Full text - Dordt College Homepages
advertisement

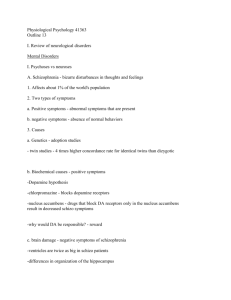
Risk Factors for Depression in College Students Abstract: Depression is an increasingly prevalent mental health issue, and most college students are at the age of first onset. This study utilized logistic regression to build a model for use in identification of depression in college students. In particular, it was determined that both sleep and exercise interact, with lower levels of each indicating greater risk for depression in this population. These findings are useful in identifying students at-risk for depression so that preventative services might be offered to such students. Background and Significance Depression is a mental illness that can be debilitating to those who experience it. In addition to psychological handicaps, depression can also affect a person’s cognitive ability and physical health. Between 5 and 8% of Americans suffer from depression each year; only half of those people are treated despite known treatments being substantially effective (Duckworth, 2013). Therefore, it is important to develop new ways to identify people at risk for depression and offer appropriate preventative treatment. Current research has shown that genetics, stress, marital status, and drug and alcohol use all play a role in depression (Haggerty, 2006). More recently, a European study of 12,395 adolescent students from 179 schools identified three additional factors that represent an invisible risk for depression: sedentary behavior, inadequate sleep, and high levels of technology use. Such behaviors are common among adolescents, yet often overlooked as risk factors for depression (Carli, 2014). As the average age of onset for depression is mid-20s it could be useful to apply these findings toward identification of depression in college students (Haggerty, 2006). The present study examines a sample of American college students with the goal of examining whether or not college students follow the pattern that low levels of sleep and exercise, as well as high levels of technology use, would result in an increased risk for depression. In addition, the study assesses age, gender, GPA, truancy, alcohol use, and cigarette use as potential covariates. Methods Data were collected using Sona, an online experiment management system (Sona Systems, 2002). Participants received partial course credit as compensation for participation in this study. They responded to an anonymous online survey which asked about various lifestyle habits and depression-related symptoms. The sample consisted of 165 students enrolled in at least one undergraduate psychology course at a mid-western university. The dependent variable for analysis was depression level as assessed by the Patient Health Questionnaire-9 (PHQ-9). The questionnaire consists of nine questions aimed at depression related systems. Respondents indicate (on a scale of 0 = “not at all” to 3 = “nearly every day”) how often they experience depression-related symptoms such as “Feeling down, depressed, or hopeless.” The total score for these nine items places a respondent in one of the following five categories: Minimal depression (0-4), mild depression (5-9), moderate depression (10-14), moderately severe depression (15-19), or severe depression (20-27) (Kroenke, 2001). For the purpose of this study, the scale was used to classify students as to whether or not they were at least moderately depressed (10-27). Since the goal of this research was to identify students who could be offered preventative services, this method served as a simple way to categorize students as either at-risk or not at-risk. The independent variables included three primary predictors: average hours of sleep per night, average hours of exercise per week, and average hours of technology use per day. Additionally, age, gender, GPA, major, number of classes missed per month, number of alcoholic beverages consumed per week, and number of cigarettes smoked per week were included as possible covariates. The binary variable indicating moderate or greater depression was analyzed using logistic regression. Backward elimination beginning with a model containing second order interactions was used to achieve the final model. The significance level for removal was 0.05. The variables considered for inclusion in the model were age, gender, GPA, missed classes, level of sleep, level of exercise, technology use, alcohol use, and cigarettes use. Odds ratio confidence intervals for significant terms are used to address the research questions described above. Additionally, the probability of depression for various predictor values was also estimated using the final model. All statistical analyses were conducted using Minitab and SAS software (Minitab, 2010; SAS, 2011). Results The logistic regression model treated “depression” as the reference category. Table 1 summarizes demographics including age, GPA, and gender. There were no significant differences on these variables between groups. Table 1. Demographics (n=165) Mean/Count Std. Dev. Range/Percent Age GPA Female 20.87 3.11 103 5.442 0.542 * 16 - 76 1.73 – 4.00 62.42% Backward Elimination resulted in a final model containing sleep and exercise, as well as the interaction between these two variables (see Table 2). While no other variables were significant at the 0.05 significance level, there was evidence that technology might have some impact on depression. The final model was assessed for goodness-of-fit using the Hosmer-Lemeshow test. No evidence indicating lack of fit was found (x2 = 8.424, p-value = 0.393). Table 2. Logistic Regression Model Sleep Exercise Sleep*Exercise Technology Coeff. SE Z P -0.067 -0.714 0.132 -0.067 0.200 0.253 0.045 0.035 -0.33 -2.83 2.95 -1.93 0.739 0.005 0.003 0.053 Odds Ratio 0.94 0.49 1.14 0.94 Lower Limit 0.63 0.30 1.05 0.87 Upper Limit 1.39 0.80 1.25 1.00 Due to the interaction between sleep and exercise levels, for interpretative purposes it is necessary to examine odds ratios for sleep at different fixed levels of exercise. Likewise odds ratios for exercise are examined at different fixed levels of sleep (see Table 3). Finally, Figure 1 displays the probability depression for various levels of sleep and exercise. The darker green areas represent combinations of sleep and exercise levels that put a person at a higher risk for depression. Table 3: Odds Ratio Estimates (Wald Cis) Exercise OR 95% CI OR 95% CI at Sleep = 5 0.96 0.87 - 1.06 Sleep at Exercise = 0 0.92 0.62 – 1.35 at Sleep = 6 1.09 0.99 - 1.21 at Exercise = 3 1.36 1.02 – 1.82 at Sleep = 7 1.25 1.07 - 1.46 at Exercise = 6 2.03 1.36 – 3.01 at Sleep = 8 1.43 1.13 - 1.80 at Exercise = 9 3.01 1.64 – 5.52 at Sleep = 9 1.63 1.19 - 2.23 at Exercise = 12 4.48 1.92 – 10.42 at Sleep = 10 1.86 1.24 - 2.77 at Exercise = 15 6.66 2.23 – 19.90 At low levels of sleep, the probability of depression is high and there is no evidence that increasing exercise affects risk for depression (see Figure 1). However, at medium and high levels of sleep, each additional hour of exercise decreases the odds of depression. For example, if a person gets 10 hours of sleep per night, for each additional hour of exercise lowers the odds of depression by a factor between 1.24 and 2.77. Likewise, at low levels of exercise, the probability of depression is high and there is no evidence that additional sleep affects a person’s risk for depression. However, at medium and high levels of exercise, additional sleep significantly decreases the odds of depression. For example, if a person gets 9 hours of exercise per week, each additional hour of sleep per night will lower his odds of depression by a factor between 1.64 and 5.52. Discussion/Conclusions This study hypothesized that low levels of sleep, low levels of exercise, and high levels of technology would increase the risk of depression in college students. It was found that both sleep and exercise do have the expected impact on risk of depression. Moreover, while atypically low levels of either sleep or exercise will put a person at a higher risk for depression, this study suggests that both must be increased to more “normal” levels in order for the odds of depression to decrease. Furthermore, once normal levels are reached, the two factors have a reinforcing interaction effect to further decrease the risk of depression. Technology use was indicated as marginally significant in the model. A future study might incorporate a larger sample to further assess this factor. A further limitation of this study is that it did not distinguish between academic and non-academic technology use. Considering that college students probably use technology for a large part of their schoolwork, we would expect high levels in the sample. Future studies should specifically address the issue of whether or not non-academic technology use is a factor. In addition to the logistic model, depression scores (0-27) were also considered using multiple linear regression (results not shown). This analysis was deemed not to be useful as the final model correctly identified only 25% of truly depressed students – likely a result of the essentially ordinal response. Future studies might consider whether an ordinal logistic model might be used to fine-tune predictions related to different levels of depression. Overall, the findings of this study were consistent with the previous literature. Students who engage in low levels of exercise and sleep are at greater risk for depression than those with adequate levels. While healthcare professionals may notice risky behaviors like drug and alcohol use to be associated with depression risk, they may often miss students who do not engage in these behaviors but are still at-risk. The present model did not find alcohol nor tobacco use to be significant predictors of depression, perhaps because of low levels of use in this sample. Given this information, it is even more important to identify the less obvious behaviors that put students at risk for depression. It is suggested that the findings presented here be used by a college health or wellness center to identify at-risk students and provide them with prevention techniques. References Carli, V., Hoven, C. W., Wasserman, C., Chiesa, F., Guffanti, G., Sarchiapone, M., Apter, A., Balazs, J., Brunner, R., Corcoran, P., Cosman, D., Haring, C., Iosue, M., Kaess, M., Kahn, J. P., Keeley, H., Postuvan, V., Saiz, P., Varnik, A. and Wasserman, D. (2014). A newly identified group of adolescents at “invisible” risk for psychopathology and suicidal behavior: findings from the SEYLE study. World Psychiatry, 13, 78–86. doi: 10.1002/wps.20088 Duckworth, K. (2013, April 1). What is Depression?. NAMI. Retrieved May 10, 2014, from https://www.nami.org/Template.cfm?Section=depression Haggerty, J. (2006). Risk Factors for Depression. Psych Central. Retrieved on May 10, 2014, from http://psychcentral.com/lib/risk-factors-for-depression/00058 Kroenke, K., Spitzer, R., Williams, J. (2001). The PHQ-9: validity of a brief depression severity measure. Journal of General Internal Medicine, 16, 606-613. doi: 10.1048/j.15251497.2001.016009606.x Minitab 16 Statistical Software (2010). [Computer software]. Minitab, Inc. (www.minitab.com) SAS Institute Inc. (2011). SAS System for Windows (Version 9.3) [Statistical processing software]. Cary, NC: SAS Institute Inc. Sona Systems, Ltd. (2002). [Software.] Available from: https://sona-systems.com