(BCR) signalling in B
advertisement
 signalling in B")
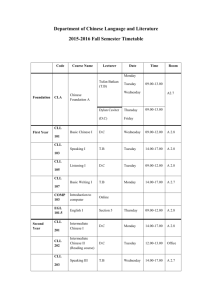
The Role of Estradiol in modulating B-cell receptor (BCR) signalling in B-cell Lymphomas and Leukaemias Eleni E Ladikou Supervisors: Prof Martin JS Dyer, Dr Sandrine Jayne Department of Cancer Studies and Molecular Medicine Medical Research Council (MRC) Toxicology Unit, University of Leicester INTRODUCTION Chronic Lymphocytic Leukaemia (CLL) is the most common form of leukaemia in the western world. In the UK only, 3000 new cases are diagnosed every year while in the United States it comprises 7% of all lymphomas (1). CLL is the accumulation of mature monoclonal CD5+ B cells in the blood, bone marrow and lymphoid tissues (2). Accumulating evidence demonstrates that male patients have a significantly higher incidence in CLL than females (ratio 1.8:1) whereas the latter have a much better prognosis and response to treatment (3). Therefore, we raised the hypothesis that this sex-dependent difference in incidence and prognosis could be the result of sex hormone differences. We decided to investigate the primary female sex hormone, estrogen. Estrogen exists in three forms in our body: Estradiol, Estrone and Estriol. Estradiol is the most abundant one in reproductive age (4). All these three estrogens are steroid hormones that enter the cell through the cell membrane and bind to intracellular receptors. Estrogen Receptor alpha (ERα) and Estrogen Receptor beta (ERβ) are transcription factors that will modulate gene expression of target genes (genomic action of ERα and ERβ). They are also involved in several signaling pathways that can affect the cell more rapidly through calcium influx (5). A third Estrogen receptor, GPR30, was recently discovered (5). This receptor is a G-protein coupled receptor with its own distinct molecular action and can act synergistically or antagonistically with the other two ERs. Estrogen is known to have a fundamental role in autoimmunity, predisposing females to it, and B-cell development. Estrogen Receptors and selective estrogen receptor ligands SERLs have been shown to play a role in B cell lymphoid malignancies. However, data on their role in primary CLL cells, to our knowledge, do not exist. This led us to investigate the role of estrogen and other SERLs in CLL. The aims of the present study were to investigate: a) the ERα and ERβ expression (at mRNA and protein level) in primary CLL B cells, b) the spontaneous apoptosis of CLL cells in absence and in presence of several stimuli (CpG ODN2216, CD40L, IgM) and c) the effect of Estradiol and SERLs on various cellular processes (e.g. apoptosis, proliferation) of primary CLL B cells. METHODS Patients and Cell lines Blood samples were obtained from patients from the Haematological Clinic at the Leicester Royal Infirmary, after informed consent. B cells were isolated from 36 CLL patients and 2 healthy volunteers by ficolling. EBV-transformed B cell lines (HRC5, GM14183, GM14295) and breast cancer cell line (MCF7) were used. Cell Cultures Cells were cultured in phenol red-free RPMI 1640 and stimulated with goat F(ab’)2 anti-human IgM, CpG-ODN/IL-2 or soluble CD40-L/IL4 in absence/presence of Estradiol , selective ERα, ERβ and GPR30 agonists (PPT, DPN, G1) , ERβ antagonists (PHTPP) and Tamoxifen at 1nM (selective estrogen receptor ligands- SERLS). Real time qPCR RNA were extracted using the RNEasy extraction kit (Qiagen), mRNA were reverse transcribed using SuperScriptTM III RT (Invitrogen). qPCR were performed using SYBR green kit (Bioline) and primers specific for ERα and ERβ. SDS-PAGE/Western Blot Cell lysates were run in 10% or 12% SDS-PAGE. Primary antibodies used were rabbit polyclonal anti-human ERα (HC-20, Santa Cruz), rabbit anti-ERβ antibody (PA1-311, Pierce), rabbit anti-phospho-ERk (91015, Cell Signalling) and rabbit anti-phospho-Syk (2701, Cell Signalling). Flowcytometry analysis Flowcytometry was used to assess cell apoptosis (using Annexin V-FITC staining (to detect phosphatidyl serine on cells in early apoptosis) and Propidium Iodide (that stains DNA and detect cells in late apoptotis) and cell proliferation (using Ki67 staining). RESULTS 1. Investigation of the Estrogen Receptors expression Total RNA were isolated from purified CLL B cells from 18 female and 18 male patients as well as EBV transformed normal B cell line (HRC). After reverse transcription, ERα and ERβ mRNA levels were investigated by real-time PCR using levels found in the HRC cell line as a reference. ERα mRNA expression was increased in all CLL patients with females showing higher mean expression when compared with male patients (p=0.0138) (Figure 1); ERβ gene expression was also increased to a lesser extent for all CLL patients, with females showing higher mean expression when compared with male patients (p=0.0515) (data not shown); the ERα: ERβ ratio between males and females was calculated for all patients. The mean ± SD of ratios showed no significant difference between the two sexes (p=0.3379). 256 ERα mRNA levels of Female Patients Fold difference 128 64 32 16 8 4 2 1 HRC WAR HOL MOC MOA PTJ PME HJC 256 FLJ SEJ SHA AMU SMO STJ WK HEJ SPO PMR EMP ERα mRNA levels of Male Patients 128 64 Fold difference Figure 1: Relative ERα gene expression ± SD (fold difference as compared to HRC) in 18 female CLL patients (top panel) and 18 male CLL patients (bottom panel) HRC level is set at 1 and serve as a reference 32 16 8 4 2 1 HRC SDE HU LJN GKI PC WJP GMJ NRT NRO SPJ VIA POM AGD MST STO BFM HTG BJR WLD VAK Whole cell protein extracts were prepared in parallel in the same patient samples. ERβ protein was expressed in both male and female CLL patients as well as in healthy volunteers (Figure 3). ERα levels on the other hand were very low, even beyond detection in some CLL patients when compared to MCF7, a breast cancer cell line (Figure 2). Interestingly, the ERα antibody recognized three unspecific bands at 68, 74 and 90 kDa. The band at 74kDa is B cell specific as it is present in all CLL patients and HRC but not in HEK293T cells transfected with ERα and MCF7. It could either be a different splicing isoform of ERα or a post-translational modification (e.g. monoubiquitination or sumoylation). Further investigation involving the transfection of ERα siRNA would confirm whether this band is related to ERα or not. Figure 12: ERα protein levels in CLL patients and 2 healthy volunteers (female TG, male GN). 20µg of total proteins from B cells of 18 CLL patients, HRC, MCF7 and ERα transfected cells (T) were loaded. Bands with asterisks (*, **, ***) represent unspecific bands. Figure 32: ERβ protein levels in the same patients and cell lines as in Figure2 except the addition of 183 (male GM14183), and 295 (female GM14295) which are cell lines of EBV transformed normal B cells. 2. Spontaneous apoptosis In contrast to CLL cells in the lymph node, CLL cells in the bloodstream (or cultured on a plastic dish) are subject to spontaneous apoptosis. Taking into consideration the sex dependent difference in CLL incidence and prognosis, we investigated the spontaneous apoptosis of both male and female CLL cells. After isolation from blood, cells were cultured for 1 or 4 days and analysed for the presence of Annexin V (a marker of early apoptosis) and for DNA content (staining with propidium iodide) using Flow Cytometry. Analysis of 43 patients reveals that female cells are more prone to spontaneous apoptosis when compared to male patients (p<000.1). Male patients had a significantly higher percentage of viable cells (42.17±6.9 at day1, 32.83±5.4 at day4) when compared to females (19.27±2.1 at day1, 14.09±2.3 at day4) (day1: p=0.006, day4: p=0.0057) (Figure 4). The difference in % of viable cells between Day 1 and Day 4 for each patient was also significant (-7.348 ± 9.345) (p=0.011) (data not shown). S p o n ta n e o u s A p o p to s is 100 M a le s F e m a le s 80 % v ia b le c e lls Figure 4: Mean ± SD of viable cells (% of total cells) in 43 patients (22 males, 21 females). Cells were cultured for 4 days receiving no stimulation. Males: 32.83±5.4, n=22. Females: 14.09±2.3, n=21 (t- test analysis p<0.0057) 60 40 20 0 M a le s F e m a le s P a t ie n ts This implies that differences in the internal microenvironment signals may predispose female cells to being more susceptible to spontaneous apoptosis. No current data on sex-dependent difference in spontaneous apoptosis exist, to our knowledge. In order to investigate whether sex-dependent difference in spontaneous apoptosis was linked with alterations in BCL2 and AID mRNA levels, we evaluated the expression of these two genes in 22 patients (a subset of the 43 previously studied). The result showed no sex dependent difference in BCL2 and AID mRNA levels (data not shown). Due to the fact that spontaneous apoptosis has been shown to depend on environmental pro-survival signals, we next examined the spontaneous apoptosis in CLL patient cells when stimulated with either of these pathways: a) Soluble CD40 ligand together with IL-4 mimicking the proliferative microenvironment of lymph nodes, b) anti-IgM antibody to mimic the in vivo engagement of BCR with antigen (adaptive immunity) and c) CpG oligodeoxynucleotides (ODN) with IL-2 to stimulate Toll-Like receptor 9 (innate immunity). CpG ODN and CD40L stimulation of CLL cells abrogated this sex-dependent difference in spontaneous apoptosis (p=0.45 and p=0.51). On the other hand, after IgM stimulation female CLL cells remain more susceptible to spontaneous apoptosis (p=0.02) (Figure 6). Data on CD40L and IgM stimulation have a small sample size (6 patients) and should therefore be extended. These data imply that spontaneous apoptosis in female CLL patient cells depends on specific environmental signals for their survival (Figure 5). CpG stimulated cells Unstimulated cells 100 S p o n ta n e o u s A p o p to s is 100 F e m a le s % v ia b le c e lls 60 40 80 % v ia b le c e lls M a le s 80 60 40 20 20 0 0 M a le s M a le s F e m a le s CD40L stimulated cells IgM stimulated cells 100 50 80 40 % v ia b le c e lls % v ia b le c e lls F e m a le s P a t ie n ts P a t ie n ts 60 40 20 30 20 10 0 0 M a le s F e m a le s P a t ie n ts M a le s F e m a le s P a t ie n ts Figure 5: Graph of Mean ± SD of viable cells (% of total cells) in CLL patients after 4 days in culture without/ with either CpG ODN2216, CD40L or IgM stimulation. 3. Effect of Estrogens on cell number We next wanted to know if the addition of Estradiol or SERLs would have an effect on the cell number of various B cell lines (RIVA, PR1, RAMOS) and primary cells. The addition of either Estradiol at 10nM or SERLs at a wide concentration range (1nM10µM) had no effect on cell number. These data are in contrast with those provided by the study of Yakimchuk et al (3). In their report, the use of Estradiol or DPN at 10 nM showed a strong antiproliferative effect on lymphoma growth in culture as compared to untreated cells. In agreement with our findings, but in contrast to those provided by Yakimchuk et al., early reports have shown an antiproliferative effect of Estradiol in human leukaemia cell lines and human acute leukaemia Jurkat T cells only at high concentration (>5µM), whereas at a lower concentration, no antiproliferative effect was seen (6,7). It is unlikely in our view that these very high concentrations are physiologically achievable (normal range of total Estradiol in serum: 15-350pg/ml). 4. Effect of Estrogens on cell apoptosis, proliferation and kinase phosphorylation One of the main tasks of this project was to investigate the effect of Estradiol and SERLs on various functions of B cells from CLL patients. Initially, we investigated the effect of compounds on apoptosis and proliferation of unstimulated primary B cell. None of the compounds tested showed any significant difference in either apoptosis or proliferation when compared with the untreated control (p>0.05) (data not shown). Next, we investigated the effect of Estradiol and SERLs on apoptosis, proliferation and kinase phosphorylation of IgM-stimulated CLL cells. We found that in one patient (out of 4 tested), Estradiol and PPT (ERα selective agonist) attenuated the time-dependent changes in ERK and SYK phosphorylation; in contrast, DPN (ERβ selective agonist) enhanced the time-dependent changes in ERK and SYK phosphorylation (Figure 6). Figure 6: Western Blot analysis of phospho-ERK and phospho-SYK in B cells isolated from a CLL patients at various timepoints after IgM stimulation (1-30mins). Cells were pretreated ineither Estradiol or different SERLs (Estradiol, DPN, PPT) at 10µM. Although this result is promising, more patient samples need to be analysed to identify groups of patients for which the BCR signaling pathway is affected by the addition of SERLs. In our experiments, the overall effect of Estradiol and SERLs on apoptosis and proliferation in stimulated primary B cells was variable, e.g. ERα agonist may alter apoptosis depending on the experimental conditions. This may be explained by the fact that, because different signalling stimuli were used in each condition activating different pathways, this resulted in a variable internal microenvironment, hence the differential response to Estradiol and SERLs. Another hypothesis for the lack of consistent results regarding response of B cells to Estradiol and SERLs could be that Estrogen Receptors in CLL cells may already be highly phosphorylated, a condition which would render ER unresponsive to estrogen treatment. The following facts support this hypothesis. a) Previous studies have shown that Estrogen Receptors can be phosphorylated by ERK and AKT, activating ERs in a ligand-independent manner (8), b) CLL B cells are characterized by high tonic signalling having SYK and NF-κB constitutively phosphorylated. This is additionally true for ERK in almost half of CLL cases (9) and c) Our experiments also show that ERK and SYK are slightly phosphorylated even at timepoint 0 before exogenous stimulation. CONCLUSION AND FUTURE WORK In this study I could show that CLL B cells derived from female patients are more prone to spontaneous apoptosis than cells from male patients. Furthermore, stimulation of the cells by CD40L/IL4 and CpG Oligodeoxynucleotides abrogated this difference, indicating that female cells might depend more on environmental prosurvival signals than their male counterparts. Additionally, engagement of either ERα or ERβ altered BCR signal duration. ERβ selective antagonists did not induce apoptosis in CLL cells. My study provides novel data to explain the gender difference in CLL incidence and prognosis as well as estrogen signalling in B-cells Future studies should include: Repeat the spontaneous apoptosis assay on a larger sample size and investigate further the effect of stimulation by CD40L, IgM or CpG ODN Determination of the mRNA and protein levels of various genes associated with apoptosis (Bclx, Mcl1 for example) and proliferation in male and female samples. Effect of various stimuli on ERα, ERβ, GPR30 mRNA and protein levels effect of SERL pre-treatment in ER levels and several signalling parameters (kinases and transcription factors such as NF-κB), apoptosis and proliferation. This work was presented as an oral presentation at ISCOMS- International Student Congress of (bio)Medical Sciences –one of the world’s leading student conferences in the (bio)medical sciences (Groningen, June 2013). It is also accepted for a poster presentation at the 24th European Student Conference (Berlin, September 2013). The Pathological Society is acknowledged for providing us with grants to support this study. REFERENCES (1) Kuppers R. Mechanisms of B-cell lymphoma pathogenesis. Nat Rev Cancer 2005 Apr;5(4):251-262. (2) Herishanu Y, Perez-Galan P, Liu D, Biancotto A, Pittaluga S, Vire B, et al. The lymph node microenvironment promotes B-cell receptor signaling, NF-kappaB activation, and tumor proliferation in chronic lymphocytic leukemia. Blood 2011 Jan 13;117(2):563-574. (3) Yakimchuk K, Norin S, Kimby E, Hagglund H, Warner M, Gustafsson JA. Up-regulated estrogen receptor beta2 in chronic lymphocytic leukemia. Leuk Lymphoma 2012 Jan;53(1):139-144. (4) Liang J, Shang Y. Estrogen and Cancer. Annu Rev Physiol 2012 Oct 8. (5) Prossnitz ER, Barton M. The G-protein-coupled estrogen receptor GPER in health and disease. Nat Rev Endocrinol 2011 Aug 16;7(12):715-726. (6) Mossuz P, Cousin F, Castinel A, Chauvet M, Sotto MF, Polack B, et al. Effects of two sex steroids (17beta estradiol and testosterone) on proliferation and clonal growth of the human monoblastic leukemia cell line, U937. Leuk Res 1998 Nov;22(11):1063-1072. (7) Jun DY, Park HS, Kim JS, Kim JS, Park W, Song BH, et al. 17Alpha-estradiol arrests cell cycle progression at G2/M and induces apoptotic cell death in human acute leukemia Jurkat T cells. Toxicol Appl Pharmacol 2008 Sep 15;231(3):401-412. (8) Thomas C, Gustafsson JA. The different roles of ER subtypes in cancer biology and therapy. Nat Rev Cancer 2011 Jul 22;11(8):597-608. (9) Scupoli MT, Pizzolo G. Signaling pathways activated by the B-cell receptor in chronic lymphocytic leukemia. Expert Rev Hematol 2012 Jun;5(3):341-348.