title of the case
advertisement

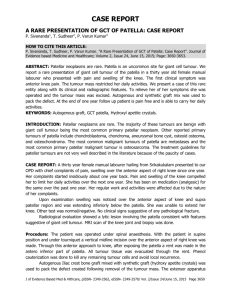
TITLE OF THE CASE “Giant cell tumour of the rib, a rare differential diagnosis of chest wall tumour” Authors of the case Dr Manoj Kumar Pattnaik Dr Paresh Chandra Majhi Dr Sameer Kumar Panigrahy Dr Anil Kumar Nayak Dr Ipsita Dhal Abstract A young adult male referred from a peripheral hospital with a painless swelling over anterolateral aspect of left lower chest wall. Initial evaluation revealed giant cell tumour (GCT) of rib & following surgical excision histopathological study confirmed the same. Giant Cell Tumor is a benign, slow growing tumor with some frankly malignant variant, commonly involve ends of long bones like lower end of femur ,upper end of tibia & lower end of radius after epiphyseal fusion in third and fourth decade with female preponderance [1-3]. On rare occasion it may involve the ribs to produce symptomatology, that of a chest wall tumour. Here we present a rare case of huge giant cell tumor of rib at its unusual location creating a well differential diagnosis of chest wall tumour. Background GCT of rib, arising from anterior arch with such a huge palpable swelling in an adult male is very unusual & sparsely reported [4-8].More commonly it arises from its posterior arch usually from the head and tubercle [8-11]. Whenever such a presentation faced, it is worthwhile to exclude common entities of chest wall tumor, and then managed accordingly. Case presentation A young adult male presented to our hospital with one year history of slow growing, painless, palpable, hard swelling over left lower chest wall, anterolaterally with no associated symptoms (figure-1, figure-2). Overlying skin was healthy with no local rise of temperature. Investigation All routine blood parameters were within normal limits except serum acid phosphatase (moderately elevated) which was done after Fine Needle Aspiration Cytology(FNAC). Cytosmears showed stromal cells in large fragments with good number of giant cells attached to periphery of fragments in the background of osteoclastic cells. Plain radiograph was not apparent (figure-3). Contrast enhanced Computed tomography showed heterogeneously enhancing mass arising from left 11th rib causing rib destruction with large soft tissue component showing central necrosis & few bony spicules, infiltrating the parietal abdominal muscle & abutting descending colon, left kidney, spleen and left psoas muscle (figure-4, figure-5).No lung pathology was detected. Differential Diagnosis Benign Lesions Fibrous dysplasia Enchondroma Eosinophilic granuloma Brown tumor Aneurysmal bone cyst Simple bone cyst Chondromyxoid fibroma Giant cell tumour Malignant Lesions Metastasis Solitary myeloma Chondrosarcoma Osteosarcoma Treatment Keeping in mind, the high recurrence of GCT, wide excision was done with involved portions of the parietal abdominal muscles. Peritoneal cavity was not entered, but left pleural cavity was opened due to diaphragm involvement (figure-6). Diphragm rent was closed with 2-0 polypropelene suture. Around one litre of intra operative blood loss was replenished by blood transfusion. Tumor mass was approximately 10x8x7cm in size with irregular greyish trabeculated friable tissue (figure-7). Histopathology showed biphagic pattern of both stromal cells & osteoclastic giant cells in isomorphic distribution with areas of hemorrhage & necrosis (figure-8, figure-9). Outcome & follow up Patient was uneventfully discharged on 10th post-operative day with no signs of recurrence after five months of follow up. He has not received any adjuvant therapy as the histopathology revealed no features of cellular atypia or mitotic activity. Serum acid phosphatase returned to base line on repeat evaluation. Discussion GCT of bone represent about 5% of all primary bone tumor. Scapula, sternum, patella, vertebra, skull, and talus have been reported as other rare sites [12]. Most of the cases are usually asymptomatic with mild pain or soft tissue swelling. Sometime it may present as pathological fracture due to thinning of cortical bone. Due to its rare incidence, GCT arising from the rib is difficult to diagnose, especially when the tumor is located in the anterior arc. Preoperatively FNAC can be used to enhance diagnostic certainty along with radiological survey. In current case, diagnosis was made by aspiration cytology preoperatively. Treatment of GCT may vary from simply curettage with or without use of alcohol, liquid nitrogen, phenol to wide excision with chest wall reconstruction [8- 11, 13]. However no standard treatment has been established for GCT of rib. The present case was subjected to liberal wide excision with primary reconstruction of diaphragm and chest wall. Literature reports high recurrence after surgical treatment, up to 50% [12].Though estrogen and progesterone receptors have been identified, role of steroid yet to be decided [14]. Role of radiotherapy was not much encouraged as malignant transformation in GCT has been reported with previous radiotherapy. Learning points As such cases have been reported and will be reported in future, we can never deny to put GCT among the differential diagnosis of chest wall tumour, at least when a bony hard and fixed mass stands out clearly in this age group even though its occurrence in rib is very unusual. Whenever a surgical excision is planned, wide excision to be done with expectation of healthy amount of blood loss as the tumour stroma is highly vascular. References 1. Dahlin DC. Giant cell tumor of bone: highlights of 407 cases. American Journal of Roentgenology.1985;144(5):955–960. [PubMed] 2. Sung HW, Kuo DP, Shu WP. Giant-cell tumor of bone: analysis of two hundred and eight cases in Chinese patients. Journal of Bone and Joint Surgery A. 1982;64(5):755–761. [PubMed] 3. Burgener FA, Kormano M. Differential Diagnosis in Conventional Radiology. 2nd edition. New York, NY, USA: Thieme Medical Publishers; 1991. 4. Briccoli A, Malaguti C, Iannetti C, et al. Giant cell tumor of the rib. Skeletal Radiology.2003;32(2):107–110. [PubMed] 5. Kumar A, Varshney MK, Trikha V, et al. An unusual presentation of a rare chest wall tumour: giant cell tumour of bone. Joint Bone Spine. 2007;74(1):100– 102. [PubMed] 6. Gupta V, Mittal R. Giant cell tumor of rib—rare location on the anterior aspect. Archives of Orthopaedic and Trauma Surgery. 2000;120(3-4):231– 232. [PubMed] 7. Reddy RHV, Queen S, Jilaihawi ANA, et al. Giant-cell tumour of the rib. European Journal of Cardio-thoracic Surgery. 2003;24(3):p. 450. [PubMed] 8. Shin JS, Lee IS, Kim A, et al. Giant cell tumor originating from the anterior arc of the rib. Journal of Korean Medical Science. 2002;17(6):849–851. [PMC free article] [PubMed] 9. Dehghan A, Moaddab AH, Eskandarlou M, et al. Anterior chest wall giant cell tumor. Gen Thorac Cardiovasc Surg. 2010;58:39–41. [PubMed] 10. Townsend CM, Beauchamp RD, Evers BM, et al. Sabiston textbook of surgery: the biological basis of modern surgical practice. 19th ed. Philadelphia (PA): Page 5 of 16 Page 6 of 7 Saunders; 2012. 11. Canale ST, Beaty JH. Campbell's operative orthopaedics. 12th ed. Philadelphia (PA): Mosby; 2013. 12. Fletcher C, Unni K, Mertens F, eds. Pathology and genetics of tumours of soft tissue and bone: International Agency for Research on Cancer. World Health Organization; 2002. 13. Chakarun CJ, Forrester DM, Gottsegen CJ, et al. Jr Giant cell tumor of bone: review, mimics, and new developments in treatment. Radiographics. 2013;33:197–211. [PubMed] 14. Vigorita VJ, Ghehman B, Mintz D, editors. Orthopaedic pathology. 2nd ed. Philadelphia: Lippincott Williams and Wilkins; 2008. pp. 280–9.