Emergency Health Care Plan - South Plainfield Public Schools
advertisement

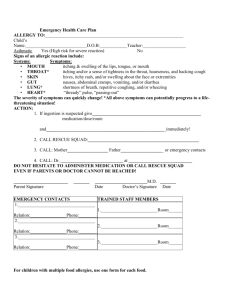
SOUTH PLAINFIELD BOARD OF EDUCATION South Plainfield, New Jersey 07080 Policy Picture Here Emergency Health Care Plan Life Threatening Allergies Allergy to: Student’s Name: DOB: Teacher: School Year: Signs of an allergic reaction include (previous reactions, if any): Systems Mouth Throat Skin Gut Lung Heart Symptoms itching and swelling of the lips, tongue or mouth itching and/or sense of tightness in the throat, hoarseness and hacking cough hives, itchy rash, and/or swelling about the face or extremities nausea, abdominal cramps, vomiting, and/or diarrhea shortness of breath, repetitive coughing, and/or wheezing “thready” pulse, “passing out” The severity of symptoms can quickly change. All above symptoms can potentially progress to a life-threatening situation! Action: 1. If ingestion or contact occurs, immediately give 2. Call 911 & request MICU. If MICU has not arrived within 15 minutes: 3. Repeat EPIPEN – YES or NO (circle one) 4. Call: Mother (name) H# C# Father (name) H# C# 5. Call: Doctor @ # (Med & dose) (Drs. Order) W# W# Preferred Hospital: DO NOT HESITATE TO ADMINISTER MEDICATION OR CALL RESCUE SQUAD Parent Signature Date Doctor Signature Date Nurse Signature Date School Doctor Signature Date Emergency Contact: 1. Name: Relation: 2. Name Relation: Trained Staff Members: 1. Room# 2. Room# Phone# Phone#