Rodney Castro Nursing 1100 (Lab) September 23, 2010 Jarvis
advertisement
 September 23, 2010 Jarvis")
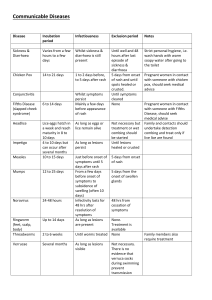
Rodney Castro Nursing 1100 (Lab) September 23, 2010 Jarvis, Physical examination and health assessment 2009 Chapter 12: pg 242 – 268 Skin Abnormalities Adolescents Increase in sebaceous gland activity creates increased oiliness and acne Acne lesions usually appear on face, back, chest, and shoulders May appear in children (7-8 years old) Peaks at 14-16 (girls) and 16-19 (boys) Pregnant Female Striae are stretch marks (silver/pink colour), appears in second trimester on abdomen, breast, thighs, which fades after deliver but not disappears Linea nigra is a brownish black line down the midline of abdomen Chloasma is an irregular brown patch of hyperpigmentation on the face, which occurs with pregnancy or ingesting contraceptive pills Vascular spiders have tiny red centers radiating branches and occur on neck face and chest Aging adult (skin colour and pigmentation) Senile lentinges (liver spots) are small flat brown macules that appear on forearms, and dorsa of hand. They are clusters of melanocytes that appear after extensive sun exposure Keratoses are thickened areas of pigmentation that look crusty and scaly, which develop on face and hands, unexposed/sun-exposed areas Moisture Dry skin is common in the aging person because of decline in size, number, and output of sweat glands and sebaceous glands Texture Common variations occurring in aging adults are acrochordons which are overgrowths of normal skin that form a stalk and are polyplike (eyelids, cheeks, and neck) Thickness With aging, skiin looks as thin as parchment and the subcutaneous fat diminishes Thin skin is in the dorsa of hands, forearms, lower legs, and dorsa of feet Skin is thicker over abdomen and chest Mobillity and Turgor Turgor is decreased (less elasticity) Hair Hair growth decreases with aging After menopause, woman develop hairs on upper chin In men, hairs develop in ears, nose, and eyebrows Nails Nail growth decreases, and local injuries in nail matrix may produce longitudinal ridges Toenails are thickened and may grow misshapen Table 12 – 2: Detecting Colour Changes in Light and Dark Skin *refer to pg 248 ~The following all have diagrams in 250-268~ Common shapes and configurations of lesions Annular Begins in the center and spreads to periphery Confluent Lesions run together Discrete Distinct, individual lesions that remain separate Grouped Clusters of lesions Gyrate Twisted, coiled spiral, snakelike Target Or iris, resembles iris of eye, concentric rings of colour in the lesions Linear A scratch, streak, line, or stripe Polycyclic Annular lesions grow together Zosteriform Linear arrangement along a nerve route Primary skin lesions Macule Solely a colour change, flat and circumscribed, of less that 1 cm (eg: freckles, measles) Papule Something you can feel caused by superficial thickening in epidermis (eg: mole, wart) Patch Macules larger than 1cm (eg: vitiligo, Mongolian spot) Plaque Papules coalesce to form surface elevation wider than 1 cm (eg: lichen planus) Nodule Solid, elevated, larger than 1 cm, extends into dermis (eg: fibroma, xanthoma) Wheal Superficial, raised, transient; irregular shape due to edema (eg: mosquito bite, allergic reaction) Tumour Larger than few cm in diameter, firm or soft, deeper in dermis (eg: lipoma, hemangioma Vesicle Elevated cavity containing free fluid, clear serum flows if ruptured (eg: herpes, shingles) Hives Wheals coalesce to form extensive reaction, intensely pruritic Bulla Single chambered, superficial in epidermis, ruptures easily (eg: friction blister, burns) Cyst Fluid filled cavity in dermis or subcutaneous layer (eg: sebaceous cyst, wen) Pustule Pus in the cavity (eg: acne, impetigo) Secondary skin lesions Debris on skin surface Crust Scale Thickened dried out exudates left when vesicles burst or dry up, coloured red-brown, honey, or yellow (eg: impetigo, scab after abrasion) Compact desiccated flakes of skin, dry or greasy from shedding of dead excess keratin cells (eg: seborrheic dermatitis, dry skin Break in continuity of surface Fissure linear crack with abrupt edges, extends into dermis, dry or moist (eg: athletes foot, cheilosis) Erosion scooped –out but shallow depression. Superficial; epidermis lost; moist but no bleeding, heals without scar because erosion does not extend into dermis Ulcer Deeper depression extending into dermis, irregular shape; may bleed; leaves scar when heals (eg: stasis ulcer, pressure sore) Excoriation Self-inflicted abrasion; superficial; sometimes crusted; scratches from intense itching (eg: insect bites, scabies) Scar After a skin lesion is repaired, normal tissue is lost and replaced with connective tissue (collagen) (eg: acne, healed area of surgery or injury) Atrophic scar Resulting skin level depressed with loss of tissue, thinning of epidermis (eg: striae) Lichenification Prolonged intense scratching eventually thickens the skin and produces tightly packed sets of papules; looks like surface of moss Keloid Hypertrophic scar, skin level is elevated by excess scar tissue, looks smooth rubbery Lesions caused by trauma or abuse Pattern injury Is a bruise or wound whose shape suggests the instrument or weapon caused it (eg: bite mark, pinch mark, belt buckle etc) Hematoma Is a bruise you can feel, elevates the skin and is seen as swelling Contusion (bruise) large patch of capillary bleeding into tissues a bruise usually occurs from trauma; also from bleeding disorders and liver dysfunction Vascular Lesions Hemangiomas Port-wine stain a large macular patch covering scalp or face, along distribution of cranial nerve V. Colour is dark red, bluish or purpleish and intensifies when crying present at birth and usually doesn’t fade strawberry mark (immature hemangioma) raised right area 2-3 cm in diameter consists of immature capillaries, present at birth, disappears ages 5-7 Cavernous hemangioma (mature) reddish blue, irregular shape, spongy mass of blood vessels Telangiectases Spider or star angioma fiery red star shape marking with solid center capillary radiations extend from the central arterial body develops on face, neck, or chest venous lake blue-purple dilatation of venules and capillaries in a star-shaped linear pattern pressure causes them to empty or disappear located in face lips, ears, and chest Purpuric Lesions Petechiae punctuate haemorrhages 1-3mm, round, dark, purple or brown caused by bleeding from superficial capillaries, may indicate abnormal clotting factors purpura confluent and extensive patch of petechiae and ecchymoses, red to purple, Seen in generalized disorders such as scurvy Common skin lesions in children Impetigo Moist, thin-roofed vesicles with thin erythematous base Contagious bacterial skin infection Common in children and infantrs Diaper dermatitis Red. Moist maculopopular patch with poorly defined borders in diaper area Inflammatory disease caused by skin irritation from ammoinia, heat, moisture, occlusive diapers Intertrigo Scalding red, moist patches, loose scales In genital area Aggravated by urine, feces, heat, and moisture Atopic dermatitis Erythematous papules and vesicles, with weeping, oozing, and crusts Occurs on scalp, forehead, cheeks, forearms, and wrists Measles Red-purple maculopopular blotchy rash appears on 3rd or 4th day of illness Rash appears first behind ears, and spreads over face, then neck, trunk, legs German measles Pink papular rash first appears on face then spreads Distinguished from measles by presence of neck lymphadenopathy and absnce of kopliks spots Chicken pox Small tight vesicles first appears on trunk, then to face, arms and legs. Vesicles erupt in succeeding crops overseveral days then become pustules then crusts Common skin lesions Primary contact dermatitis Local inflammatory reaction to an irritant in the environment or an allergy Erythema shows first, followed by swelling, wheals, scars Allergic drug reactions Erythematous and symmetrical rash Some drugs prude urticarial rash or vesicles Tinea corporis (ring worms of body) Scales on chest, abdomen, back of arms forming multiple circular lesions Tinea pedis (ringworms of foot) Fungul infection appears as small vesicles between toes, sides of feet soles Commonly found in warm moist feet (eg: after exercising in gym) Psoriasis Scaly erythematous patch, with silvery scales Located on scalp, outside of elbows and knees, low back, and anogenital area Tinea verisocolor Fine, scaling, round patches caused by superficial fungal infection Located on neck, trunk, upper arms, common in healthy young adults Labial herpes simplex (cold sore) Has a prodrome of skin tingling and sensitivity Lesions erupt with tight vesicles, then pustules, then acute gingiovostomatitis with ulcers Located in upper lip, and mouth and tongue Herpes zoster (shingles) Small grouped vesicles emerge along route of cutaneous senseory nerve, then pustules, then crusts Common on trunk, common more on adults older than 50 Erythema migrans of lyme disease Caused by spirochete bacterium carried by black or dark brown deer tick First stage has a red macular rash Rash radiates from the site of the tick bite with some central clearing and is usually located in axilla, or behind knee Rash fades in 4 weeks Malignant skin lesions Basal cell Usually starts as skin-coloured papulae, with a translucent top One of the most common forms of skin cancer Squamous cell carcinoma Erythematous scaly patch with sharp margins Usually on hands or head, areas exposed to solar radiation Malignant Brown, black, purple, tan coloured Arises from pre-existing nevi Common locations are on trunk, back in men and woman, legs on women Skin lesions associated with acquired immune deficiency syndrome Epidemic kaposi’s sarcoma: patch stage An aggressive form of kaposi’s sarcoma is one of the diseases that characterizes AIDS Epidemic kaposi’s sarcoma: plaque stage Evolving lesions develop into raised papules or thickened plaques Epidemic Kaposi’s sarcoma: advanced disease Advanced – stage, widely disseminated lesions involving skin, mucous membranes and visceral organs Infectious disease as a biological weapon Anthrax Cutaneous anthrax is caused by bacillus anthracis when it comes in contact with a pre-existing lesion or broken skin After 3 days, a red raised pruritic papulae appears followed by a round ulcer surrounding vesicles a few days later A tough black scab forms in a few weeks, which loosens and falls off in another few weeks Small pox Is a viral infection with no known treatment Disease is spread by direct contact or inhalation of respiratory droplets During incubation period 10-12 days, infected person will develop flu-like symptom (fever,headache,vomiting) Abrnomal conditions of hair Seborrheic dermatitis (cradle cap) Thick, yellow to white, greasy, adherent scales iwth mild erythema on scalp and forehead Common in early infancy Tinea Capitis (scalp ringworm) Rounded patchy hair loss on scalp, leaving broken-off hairs Caused by fungul infection; l Seen in children and farmers, highly contagious Toxic alopecia Patchy asymmetric balding Regrowth occurs after illness or discontinuation of toxin Alopecia areata Sudden appearance of sharply circumscribed round or oval balding patch When limited to a few patches, person usually has complete regrowth Traumatic alopecia: traction alopecia Linear or oval patch of hair loss along hairline; caused by trauma from hair rollers, tight braiding etc Trichotillomania Traumatic self-induced hair loss usually the result of compulsive twisting or plucking Pediculosis capitis (head lice) Causes intense itching of scalp Common among school age children Folliculitis Superficial infection with hair follicles Usually on arms, legs, face, and buttocks Hirsutism Excess body hair in females forming male sexual pattern (face, chest, upper lip etc) Caused by endocrine or metabolic dysfunction Furuncle and abscess Red, swollen hard, tender, pus-filled, lesion caused by acute localized bacterial infection Abnormal conditions of the nail Koilonchia Thin depressed nails with lateral edges tilted up, forming concave shape Paronchia Red swollen tender inflammation of nail folds Often a fungal infection Beau’s line Transverse furrow or groove, a depression across the nail that exends down to the nail bed Splinter haemorrhages Red-brown linear streaks with subacute bacterial endocarditis Late clubbing Proximal edge of nail elevates; angle is greater than 180 degrees Seen with chronic obstructive pulmonary diseases Onycholysis Slow persistent fungal infection of fingernails and more often toenails Fungus causes change in colour Pitting Sharply defined pitting and crumbling of the nails with distal detachment often occurs with psoriasis Habit-tic dystrophy Depression down middle of nail caused by continuous picking of cuticle