C. Tyler_Ellis_cancors_abstract
advertisement

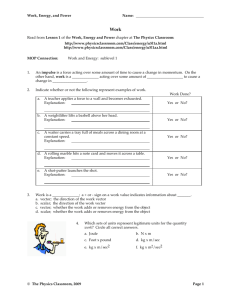
PATIENT-REPORTED ROLES, PREFERENCES, AND EXPECTATIONS REGARDING TREATMENT OF STAGE I RECTAL CANCER IN THE CANCER CARE OUTCOMES RESEARCH AND SURVEILLANCE CONSORTIUM (CANCORS) Authors: C. Tyler Ellis, MD, MSCR1, Mary E. Charlton, Ph.D2, Karyn B. Stitzenberg, MD, MPH3 1 Department of Surgery, University of North Carolina 2 Department of Epidemiology, University of Iowa College of Public Health, Iowa City, IA 3 Department of Surgical Oncology, Lineberger Comprehensive Cancer Center, University of North Carolina BACKGROUND: Historically, stage I rectal cancer was treated with total mesorectal excision (TME). However, there has been growing use of local excision (LE), with and without adjuvant therapy to treat these early rectal cancers. Little is known about how patients and providers choose amongst the various treatment approaches. OBJECTIVE: To identify patient roles, preferences and expectations as they relate to treatment decision-making for patients with stage I rectal cancer. DESIGN AND SETTINGS: Geographically diverse population and health-system based cohort study. PATIENTS: 154 adults with newly diagnosed and surgically treated stage I rectal cancer between 2003-2005. MAIN OUTCOME MEASURES: We compared patients by surgical treatment groups: (1) TME and (2) LE. Clinical, sociodemographic, and health-system factors were assessed for association with patient decision-making preferences and expectations. RESULTS: 80% of TME patients vs. 63% of LE patients expected that surgery would be curative, p=0.04. The TME group was less likely to report that radiation would cure their cancer compared to the LE group (27% vs 63%, p=0.004). When asked about preferred role in decision making, 28% of TME patients preferred patient-controlled decision making compared with 48% of LE patients, p=0.046. However, with regard to the treatment actually received, 38% of the TME group reported making their own surgical decision compared to 25% of the LE group, p=0.18 (Figure). CONCLUSIONS: Patients’ preferred decision-making role did not match the actual decision-making process. Future efforts should focus on bridging the gap between the decision-making process and patients’ preferences of various treatment approaches. This will be particularly important as newer innovative procedures play a more prominent role in the rectal cancer treatment paradigm. Figure. Patient Responses to Questions about Decision-Making Role Reported and Preferred by Patients. I. Patient Preferred Decision-Making Role 70% p-value 0.046 Response (%) 60% 50% 40% 30% 20% 10% 0% Preferred PatientControlled Decision Preferred Shared Decision-Making TME Preferred DoctorControlled Decision Don't Know LE II. Patient Reported Decision-Making Role 70% p-value 0.18 Response (%) 60% 50% 40% 30% 20% 10% 0% Patient-Controlled Decision Shared DecisionMaking TME Doctor-Controlled Decision Don't Know LE Shown are the responses of patients with stage I rectal cancer by surgical treatment type: total mesorectal excision (TME) or local excision (LE). Preferred role in the decision-making process reported by patients (Panel I). Actual role in the decision-making process reported by patients (Panel II).