based only on comparing supply and demand within each county. To extend the example from above, suppose that when translated into travel probabilities these Census travel patterns take the following matrix form: A B C A 0.50 0.10 0.4 B 0.05 0.70 0.3 C 0.05 0.05 0.9 A key advantage of using observed local travel patterns is that the travel probabilities are not a strict function of distance; this model allows for off-diagonal travel probabilities that are not equal, as they are in a purely distance-based parametric model. In this way, for example, a large share of residents of a rural county adjacent to an urban county could be modeled as seeking primary care in the urban county, while the model would also not assume the same probability of seeing care in the rural county for residents of the urban county (as would be the case in a pure distance-based equation, since the distances are equal in each case). By applying the gravity model formula we end up with an implied population-to-provider ratio that distributes patients to nearby counties according to local travel patterns. As can be seen below, the resulting estimates indicate that no county is below the standard 3,500:1 ratio that designates a shortage area. 1 2 3 population PCPs population.to.provider implied.pop.to.provider 10000 1 10000 3256 20000 4 5000 2954 30000 20 1500 1979 Example Using ACS Data Autauga county, Alabama is a county near the metropolitan area of Montgomery; it is also the first county listed alphabetically in the United States. It also provides a nice real-world example 6 of how our non-parametric gravity model can be applied to construct estimates of local workforce capacity. The figure below uses county PCP and population data to construct a population-to provider ratio for three counties including Autauga. As can be seen by the color shadings, a simple population-to-provider ratio estimated separately for each county would reveal that Autauga county (upper left) and neighboring Elmore county (Upper Right) have potential capacity gaps. eFigure 1: Population-to-PCP Ratios and County Travel Flows, Autauga, AL and Vicinity The figure also overlays county commuting data from the ACS, showing that roughly half of the county populations of Autauga and nearby Elmore county commute daily into Montgomery county for work. Conversely, about 2 percent of the Montgomery county population works in Autauga and Elmore counties. We can use these travel patterns to construct a matrix of travel probabilities, and feed these travel probabilities through the gravity model to “smooth” out patient travel across local areas. The results of applying the non-parametric, travel-adjusted gravity model are displayed in eFigure2 below. 7 eFigure 2: Implied Population-to-PCP Ratio After Applying Gravity Model, Autauga, AL and Vicinity 8 A2. Supplemental Tables and Figures 9 Figure A2: Geographically Accessible Primary Care Nurse Pract it ioners per 100k Populat ion, by Urban/ Rural Cat egory and St at e Scope of Pract ice Environment Not es: Est imat es reflect unadjust ed means of geographically accessible primary care nurse pract it ioners (PCNPs), overall and by rural/ urban cont inuum code cat egory, and by st at e scope of pract ice cat egory. All out comes were fit using a non-paramet ric compound gravity model applied t o Area Healt h Resource File (AHRF) and Census Bureau county t ravel dat a. Full Pract ice St at es: AK ,AZ,CO,DC,HI,IA,ID,ME,MT ,ND,NH,NM,NV,OR,RI,VT ,WA,WY Reduced Pract ice St at es: AL,AR,CT ,DE,IL,IN,K S,K Y,LA,MD,MN,MS,NE,NJ,NY,OH,PA,SD,UT ,WI,WV Rest rict ed Pract ice St at es: CA,FL,GA,MA,MI,MO,NC,OK ,SC,T N,T X,VA 10 Figure A3: Geographically Accessible Primary Care Physicians per 100k Populat ion, by Urban/ Rural Cat egory and St at e Scope of Pract ice Environment Not es: Est imat es reflect unadjust ed means of geographically accessible primary care physicians (PCMDs), overall and by rural/ urban cont inuum code cat egory, and by st at e scope of pract ice cat egory. All out comes were fit using a non-paramet ric compound gravity model applied t o Area Healt h Resource File (AHRF) and Census Bureau county t ravel dat a. Full Pract ice St at es: AK ,AZ,CO,DC,HI,IA,ID,ME,MT ,ND,NH,NM,NV,OR,RI,VT ,WA,WY Reduced Pract ice St at es: AL,AR,CT ,DE,IL,IN,K S,K Y,LA,MD,MN,MS,NE,NJ,NY,OH,PA,SD,UT ,WI,WV Rest rict ed Pract ice St at es: CA,FL,GA,MA,MI,MO,NC,OK ,SC,T N,T X,VA 11 Figure A4: Geographically Accessible Primary Care Physician Assist ant s per 100k Populat ion, by Urban/ Rural Cat egory and St at e Scope of Pract ice Environment Not es: Est imat es reflect unadjust ed means of geographically accessible primary care physician assist ant s (PCPAs), overall and by rural/ urban cont inuum code cat egory, and by st at e scope of pract ice cat egory. All out comes were fit using a non-paramet ric compound gravity model applied t o Area Healt h Resource File (AHRF) and Census Bureau county t ravel dat a. Full Pract ice St at es: AK ,AZ,CO,DC,HI,IA,ID,ME,MT ,ND,NH,NM,NV,OR,RI,VT ,WA,WY Reduced Pract ice St at es: AL,AR,CT ,DE,IL,IN,K S,K Y,LA,MD,MN,MS,NE,NJ,NY,OH,PA,SD,UT ,WI,WV Rest rict ed Pract ice St at es: CA,FL,GA,MA,MI,MO,NC,OK ,SC,T N,T X,VA 12 Figure A5: Adjust ed Di↵erences in Geographic Accessibility of Primary Care Physicians, by Urban/ Rural Cat egory and St at e NP Scope of Pract ice Environment Not es: Est imat es reflect adjust ed di↵erences in t he geographic accessibility of primary care physicians (PCMDs) per 100k populat ion by urban/ rural cat egory and st at e scope of pract ice environment . T he reference cat egory for comparisons wit hin each rural/ urban cat egory is Full Pract ice St at es. All out comes were generat ed using a non-paramet ric compound gravity model applied t o Area Healt h Resource File (AHRF) and Census Bureau county t ravel dat a. Gravity model out comes were fit using a negat ive binomial model wit h county-level cont rols for populat ion size, income & poverty, educat ional st at us, race/ et hnicity, gender, and unemployment . T he reference cat egory for each di↵erence comparison is count ies wit h t he same urban/ rural classificat ion in st at es wit h full scope of pract ice for NPs. Shaded point s indicat e t hat t he est imat e is st at ist ically significant from 0 ( ↵ = 0.05). Full Pract ice St at es: AK ,AZ,CO,DC,HI,IA,ID,ME,MT ,ND,NH,NM,NV,OR,RI,VT ,WA,WY Reduced Pract ice St at es: AL,AR,CT ,DE,IL,IN,K S,K Y,LA,MD,MN,MS,NE,NJ,NY,OH,PA,SD,UT ,WI,WV Rest rict ed Pract ice St at es: CA,FL,GA,MA,MI,MO,NC,OK ,SC,T N,T X,VA 13 Figure A6: Adjust ed Di↵erences in Geographic Accessibility of Primary Care Physician Assist ant s, by Urban/ Rural Cat egory and St at e NP Scope of Pract ice Environment Not es: Est imat es reflect adjust ed di↵erences in t he geographic accessibility of primary physician assist ant s (Pas) per 100k populat ion by urban/ rural cat egory and st at e scope of pract ice environment . All out comes were generat ed using a non-paramet ric compound gravity model applied t o Area Healt h Resource File (AHRF) and Census Bureau county t ravel dat a. Gravity model out comes were fit using a negat ive binomial model wit h county-level cont rols for populat ion size, income & poverty, educat ional st at us, race/ et hnicity, gender, and unemployment . T he reference cat egory for each di↵erence comparison is count ies wit h t he same urban/ rural classificat ion in st at es wit h full scope of pract ice for NPs. Shaded point s indicat e t hat t he est imat e is st at ist ically significant from 0 ( ↵ = 0.05). Full Pract ice St at es: AK ,AZ,CO,DC,HI,IA,ID,ME,MT ,ND,NH,NM,NV,OR,RI,VT ,WA,WY Reduced Pract ice St at es: AL,AR,CT ,DE,IL,IN,K S,K Y,LA,MD,MN,MS,NE,NJ,NY,OH,PA,SD,UT ,WI,WV Rest rict ed Pract ice St at es: CA,FL,GA,MA,MI,MO,NC,OK ,SC,T N,T X,VA 14 Figure A7: Percent age of Nurse Pract it ioners in Primary Care and Non-Primary Care Set t ings, by Urban/ Rural Cat egory Not es: Est imat es reflect t he percent age of all geographically accessible nurse pract it ioners who are in primary care set t ings vs. non primary care set t ings. All out comes were generat ed using a non-paramet ric compound gravity model applied t o Area Healt h Resource File (AHRF) and Census Bureau county t ravel dat a. 15 Figure A8: Percent age of Nurse Pract it ioners in Primary Care and Non-Primary Care Set t ings, by St at e Scope of Pract ice Environment and Urban/ Rural Cat egory Not es: Est imat es reflect t he percent age of all geographically accessible nurse pract it ioners who are in primary care set t ings vs. non primary care set t ings. All out comes were generat ed using a non-paramet ric compound gravity model applied t o Area Healt h Resource File (AHRF) and Census Bureau county t ravel dat a. Full Pract ice St at es: AK ,AZ,CO,DC,HI,IA,ID,ME,MT ,ND,NH,NM,NV,OR,RI,VT ,WA,WY Reduced Pract ice St at es: AL,AR,CT ,DE,IL,IN,K S,K Y,LA,MD,MN,MS,NE,NJ,NY,OH,PA,SD,UT ,WI,WV Rest rict ed Pract ice St at es: CA,FL,GA,MA,MI,MO,NC,OK ,SC,T N,T X,VA 16