Dear Registered Instructor Workshop Host Site,
advertisement

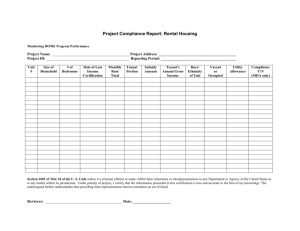
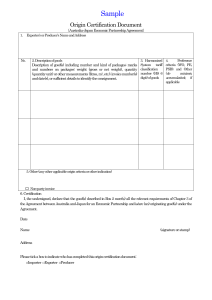
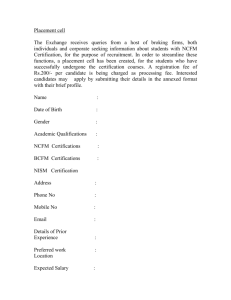
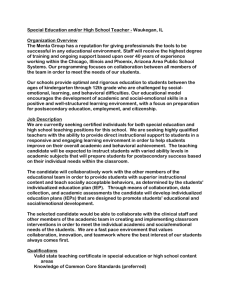
[Type text] Dream Catchers at the Cori Sikich Therapeutic Riding Center 10120 Fire Tower Road Toano, VA 23168 hjolly@dreamcatcherswilliamsburg.org www.dreamcatcherswilliamsburg.org Dear OSWC Participant: Thank you for your interest in attending the PATH INTERNATIONAL On-Site Workshop and/or Certification for Registered Level Instructors from June 24 - 27, 2013, at Dream Catchers. We are pleased to offer the certification to 10 participants, and the workshop for up to 20 participants. Enclosed is the PATH INTERNATIONAL Phase Two packet along with paperwork needed for our center in order for you to participate either as a workshop participant and/or a certification candidate. Please return all enclosed paperwork, along with copies of your PATH INTERNATIONAL membership card, Instructor-inTraining letter, and your payment by check made payable to Dream Catchers ($450 for workshop only/$350 for certification only or both for $700 or an audit fee for the workshop of $125) no later than May 15, 2013. However, please note that we will accept registrations from only 10 certification candidates and 20 workshop participants, and after all spaces have been taken will maintain a waiting list. If you should cancel your participation between May 16 and June 10, 2013, all but $100 to cover administrative costs will be refunded. There will be no refunds issued after June 10, 2013. Upon receipt of your payment and all completed forms and materials, you will receive a confirmation letter with more details about the schedule during the workshop and certification. If you are in need of lodging during your stay in Williamsburg, we will be happy to provide you with a list of local hotels that are convenient to Dream Catchers. If you have any questions, concerns or special needs, please do not hesitate to contact us at 757-566-1775 or at hjolly@dreamcatcherswilliamsburg.org We hope to see you soon! Sincerely, Harriet Jolly Office Manager Packet #2 1/10 -1- [Type text] Phase Two Packet Candidate Forms Packet #2 1/10 -2- [Type text] Welcome Candidate! Welcome to the PATH International Registered Instructor On-Site Certification Program! We applaud your commitment to gaining professional certification through this method of testing. Please make sure that you have previously completed Phase One of the PATH International Certification process prior to proceeding to the certification. All components of Phase One and Phase Two will need to be successfully completed before you can complete the certification. Purpose of Certification The purpose of this certification is to determine if the candidates possess adequate prior experience and sufficient skills to meet the criteria that are delineated for the PATH INTERNATIONAL Registered Instructor Program. Please refer to the PATH INTERNATIONAL Registered Instructor Application booklet for a listing of all criteria. During the certification process you will be evaluated on your horsemanship and teaching ability. While the On-Site process is an effective certification method, this can also be a stressful experience. The following is designed to provide information to help you arrive properly prepared to succeed and make this a positive experience. Workshop Portion Throughout the workshop you will be provided with invaluable insight and teaching strategies from experienced professionals. The workshop will also include hands-on activities including role playing and demonstrations on proper mounting and dismounting. However, the workshop portion serves as an educational review of the criteria, but cannot and does not provide the sole education necessary to pass the certification. You are required to bring those materials indicated in the on-line Instructor Self-Study: 1) posture & alignment photo; 2) a sample lesson plan. Being Physically Prepared Remember that both the teaching and the riding segments require physical preparedness to complete. If you have any concerns regarding your ability to pass any component of the certification, based on physical or mental limitations due to disability, injury or medical condition, contact the Host Site representative or the PATH INTERNATIONAL office for an Accommodation. See Instructor Certification Process for Exception to Application Requirements. The Horsemanship Component of Certification The riding test will be done after the workshop is complete. The Host Site and the evaluators will decide the scheduling of this portion. It will either be at the conclusion of the second day of the workshop or on the morning of the certification day. Candidates will be assigned horses that meet their riding style and requirements. If candidates have specific horse needs, they should inform the Host Site representative prior to the riding portion. Candidates will assist in the grooming and tacking of their mounts. Candidates will be evaluated on both the warm-up and the riding pattern. The Lesson Component of Certification Lessons will be randomly assigned and will be scheduled at ½-hour intervals. The Host Site will provide each candidate with detailed Rider Profiles for two students the evening prior to the certification lessons. The Lesson Plan should be developed based on the information provided in the Rider Profiles. Candidates will need to provide a Lesson Plan to the evaluators prior to the beginning of the lesson. Each lesson will be 20 minutes long. This must include mounts, lesson content to include teaching an equestrian skill and dismounts. Candidates are responsible for ensuring that their horses, volunteers and arena are set up for the class. The Host Site representative will identify volunteer needs. Candidates are responsible for checking with the Host Site representative to determine how these needs will be met and to determine which equipment each rider typically uses. Every effort has been made by the Host Site to provide suitable riders, volunteers and horses; however, as in any therapeutic riding program, there exists the possibility of last minute substitutions. In the event that a substitution is made, the Host Site representative will provide the candidate with information specific to the change. At the conclusion of the lesson, the candidate will need to complete the evaluation portion of the Lesson Plan and return it to the evaluators. Evaluation of Candidates Following the completion of the lesson component, the evaluators will meet to complete written reports on each candidate. This process takes several hours to complete. Be prepared to stay late or to meet the following day for your performance review. Individual evaluation sessions will be scheduled at 15-minute intervals to review results with each candidate. Remember that all evaluations will be based on the criteria outlined for the PATH INTERNATIONAL Registered Instructor Certification Program. Thank you for participating in the PATH International Instructor Workshop and/or On-Site Registered Certification. Good luck and enjoy! Packet #2 1/10 -3- [Type text] PATH Int’l. Instructor Workshop and/or On-Site Registered Certification Phase Two Workshop and/or Certification Form Name: ______________________________________________________________________________________________________ Address: ____________________________________________________________________________________________________ Phone: Daytime: ( Fax: ( ) ___________________ Evening: ( ) _____________________ Cell: ( ) __________________________ ) _______________________ Email: _______________________________________________________________ Workshop and/or Certification dates: _________________________ Location: ____________________________________________ Please register me for the following: Workshop only ($450) Certification only($350) Both - Workshop & Certification ($700) If you are participating in the Certification component, complete the following for the purposes of horse and tack selection. For the riding demonstration portion of certification, please indicate the following: Preferred seat: English Western Height:___________ Weight: ___________ All participants of the Workshop and/or Certification must be PATH INTERNATIONAL Individual Members. Please use the forms provided. Incomplete Phase Two packets will not be accepted. To be completed by all participants: I am a current PATH INT’L Individual member and have included a copy of my card. Membership # (required) ____________ I am not a current PATH INT’L Individual member and I have enclosed the $45.00 membership fee payable to PATH INT’L. I have enclosed my signed and dated PATH INT’L Liability Release and Emergency Medical Treatment Form. I am taking the workshop only and have enclosed the workshop fee of $450 (if applicable) I am enclosing the combined registration fee of $ 700 for both workshop and certification. (if applicable) I am auditing the workshop and am enclosing the audit fee of $ 125 (if applicable). To be completed only by candidates applying for certification: I am participating in the certification only and I have enclosed the Registered Instructor On-Site-Certification fee of ________. I am at least 18 years of age. I have enclosed copies of my current CPR and First Aid certification. I have completed Phase One of the Certification process through the PATH INTERNATIONAL office. I have enclosed a copy of the Confirmation of Instructor-In-Training status letter from the PATH INTERNATIONAL office verifying my successful completion of Phase One. I have applied for an exemption or accommodation through the PATH INTERNATIONAL office and have enclosed a copy of the letter. I have enclosed the Documentation of Group Mounted Teaching Hours form. I have enclosed this Registration form. I have enclosed the Resume form. I have enclosed the Personal Reference form. I have enclosed the Professional Reference form. I have enclosed the Essay Questions form. I have completed a PATH INTERNATIONAL On-Site Workshop, or I will be attending the workshop scheduled with this certification. If a PATH INTERNATIONAL On-Site Workshop was previously attended, please indicate the date and location:________________________ and include a copy of your Certificate. I understand that prior to the Workshop and/or Certification I will make a copy of all application materials to keep for my records. I understand that all components of the Certification process need to be completed before I can attend the certification. Make Workshop and/or Certification checks payable to: Dream Catchers Send to: Dream Catchers, 10120 Fire Tower Road, Toano, VA 23168 Certification Registration Deadline: May 15, 2013 Completed Phase Two Packet Deadline: June 7, 2013 All application materials will be kept confidential and used for no other purposes than that required for PATH INT’L Instructor Certification. Packet #2 1/10 -4- [Type text] PATH INT’L Instructor Workshop and/or On-Site Registered Certification Applicant Riding Demonstration In order to successfully pass this segment, all candidates must wear an ASTM/SEI approved helmet. Candidates will be required to demonstrate their own riding ability by riding the following pattern, which includes: - Warm-up - Circle - Ride at a walk, trot (jog), and canter (lope) both directions of the arena - Back - Change the rein through the diagonal - Halt After a brief warm-up, execute the following pattern to demonstrate your riding skills: Packet #2 1/10 -5- [Type text] PATH INT’L Instructor Workshop and/or On-Site Registered Certification Riding Instructor Resume Name: ______________________________________________________ Phone: _________________________ Address: ____________________________________________________________________________________ City: ______________________________________________ State: _______________ Zip: ________________ Are you a licensed therapist? PT OT Other Therapist: ________________________________ Are you a PATH INTERNATIONAL Individual member: Yes No If affiliated with an operating center, list name: _____________________________________________________ EDUCATION High School: _______________________________________ Year: ________ Diploma: __________________ College or Vocational: _______________________________ Year: ________ Diploma: __________________ Other Studies/Certificates/License: ____________________________________ Year: _____________________ Work Experience related to disabilities (other than therapeutic riding): ___________________________________ ___________________________________________________________________________________________ EQUESTRIAN BACKGROUND Number of years riding: ________ Owning a horse: ________ Number of years giving riding instruction: ________ Type of instruction: _________________ Pony Club level: ______________ 4-H level: ____________________ Your equestrian experience: ____________________________________________________________________ ___________________________________________________________________________________________ EXPERIENCE TEACHING RIDERS WITH DISABILITIES Do you work with any of the following disabilities? Check all that apply. Mental Impairments Cerebral Palsy Learning Disabilities Multiple Sclerosis Communication Impairment Muscular Dystrophy Hearing Impairments Brain Injury/Head Trauma Visual Impairments Spina Bifida Emotional Impairments Stroke/CVA Autism Post-Polio Down Syndrome Other ____________________ ADDITIONAL INFORMATION Professional organizations of which you are a member:_______________________________________________ ___________________________________________________________________________________________ Articles/books/lectures you have done:____________________________________________________________ ___________________________________________________________________________________________ Signature: __________________________________________________________________________________ Title: __________________________________________________ Date: _____________________________ Packet #2 1/10 -6- [Type text] PATH INT’L Instructor Workshop and/or On-Site Registered Certification Personal Reference (This reference cannot be the same as the Professional Reference.) Instructor Certification Candidate’s Name: _______________________________________________________ Name of Reference: __________________________________________________________ Age: __________ Address: _________________________________________________________________________________ City: __________________________________________________ State: _________ Zip: _______________ Phone: Day: ___________________________________ Evening: ________________________________ In what capacity does the reference know the candidate? Evaluate the candidate’s knowledge of horses and horsemanship: Evaluate the candidate’s understanding of individuals with disabilities and riding: (Please attach extra sheets if necessary) Signature of Reference: _______________________________________________ Date: ____________ Packet #2 1/10 -7- [Type text] PATH INT’L Instructor Workshop and/or On-Site Registered Certification Professional Reference (This reference cannot be the same as the Personal Reference. This reference must be familiar with applicant’s riding instruction experience.) Instructor Certification Candidate’s Name: _______________________________________________________ Name of Reference: __________________________________________________________ Age: __________ Address: _________________________________________________________________________________ City: __________________________________________________ State: _________ Zip: _______________ Phone: Day: ___________________________________ Evening: ________________________________ In what capacity does the reference know the candidate? How many hours of lesson instruction has the applicant completed? Evaluate the candidate’s knowledge of horses and horsemanship: Evaluate the candidate’s understanding of individuals with disabilities and riding: (Please attach extra sheets if needed) Signature of Reference: _______________________________________________ Date: ____________ Packet #2 1/10 -8- [Type text] PATH INT’L Instructor Workshop and/or On-Site Registered Certification Essay Questions In your own words, answer the following questions. You may use this page or answer on a separate sheet of paper. Typed answers are suggested, as they are the easiest to read. Instructor Certification Candidate’s Name: _______________________________________________________ 1. Indicate which style of riding you teach: _____Balance Seat _____Forward Seat _____Dressage _____Western _____ Other: ______________________________________________________ Explain why you teach the style of riding indicated and what the benefits are for your riders. 2. Discuss your philosophy of teaching: 3. Describe your strengths as a therapeutic riding instructor: 4. Describe your opportunities for improvement as a therapeutic riding instructor: Packet #2 1/10 -9- [Type text] PATH INT’L Instructor Workshop and/or On-Site Registered Certification Documentation of Mounted Group Lesson Teaching Hours Name of Candidate: _________________________________________________________________________________ Address: __________________________________________________________________________________________ City: __________________________________________________State:_______________Zip:____________________ Phone: Day: (__ ) ______ Evening: (____)_______________ Email: _______________________________________ Date Location/Organization Discipline Hours Mentor’s NAME & PATH INTL ID# Comments Please note: This form is not valid without the Mentor’s PATH INT’L ID # Total Hours: ________ Documentation of 25 hours teaching mounted group lessons to riders with disabilities. I do hereby affirm that that this information recorded above is accurate and factual. Candidate Signature: ______________________________________________________________ Date: ____________________ Please submit this form to the Host Site with your Phase Two packet. Packet #2 1/10 - 10 [Type text] Registered Instructor On-Site Workshop and/or Certification Authorization for Emergency Medical Treatment Form In the event emergency medical aid/treatment is required due to illness or injury during the process of participating in the PATH INTERNATIONAL Instructor Workshop and/or On-Site Registered Certification Program, or while being on the property of the hosting PATH INTERNATIONAL Center, I authorize the PATH INTERNATIONAL Registered On-Site Faculty/Evaluators to: 1. Secure and retain medical treatment and transportation if needed. 2. Release participant records upon request to the authorized individual or agency involved in the medical emergency treatment. Participant’s Name: _______________________________________________________________ Address: _______________________________________________________________ City/State/Zip: _______________________________________________________________ In the event that I cannot be reached, please contact: Name: ____________________________ Phone: ________________ Relationship: __________ Name: ____________________________ Phone: ________________ Relationship: __________ Physician’s Name: ____________________________________Phone:_____________________ Preferred Medical Facility: ________________________________________________________ Health Insurance Company: ___________________________ Policy #:____________________ Consent Plan This authorization includes x-ray, surgery, hospitalization, medication and any procedure deemed “life saving” by the physician. This provision will only be invoked if the person listed below is unable to be reached. Consent Signature: ____________________________________________ Date: ___________________ (Participant, Parent or Guardian) Print Name: _____________________________________________ Phone: ______________________ Address: ____________________________________________________________________________ Non-Consent Plan I do not give my permission for emergency medical treatment/aid in the case of illness or injury during the process of participating in the PATH INTERNATIONAL Registered On-Site Certification process or while being on the property of the hosting PATH INTERNATIONAL Center. In the event emergency treatment/aid is required, I wish the following procedures to take place: __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ Consent Signature: ____________________________________________ Date: __________________ (Participant, Parent or Guardian) Print Name: ____________________________________________ Phone: ______________________ Address: ____________________________________________________________________________ Packet #2 1/10 - 11 [Type text] PATH INT’L Instructor Workshop and/or On-Site Registered Certification Liability Release Form I, __________________________________________________, would like to participate in the PATH INT’L (Candidate’s Name) Instructor Workshop and/or On-Site Registered Certification. I acknowledge the risks and potential for risks of horseback riding. However, I feel that the possible benefits to me are greater than the risks assumed. I hereby, intending to be legally bound, for myself, my heirs and assigns, executors or administrators, waive and release forever all claims for damages against PATH INTERNATIONAL, it’s Board of Trustees, employees and Faculty/Evaluators for any and all injuries and/or losses I may sustain while participating in the PATH INTERNATIONAL Instructor Workshop and/or On-Site Registered Certification. Signature: _____________________________________________ Date: _____________ (Candidate) Many disabilities or injuries have accompanying conditions that pose special physical risks during exercise. Horseback riding is exercise, as are other activities involved in this Workshop and/or Certification, such as handling and working around horses. I understand that PATH INTERNATIONAL and the Host Site recommends that I seek the advice of a physician before participating in activities that involve exercise, riding, handling or being near horses. I understand that if I have a disability/disabilities, injury or physical condition that might affect my ability to ride, handle, or be around horses at the PATH INTERNATIONAL Instructor Workshop and/or On-Site Registered Certification, I will need to apply for an exemption or accommodation as outlined in the Accommodation or Exemption Policy. Signature: _____________________________________________ Date: _____________ (Candidate) Packet #2 1/10 - 12 [Type text] 10120 Fire Tower Road Toano, VA 23168 757-566-1775 OSWC Participant Information and Release Name: Date: Address: Day Phone: City: Zip:___________ DOB:_____________________ In case of emergency, please contact: Name: Phone: Relationship: _______ Dates of On-Site Workshop and/or Certification:_____________________________ Media Release Please check the appropriate box and sign below: I hereby (please check one): o Consent to and authorize the use and reproduction by Dream Catchers at the Cori Sikich Therapeutic Riding Center of any and all photographs and any other audio/visual media taken of me for promotional material, educational activities, exhibitions or for any other use for the benefit of the program. o Do not consent to above stated photo/media release. Signature: _______________________________________ Date: ____________________ Packet #2 1/10 - 13 [Type text] Dream Catchers Emergency Medical Consent Please check below the appropriate box and sign below: o I do hereby give consent to seek emergency medical attention in the event of a situation while on the premises or surrounding premises of Dream Catchers at the Cori Sikich Therapeutic Riding Center located in Toano, Virginia, where it is deemed necessary and prudent by the staff or volunteers of Dream Catchers to seek professional medical services. I expect my emergency contact to be notified in the event that emergency medical care is sought on my behalf. o I do not give permission to the staff and volunteers of Dream Catchers at the Cori Sikich Therapeutic Riding Center to seek emergency medical attention on my behalf. Instead, in the event of any emergency, I wish the following procedures to take place (please explain in detail): ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ Printed Name:______________________________________________________ Signature: _________________________________________________________ Date: _____________________________________________________________ Release, Waiver & Indemnity Agreement Desiring to utilize the premises known as the Cori Sikich Therapeutic Riding Center and the adjoining properties, I, as the undersigned, do hereby willingly enter into this Release, Waiver & Indemnity Agreement. I recognize that, under Virginia law, an equine activity sponsor or equine professional is not liable for an injury to or the death of an individual in equine activities resulting exclusively from the inherent risks of equine activities. I fully understand that the activity of mounting, riding, boarding, feeding, or even being near a horse, involves numerous dangers and risks of injury to said individual and I completely release the owner of the Premises, and DCTR and its officers, directors, volunteers, employees, or its agents from any and all liability for any and all injuries resulting from the Participant’s, Volunteer’s, or Staff’s engagement in the Programs offered by DCTR. I expressly agree that this Release, Waiver and Indemnity Agreement shall be governed and construed as being sufficient to satisfy the assumption of risk and waiver requirements necessary to relieve equine activity sponsors and equine professionals from liability under the Virginia Equine Activity Liability Act, Section 3.1-796.130, et.seq. of the Code of Virginia (the “Act”), and that the owners of the Premises, DCTR and its officers, directors, volunteers, employees, and agents are covered as equine activity sponsors and/or equine professionals by the provisions of this Act. This Release, Waiver, and Indemnity Agreement shall be governed and construed by the laws of the Commonwealth of Virginia, regardless of where any injury or loss shall occur. In the event that any portion of this Release, Waiver, and Indemnity Agreement shall be declared unenforceable, such declaration shall not affect the remaining terms of this document, which shall survive intact. Printed Name: _________________________________________________ Signature:_____________________________________________________ Date:_________________________________________________________ Packet #2 1/10 - 14 [Type text] Dream Catchers at the Cori Sikich Therapeutic Riding Center Confidentiality Policy for Participants, Volunteers, and Staff Maintaining confidentiality of medical and sensitive information is of utmost importance to Dream Catchers. Participants and their families, other participants, volunteers and staff have a right to privacy that gives them control over the dissemination of their medical or other sensitive information. Dream Catchers staff, volunteers, and participants will preserve this right of confidentiality for all individuals. Dream Catchers staff, volunteers, PATH INTERNATIONAL certification and workshop participants and activity participants will keep confidential all medical, social, referral, personal, and financial information regarding a person and his/her family unless express permission to share information is provided. Anyone who works or volunteers for, or provides services to, Dream Catchers is bound by this policy. Participants, their caregivers, and other family members must also preserve the confidentiality of other participants and/or their family members. This includes, but is not limited to, full, and part time staff, independent contractors, temporary employees, volunteers, participants, family members and caregivers, visitors, workshop and certification participants, and board members. In effect, this policy applies to anyone connected to Dream Catchers who could obtain medical/sensitive participant information accidentally or purposely. Disclosure of information to outside agencies or individuals requires the specific written consent of the participant or if the participant is under the age of 18 or is deemed incompetent to give authorization, then that participant’s parent, guardian or agent. As a participant in a PATH INTERNATIONAL On-Site Workshop and/or Certification, I hereby agree with the above stated written policy and agree to uphold its standards and regulations. _____________________________________ Signature of OSWC Participant Packet #2 1/10 __________________ Date - 15