here
advertisement

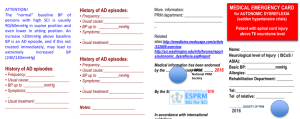
WORKING TOWARDS EUROPEAN / INTERNATIONAL MEDICAL EMERGENCY AUTONOMIC DYSREFLEXIA CARD (You are kindly asked to make your comments on this word document and send it back to: C-A.Rapidi: rapidicha@hotmail.com) During the initial rehabilitation process autonomic dysreflexia (AD) is inadequately emphasized by the Rehabilitation team (usually AD is a problem in more chronic phase). Patients with SCI and their caregivers are coping with the tremendous changes in their quality of life post injury; and have poor recognition of the symptoms and understanding of the causes of AD. (Table 1: Knowledge of AD among patients / their caregivers / health personnel) Table 1: Knowledge of AD among patients / their caregivers / health personnel Author / year / country / Total Sample Size CF McGillivray, et al. JSCM, 2009 Canada N=100 chronic SCI, 16 family members Method / Aim Results self-report mail survey to: (a) evaluate knowledge of AD among SCI consumers and their family members and (b) to identify the preferred format and timing of education on AD for these stakeholders. high-risk group for AD, 41% of the sample had never heard of the condition J Schottler, et al. Spinal Cord, 2009 USA N=215 (1-21 years old) The incidence of knowledge of AD from patient and caregiver perspectives 40% of patients & 44% of caregivers claimed symptoms of AD, and out of them: 15% of patients & 9% of caregivers did not know the definition of AD or did not recognize the term AD when first asked CR Jackson, R Acland Emerg Med J, 2011 New Zealand N=70 (18 doctors, 52 nurses) A questionnaire was designed to assess the knowledge of the ED staff on AD 41% of the staff in emergency department could not answer any questions There is a need to improve knowledge and management of AD among healthcare professionals not specialized in SCI, ED personnel, Primary care, patients and caregivers A series of strategies may contribute to improve knowledge and management of AD: • Campaign in general hospitals without experience in SCI rehabilitation • Information in triage folders • Educational courses on AD among healthcare professionals • Leaflets with medical information concerning AD in emergency rooms and GPs’ offices • Education of patients, their families and care givers • Web sites where health professionals and consumers can obtain information from one another. • Carrying an AD card AUTONOMIC DYSREFLEXIA EMERGENCY CARD Autonomic dysreflexia cards have been developed by different countries, organizations, in different sizes, with different information, focusing in different target groups. The different providers of cards are (Information by internet surfing): • Patients’ Associations & non-profit charity Foundations (the majority) • SCI Hospitals & Rehabilitation Centers • SCI Scientific Societies There are many different things to consider on the medical emergency AD card practical issues: size, letters’ size: satisfactory or small, squashed text, text easy to read or not text quality: concisely written text (what AD is, symptoms, signs, causes), clear recommendations for health providers,1st line drug, clear recommendations for patients & caregivers personal information: Name, contact details, Rehabilitation Department/Hospital or other center, responsible for the patient and his medical file, Neurological Level of Injury, AIS, previous AD episodes who is responsible for the AD card creation AND when it is updated: clearly written: who is scientifically responsible for what is written on the card, card provider’s contact details for more information who is responsible for the distribution of this AD card A universal AD card should be suggested by the SIG for SCI of ESPRM in English language and should be translated to national languages too. Patients could curry in their wallets both versions. This card with a universal figure and same colors would be easily recognized all over the world. This card: • • • • • Should have a convenient shape, like a wallet card, to be easily carried Should have some individualized information Should be official and endorsed by scientific societies Should be regularly updated It may be distributed by the PRM Department/Hospital/Center, primary healthcare provider A working hypothesis for a European emergency medical AD card (you san print this card from the attached pptx “AD CARD, 2016 eng”) Dimensions: 5.3/8.5 folded = wallet size 8 pages 1st page: definition of AD (very briefly) personal ID Neurological Level of Injury (NLI) Basal Blood Pressure (BP basal) Allergies Rehabilitation Department tel. of relatives 2nd page: definition of AD 3rd page: common signs & symptoms, common causes 4th & 5th page: what to do (physicians) 6th page: awareness for “physiologic” BP of SCIed patients, previous AD episodes details 7th page: previous AD episodes details, notes 8th page: for more information contact Rehabilitation department & the following links Medical information is endorsed by: National PRM Society (HSPRM-SCIS & University of Patras SCI Reha Department) ESPRM (SIG for SCI) Comments: wallet size, clear recommendations, 1st line drug: NIFEDIPINE 1st Page MEDICAL EMERGENCY CARD for AUTONOMIC DYSREFLEXIA (sadden hypertensive crisis) Patient with spinal cord injury above T6 neurotome level Name: __________________________ Neurological level of Injury ( ISCoS / ASIA): ________________________ Basic BP: ______________mmHg Allergies: ______________________ Rehabilitation Department: ________ ________________________________ Tel:____________________________ Tel of relative: ______________ 8th Last page More information: PRM department: ___________________ __________________________________ Related sites: http://emedicine.medscape.com/article/322809-overview http://sci.washington.edu/info/forums/reports/autonomic_dysreflexia.as p#report Medical information has been endorsed: by the National Society PRM, by the ESPRM (SIG for SCI) In accordance with international guidelines 2nd Page AUTONOMIC DYSREFLEXIA (AD) Patient with tetraplegia or high paraplegia (SCI above T6) may present a sudden dysfunction of autonomic nervous system resulting from stimulus below neurological level of injury, this dysfunction is called: AD AD is an unopposed overactivity of sympathetic nervous system, leading to a sudden increase of blood pressure. If AD is not treated in time may lead to intracranial haemorrhage, stroke, seizures or even death 3rd Page COMMON SYMPTOMS & SIGNS feeling of great anxiety high BP, sudden rapid increase pounding headache flushing & sweating above the level of injury paling, vasoconstriction below the level of injury (sweating sometimes) slow or rapid heart rate breathing difficulty blurring of vision stuffy nose Nausea COMMON CAUSES urine retention plugged catheter fecal impaction pressure sore or burn ingrown toenail fractures of lower limbs UTI any noxious stimulus below the level of injury 4th Page (Treatment) • • • • Sit patient upright (not lying down) Monitor blood pressure every 3-5 min Remove whatever is tight below the level of the lesion (clothing, etc.) Quick physical exam to include abdomen for distended bladder or bowel, lower limbs for skin lesion, fractures, etc. in order to reveal the stimulus that caused AD and treat it • If indwelling urinary catheter is in place, check for obstructions 5th Page (Treatment) • If an indwelling catheter is not in place, catheterize the patient using anesthetic jelly • ATTENTION: If there is a need to check bowel, this must be done using anesthetic jelly • If BP despite previous management is high (>150mmHg), give an antihypertensive with rapid onset and short duration anti-hypertensive drugs (e.g.sublingual nifedipine), may repeat in 20-30min, and continue investigate causes of AD • If IV antihypertensives are needed, this should be done only in a monitoring setting of ICU 6th Page ATTENTION! The “normal” baseline BP of persons with high SCI is usually 90/60mmHg in supine position and even lower in sitting position. An increase >20mmHg above baseline BP is an AD episode, and if this not treated immediately, may lead to extremely increased BP (240/130mmHg) History of AD episodes: Frequency:______________________ Usual cause:_____________________ BP up to __________mmHg Symptoms:______________________ Usual treatment:__________________ _______________________________ 7th Page History of AD episodes: Frequency:_________________________ Usual cause:_______________________ BP up to __________mmHg Symptoms:_________________________ Usual treatment:____________________ __________________________________ History of AD episodes: Frequency:_________________________ Usual cause:_______________________ BP up to __________mmHg Symptoms:_________________________ Usual treatment:____________________ __________________________________ Notes: _____________________________ _____________________________________ (You are kindly asked to make your comments on this word document and send it back to: C-A.Rapidi: rapidicha@hotmail.com) Thank you in advance for your contribution in this effort: “working towards a medical emergency AD card”. Christina-Anastasia RAPIDI President of the Hellenic Spinal Cord section of PRM