supplemental data: supplemental methods: ablation procedures
advertisement

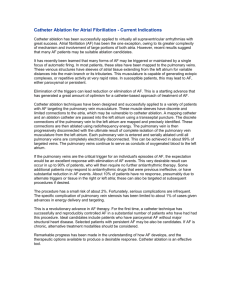
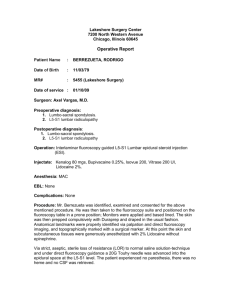
supplemental data: supplemental methods: ablation procedures: typical flutter (AFL): The electrophysiological study was performed under sedation utilizing midazolam and fentanyl. One quadripolar diagnostic catheter (Biosense Webster, California, USA) was advanced into right ventricular apex and one decapolar catheter (Webster® CS uni-directional catheter, Biosense Webster, California, USA) into the coronary sinus under fluoroscopic guidance. Subsequently, in the CARTO-3 group (c3) the infero-septal and infero-lateral tricuspid annulus as well as the junction between the inferior vena cava and the right atrium were marked in the EAM (electroanatomical map) as anatomical landmarks of the cavo-tricuspid isthmus (CTI) under fluoroscopic guidance. Afterwards, if tachycardia was present, an entrainment mapping was performed at the CTI to confirm typical flutter. Now an point by point ablation line at the CTI was created under guidance of the EAM and active fluoroscopy if necessary (Thermocool® SF catheter, Biosense Webster, California, USA; ablation settings: 40W at an irrigation rate of 15ml/min with a maximum temperature of 43°C). Finally the bidirectional block of the line was confirmed with differential pacing under guidance of the EAM and active fluoroscopy if necessary. In the CARTO-UNIVU group (cU) after positioning of the diagnostic catheters the UNIVU module was registered and one X-ray image in RAO 20-30° and one X-ray image in LAO 50-60° were recorded. Then, the infero-septal and inferolateral tricuspid annulus as well as the junction between the inferior vena cava and the right atrium were marked in the EAM as anatomical landmarks of the cavo-tricuspid isthmus (CTI) under active catheter tracking in the pre recorded X-ray images and only if necessary under fluoroscopic guidance. Afterwards, if tachycardia was present, an entrainment mapping was performed at the CTI to confirm typical flutter. Now an point by point ablation line at the CTI was created under guidance of the EAM, active catheter tracking in pre recorded X-ray images and active fluoroscopy only if necessary (ablation settings: 40W at an irrigation rate of 15ml/min with a maximum temperature of 43°C). Finally the bidirectional block of the line was confirmed with differential pacing under guidance of the EAM, active catheter tracking in pre recorded X-ray images and active fluoroscopy only if necessary. atrial fibrillation (AF): The electrophysiological study was performed under sedation utilizing midazolam fentanyl and propofol. One quadripolar diagnostic catheter (Biosense Webster, California, California, USA) was advanced into right ventricular apex and one decapolar catheter (Webster® CS uni-directional catheter, Biosense Webster, California, USA) into the coronary sinus under fluoroscopic guidance. A single trans-septal puncture was performed with a steerable intra-cardiac sheath (Agilis™ NxT, St. Jude Medical, Inc., Minnesota, USA) under fluoroscopy guidance. Upon left atrial access, a bolus of unfractionated Heparin (100 IU/kg) was administered and repeated intermittently to maintain an activated clotting time between 300 and 350 ms. If atrial fibrillation was present during the procedure an electrical cardioversion was performed. In the CARTO-3 group (c3) an EAM including substrate-mapping (voltage values higher than 0.5 mV were defined as healthy myocardium. Voltage values below 0.2 mV were defined as total scar) of the left atrium and the pulmonary veins was acquired under fluoroscopic guidance with a multipolar mapping catheter (Lasso® eco NAV catheter, Biosense Webster, California, USA). During the EAM acquisition selective angiographies of the pulmonary veins were done for fluoroscopic confirmation of catheter position throughout PVI. Now the acquired EAM was merged to the reconstructed CT with a visual alignment technique and well defined anatomical landmarks, followed by registration of the surface. Subsequently, in all atrial fibrillation procedures a point by point pulmonary vein isolation was performed with pace and ablate technique under guidance of EAM and if necessary under active fluoroscopy (ablation settings: 40W at an irrigation rate of 15ml/min with a maximum temperature of 43°C, reduction of the RF energy to 30W at the left atrial posterior wall, intra-oesophageal temperature monitoring with RF stop cut off of 39°C). In case of additional low voltage areas within the left atrium these areas were isolated by point by point creation of additional ablation lines. Finally the conformation of PVI and bidirectional block of all additional lines was performed under EAM and if necessary fluoroscopic guidance. In the CARTO-UNIVU group (cU) after trans-septal puncture the UNIVU module was registered and angiographies of the left atrium and the pulmonary veins were recorded in RAO (20-30°) and LAO (50-60°) views. The further procedure was done like in the CARTO-3 group but under active catheter tracking in the angiographies and active fluoroscopy only if necessary. ectopic atrial tachycardia (EAT): One quadripolar diagnostic catheter was advanced into right ventricular apex and one decapolar catheter into the coronary sinus under fluoroscopic guidance. If patient were under sinus rhythm the EAT was triggered with programmed atrial stimulation. If the origin of the tachycardia was supposed in the left atrium a single trans-septal puncture was performed with a steerable intra-cardiac sheath (Agilis™ NxT, St. Jude Medical, Inc., Minnesota, USA) under fluoroscopy guidance. In the CARTO-3 group (c3) an EAM including activation-mapping of the right or left atrium were acquired under fluoroscopic guidance. Subsequently, the ectopic focus was ablated under guidance of the EAM and if necessary under active fluoroscopy (ablation settings: 30-40W at an irrigation rate of 15ml/min with a maximum temperature of 43°C). In the CARTO-UNIVU group (cU) after positioning of the diagnostic catheters and optional trans-septal puncture the UNIVU module was registered and one X-ray image in RAO 20-30° and one X-ray image in LAO 50-60° were recorded. The further procedure was done like in the CARTO-3 group but under active catheter tracking in the pre recorded X-ray images and active fluoroscopy only if necessary. In all patients an observational time of 15 minutes was kept after the last ablation to rule out an early recurrence. accessory pathyway (AP): One quadripolar diagnostic catheter was advanced into right ventricular apex and one decapolar catheter into the coronary sinus under fluoroscopic guidance. If the AP was supposed in the left atrium a single transseptal puncture was performed with a steerable intra-cardiac sheath (Agilis™ NxT, St. Jude Medical, Inc., Minnesota, USA) under fluoroscopy guidance. In the CARTO-3 group (c3) an EAM including activation-mapping of the mitral or tricuspid annulus were acquired under fluoroscopic guidance. Subsequently, the AP was ablated under guidance of the EAM and if necessary under active fluoroscopy (ablation settings: 30-40W at an irrigation rate of 15ml/min with a maximum temperature of 43°C). In the CARTO-UNIVU group (cU) after positioning of the diagnostic catheters and optional transseptal puncture the UNIVU module was registered and one X- ray image in RAO 20-30° and one X-ray image in LAO 50-60° were recorded. The further procedure was done like in the CARTO-3 group but under active catheter tracking in the pre recorded X-ray images and active fluoroscopy only if necessary. In all patients an observational time of 15 minutes was kept after the last ablation to rule out an early recurrence. premature ventricular complexes (PVCs) One quadripolar diagnostic catheter was advanced into right ventricular apex and one decapolar catheter into the coronary sinus under fluoroscopic guidance. If the PVC was supposed in the left ventricle a single trans-septal puncture was performed with a steerable intra-cardiac sheath (Agilis™ NxT, St. Jude Medical, Inc., Minnesota, USA) under fluoroscopy guidance. In case the origin of the PVC was supposed in the aortic valve or in the left ventricular outflow tract, a retrograde trans-aortic access of the ablation catheter was chosen. In the CARTO-3 group (c3) EAMs including activation- or pace-mapping of the supposed cardiac chambers were acquired under fluoroscopic guidance. Subsequently, the PVC was ablated under guidance of the EAM and if necessary under active fluoroscopy (ablation settings: 30-50W at an irrigation rate of 1530ml/min with a maximum temperature of 43°C). In the CARTO-UNIVU group (cU) after positioning of the diagnostic catheters and optional trans-septal puncture or trans-aortic access the UNIVU module was registered and one X-ray image in RAO 20-30° and one X-ray image in LAO 50-60° were recorded. The further procedure was done like in the CARTO-3 group but under active catheter tracking in the pre recorded X-ray images and active fluoroscopy only if necessary. In all patients an observational time of 15 minutes was kept after the last ablation to rule out an early recurrence. ventricular tachycardia (VT): One quadripolar diagnostic catheter was advanced into right ventricular apex and one decapolar catheter into the coronary sinus under fluoroscopic guidance. If patient were under sinus rhythm the VT was tried to trigger with programmed ventricular stimulation. The triggered VT was recorded and terminated with anti-tachycardia pacing or electrical cardioversion. In case the an epicardial origin of the tachycardia was supposed, an epicardial puncture was performed under fluoroscopic guidance and an steerable sheath (Agilis™ EPI, St. Jude Medical, Inc., Minnesota, USA) was advanced into the pericardial space. If the origin of the tachycardia was supposed in the left ventricle a single trans-septal puncture was performed with a steerable intra-cardiac sheath (Agilis™ NxT, St. Jude Medical, Inc., Minnesota, USA) under fluoroscopy guidance. In the CARTO-3 group (c3) angiographies of the ventricles in RAO 20-30° and in LAO 50-60° were recorded (in case von severe renal dysfunction or hemodynamic instability only X-ray images were recorded). Then EAM including substrate-, pace- and activation-mapping of the right or left ventricle (endo- and epicardial) were acquired under fluoroscopic guidance. Subsequently, a substrate modification due to ablation of the low voltage areas under guidance of the EAMs and if necessary under active fluoroscopy (ablation settings: 40-50W at an irrigation rate of 15ml/min with a maximum temperature of 43°C) was performed. In the CARTO-UNIVU group (cU) after positioning of the diagnostic catheters and optional epicardial and trans-septal puncture the UNIVU module was registered and angiographies of the ventricles in RAO 20-30° and in LAO 50-60° were recorded (in case von severe renal dysfunction or hemodynamic instability only X-ray images were recorded). The further procedure was done like in the CARTO-3 group but under active catheter tracking in the pre recorded angiographies and active fluoroscopy only if necessary. supplemental figures: fluoroscopy time in min 20 p < 0.001 p = 0.001 15 10 5 0 15.7 5.2 PVI only 16.2 7.8 PVI + ablation lines carto univu fluoroscopy dose in cGycm2 carto 3 10000 p < 0.001 p = 0.06 8000 6000 4000 2000 0 8068 3049 PVI only 6836 4498 PVI + ablation lines supplemental figure 1: fluoroscopy time and fluoroscopy dose in AF procedures (c3 vs. cU) subgroup analyses of fluoroscopy time and dose used for the AFablation procedures CARTO-3 vs. CARTOUNIVU: in PVI only subgroup only an PVI was performed, in the PVI+ablation lines group a PVI and additional ablation lines were necessary during procedure. data presented as mean±SEM, p<0.05 was defined as significant supplemental figure 2: RF time and RF dose in different ablation procedures (c3 vs. cU) RF (radiofrequency) application time in seconds [sec] and RF application dose in Ws of the different ablation procedures CARTO-3 vs. CARTO-UNIVU, AFL: ablation of typical flutter, AF: atrial fibrillation, EAT: ectopic atrial tachycardia, AP accessory pathway, PVC: premature ventricular contractions, VT: ventricular tachycardia. RF: radio frequency, data presented as mean±SEM, p<0.05 was defined as significant