Pathology Ch11 - Blood Vessels - pp483-521
advertisement

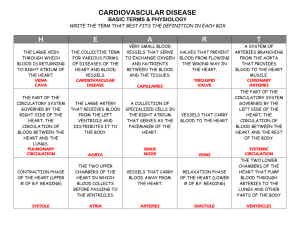
Pathology Ch11 - Blood Vessels - pp483-521 Vascular Structure and Function Arterial walls are thicker than corresponding veins Atherosclerosis affects mainly elastic and muscular arteries HTN affects small muscular arteries and arterioles Different varieties of vasculitis involve only vessels of a certain caliber Layers of vasculature walls: o Intima Single layer of endothelial cells sitting on a basement membrane Demarcated from media by the internal elastic lamina o Media Varies in structure according to functional demands Arteries: several well-organized concentric layers of SM Veins: SM arranged more haphazardly Elastic arteries (ex. aorta): high elastin content, lost with aging Muscular arteries: circumferentially oriented SM regulated by ANS inputs and local metabolic factors Arterioles: principal points of physiologic resistance to blood flow (resistance inversely proportional to diameter4 >> small changes in diameter can have profound effects on blood pressure) o Adventitia Separated from media by external elastic lamina Consists of loose CT containing nerve fibers and vasa vasorum (vessels fo the vessels) Arteries divided into 3 types based on size and structural features: o Large/elastic arteries = aorta, major branches off the aorta (subclavian, carotid, iliac aa.), pulmonary aa. o Medium/muscular arteries = smaller branches of the aorta (ex. coronary and renal aa.) o Small arteries (<2mm) and arterioles (20-100μm) within tissues and organs Capillaries (7-8μm) are roughly the size of RBCs o Have endothelial lining, but no media o Pericytes (resemble SM cells) lie just beneath the endothelium o Collectively huge cross-sectional area and low flow rate > ideal for gas exchange between blood and tissues o Highest density in tissues w/ high metabolic rates (ex. myocardium and brain) Postcapillary venules > collecting venules > small > medium > large vv. o Most inflammatory reactions, vascular leakage, and leukocyte exudation occurs from postcapillary venules Compared to arteries, veins have larger diameters, larger lumens, and thinner/less organized walls o Contains 2/3 of total blood volume o Less rigid walls > subject to dilation/compression, and infiltration by tumors and inflammatory processes o Reverse flow prevented by venous valves Lymphatics are thin-walled channels lined by specialized endothelium o Return interstitial tissue fluid and inflammatory cells back to blood stream o Can also transport microbes and tumor cells (dissemination) Vascular Anomalies Developmental or berry aneurysms o Occur in cerebral vessels o Rupture > intracerebral hemorrhage Arteriovenous fistulas o Direct connections between arteries and veins > bypass capillary bed o From developmental defects, arterial aneurysm into adjacent vein, penetrating injuries, or inflammatory necrosis o Rupture > intracerebral hemorrhage o Can shunt enough blood to force heart to pump additional volume > high-output cardiac failure Fibromuscular dysplasia o Focal irregular thickening in medium and large muscular arteries (ex. renal, carotid, splanchnic, vertebral) o Thickened by medial and intimal hyperplasia and fibrosis > luminal stenosis o Renal artery stenosis > renovascular HTN o Adjacent vessels segments show thinned media > aneurysms > can rupture o "String of beads" appearance o Most common in young women Vascular Wall Response to Injury Endothelial cells can be "activated" > express adhesion molecules, cytokines, chemokines, growth factor, and vasoactives Endothelial dysfunction = alterations in endothelial phenotype (often proinflammatory and prothrombogenic) Vascular SM cells = predominant element of media > important in vascular repair and pathologic processes (atherosclerosis) Vascular injury (associated w/ endothelial cell dysfunction or loss) > stimulates SM cell recruitment and proliferation and associated matrix synthesis >> intimal thickening > may impede vascular flow Hypertensive Vascular Disease Sustained systolic >139mmHg or diastolic >89mmHg = inc risk of atherosclerotic disease Essential hypertension = idiopathic HTN in 90-95% of cases Secondary hypertension = resulting from renal or adrenal disease o Renal: acute glomerulonephritis, chronic renal disease, polycystic disease, renal artery stenosis, renal vasculitis, renin-producing tumors o Endocrine: adrenocortical hyperfunction, exogenous hormones, pheochomocytoma, acromegaly, hypo/hyperthyroidism, pregnancy o Cardiovascular: coarcation of aorta, polyarteritis nodosa, inc. intravascular volume, inc. CO, rigidity of aorta o Neurologic: psychogenic, increased intracranial pressure, acute stress Malignant hypertension = rapidly rising bp that can lead to death within 1-2 years (usually >200/120) Blood Pressure Regulation o BP = function of cardiac output and peripheral vascular resistance Cardiac output = function of stroke volume and heart rate Stroke volume dictated by filling pressure (blood volume) Heart rate/contractility regulated by adrenergic systems Peripheral resistance = regulated at level of arterioles by neural and hormonal inputs Vasoconstrictors (angiotensin II, catecholamines, endothelin) Vasodilators (kinins, prostaglandins, NO) Autoregulation > vasoconstriction to protect tissues against hyperperfusion Fine-tuned by tissue pH and hypoxia to accommodate local metabolic demands o Factors released from kidneys, adrenals, and myocardium influence vascular tone and regulate blood volume Kidneys reabsorb 98% of sodium via active sodium transporters Remaining sodium is reabsorbed by epithelial sodium channel (ENaC) which is regulated by reninangiotensin system > determines net sodium balance Kidneys and heart have cells that sense changes in bp or volume > release effectors to normalize Renin = proteolytic enzyme produced by renal juxtaglomerular cells, released in response to low blood pressure in afferent arterioles, elevated levels of catecholamines, or low sodium levels in the distal convoluted renal tubules o Renin cleaves angiotensinogen to angiotensin I > converted to angiotensin II by ACE (produced by vascular epithelium) o Angiotensin II raises bp by (1) inducing vascular contraction, (2) stimulating aldosterone secretion which increases Na+ resorption in distal convoluted tubule, (3) increasing tubular Na+ resorption Kidneys also produce vascular relaxing substances (prostaglandins and NO) that counterbalance vasopressor effects of angiotensin Myocardial natriuretic peptides from atrial and ventricular myocardium inhibit sodium resorption in distal renal tubules and induce systemic vasodilation Pathogenesis of Hypertension o Idiopathic/primary = multiple small changes in renal sodium homeostasis and/or vessel wall tone/structure Genetic factors influence blood pressure regulation. Cumulative effects of polymorphisms. Reduced renal sodium excretion in the presence of normal arterial pressure may be key initiating event Vasoconstrictive influences such as factors that induce vasoconstriction or stimuli that cause structural changes in vessel wall Environmental factors such as stress, obesity, smoking, physical activity, and heavy salt consumption o Secondary = Renovascular hypertension Renal artery stenosis decreases glomerular flow and pressure in afferent arteriole of glomerulus Induces renin secretion > increases vascular tone and blood volume Single-gene disorders Gene defects affecting enzymes involved in aldosterone metabolism o Aldosterone synthase, 11β-hydroxylase, 17α-hydroxylase o Leads to increase in secretion of aldosterone Mutations affecting proteins that influence sodium reabsoption o Ex. Liddle syndrome caused by gain-of-function mutations in epithelial Na+ channel protein > inc. distal tubular reabsorption of sodium in response to aldosterone Vascular Pathology in Hypertension o Hypertension accelerates atherogenesis and causes degenerative changes in the walls of large and medium arteries > can lead to both aortic dissection and cerebrovascular hemorrhage o Also associated w/ 2 forms of small blood vessel disease: hyaline arteriosclerosis and hyperplastic arteriosclerosis Hyaline arteriosclerosis: arterioles show hyaline thickening w/ associated luminal narrowing. Reflect plasma protein leakage across injured endothelial cells and increased smooth muscle cell matrix synthesis due to chronic hemodynamic stresses of hypertension. Nephrosclerosis > impaired renal flow and glomerular scarring. Hyperplastic arteriosclerosis: lesions occur in severe hypertension. Vessels exhibit concentric, laminated thickening of the walls (onion-skin) w/ luminal narrowing. Laminations consist of SM cells w/ thickened, reduplicated basement membrane. Accompanied by fibrinoid deposits and vessel wall necrosis (necrotizing arteriolitis), particularly in the kidney. Arteriosclerosis Hardening of the arteries due to arterial wall thickening and loss of elasticity Arteriolosclerosis: small arteries and arterioles > downstream ischemic injury. Monckeberg medial sclerosis: calcification of walls of muscular arteries, involving internal elastic membrane. Calcification doesn't encroach the lumen > not usually clinically significant. Atherosclerosis: most frequent and clinically important pattern Atherosclerosis Underlies the pathogenesis of coronary, cerebral, and peripheral vascular disease o Can lead to MI, aortic and carotid atherosclerotic disease, and stroke Cause intimal lesions (atheromas) that protrude into vessel lumens o Atheromatous plaque made up of lipid core covered by fibrous cap > obstruct blood flow, increase diffusion distance from the lumen to the media, and can rupture leading to obstructive vascular thrombosis Constitutional Risk Factors o Genetics = usually polygenic o Age = doesn't usually become clinically manifested until middle age or later o Gender = premenopausal women are relatively protected compared to men. After menopause the risk increases and can become higher than that of men. Modifiable Major Risk Factors o Hyperlipidemia = hypercholesterolemia especially. o Hypertension = both systolic and diastolic levels are important o Cigarette smoking = prolonged smoking of 1+ packs a day increases chance or ischemic heart disease death 2x o Diabetes mellitus = induces hypercholesterolemia Additional Risk Factors o Inflammation = C-reactive protein (CRP) is a good marker for inflammation correlated w/ ischemic heart disease CRP is acute phase reactant synthesized by the liver in response to IL6 > innate immune response Good marker for MI, stroke, peripheral arterial disease, and sudden cardiac death o Hyperhomocystinemia = serum homocysteine correlates w/ coronary atherosclerosis, peripheral vascular disease, stroke, and venous thrombosis Homocystinuria (due to rare inborn errors of metabolism) > premature vascular disease Low folate and vitamin B12 can increase homocystine o Metabolic syndrome = associated w/ central obesity, characterized by insulin resistance, HTN, dyslipidemia, hypercoagulability, and proinflammatory state o Lipoprotein a [Lp(a)] = altered form of LDL that contains apolipoprotein B-100 linked to apo A. Associated w/ coronary and cerebrovascular disease risk, independent of total cholesterol or LDL levels o Factors affecting hemostasis = platelet-derived factors and thrombin (procoagulants and proinflammatory) o Other factors = stressful lifestyle, obesity Pathogenesis of Atherosclerosis o o o o o o o o o o Response to injury hypothesis = atherosclerosis is a chronic inflammatory and healing response of the arterial wall to endothelial injury. Lesion progression occurs through interaction of modified lipoproteins, monocyte-derived macrophages, and T lymphocytes w/ endothelial cells and SM cells of the arterial wall (1) Endothelial injury and dysfunction > increased vascular permeability, leukocyte adhesion, and thrombosis Most important causes of endothelial dysfunction = hemodynamic disturbances and hypercholestrolemia Hemodynamic disturbances = plaques tend to occur in areas of disturbed flow patterns Dyslipoproteinemias = Increased LDL cholesterol levels Decreased HDL cholesterol levels Increased levels of abnormal lipoprotein a (2) Accumulations of lipoproteins (mainly LDL) in the vessel wall (3) Monocyte adhesion to the endothelium > migration into intima > transform into macrophages and foam cells Macrophages accumulate oxidized LDL > foam cells Modified LDL is toxic to endothelial cells, SM cells, and macrophages Binding and uptake stimulates inflammation cascade > release of growth factors, cytokines, and chemokines > recruit and activate more monocytes > monocytes release more ROS > oxidize more LDL (4) Platelet adhesion (5) Factor release from activated platelets, macrophages, and vascular wall cells > induce SM cell recruitment PDGF (released by locally adherent platelets, macrophages, endothelial cells, and SM cells) Fibroblast growth factor Transforming growth factor-α (6) SM cell proliferation, ECM production, and recruitment of T cells Convert a fatty streak into a mature atheroma > progressive growth of atherosclerotic lesion Growth factors stimulate SM cells to synthesize ECM > stabilizes atherosclerotic plaques (7) Lipid accumulation both extracellularly and within cells (macrophages and SM cells) Morphology Fatty streaks = lipid-filled foamy macrophages Atherosclerotic plaque = SM cells, macrophages, T cells + ECM + intra/extracellular lipid Most extensively involved vessels are the lower abdominal aorta, coronary arteries, popliteal arteries, internal carotid arteries, and vessels of circle of Willis Rupture, ulceration, or erosion of the surface of atheromatous plaques exposes highly thrombogenic substances and leads to thrombosis > occlude vessels Atheroembolism due to rupture of plaque > discharge debris into bloodstream Aneurysm formation due to atherosclerosis-induced pressure or ischemic atrophy of underlying media Consequences of Atherosclerotic Disease MI, cerebral infarction, aortic aneurysms, peripheral vascular disease Atherosclerotic Stenosis Small arteries = plaques can gradually occlude lumen > compromise flow > ischemic injury Critical stenosis = stage at which occlusion is severe enough to produce ischemia o Coronary = when 70% decrease in luminal cross-section > stable angina Lead to mesenteric occlusion and bowel ischemia, sudden cardiac death, chronic ischemic heart disease, ischemic encephalopathy, and intermittent claudication Acute Plaque Change Rupture/fissuring = expose highly thrombogenic plaque constituents Erosion/ulceration = expose thrombogenic subendothelial basement membrane to blood Hemorrhage into the atheroma = expanding its volume Plaques responsible for MI/acute coronary syndromes are asymptomatic until acute change Rupture when they can't withstand mechanical stresses generated by vascular shear forces Vulnerable plaques = contain large areas of foam cells and extracellular lipid, have thin fibrous caps, contain few SM cells, or have clusters of inflammatory cells Thrombosis Vasoconstriction Stimulated by (1) circulating adrenergic agonists, (2) locally released platelet contents, (3) endothelial cell dysfunction w/ impaired secretion of endothelial derived relaxing factors relative to contracting factors, and (4) mediators released from perivascular inflammatory cells Aneurysm and Dissection Aneurysm = localized abnormal dilation of a blood vessel or the heart (may be congenital or acquired) o Saccular = one side of vessels o Fusiform = both sides of vessel o False aneurysm = defect in vessel wall > extravasation of blood into extravascular CT > hematoma o Dissection = blood enters defect in wall and tunnels between its layers Pathogenesis of Aneurysms o Arterial walls are constantly remodeling to maintain their structural and functional integrity o Aneurysms can occur when the CT within the wall is compromised, as in: Intrinsic quality of the vascular wall CT is poor Marfan syndrome (defect in fibrillin > weird TGF-β activity & weakened elastic tissue) Loeys-Dietz syndrome (TGF-β receptor mutation > defective elastin & collagen I/III) Ehlers-Danlos syndrome (defective type III collagen) Scurvy (altered collagen cross-linking due to vitamin C deficiency) Balance of collagen degradation and synthesis is altered by inflammation/proteases Increased matrix metalloprotease (MMP) expression Decreased expression of tissue inhibitors of metalloproteases (TIMPs) Wall is weakened through loss of SM or synthesis of noncollagenous/nonelastic ECM Atherosclerotic thickening of intima > ischemia of the inner media Systemic HTN > narrowing of arterioles of vasa vasorum > medial ischemia Result in cystic medial degeneration o Two most important causes: atherosclerosis and HTN Atherosclerosis >> abdominal aortic aneurysms HTN >> ascending aortic aneurysms Abdominal Aortic Aneurysm o Atherosclerosis > weakens media > AAA o Most frequent in male smokers, rarely before age 50 o Morphology Usually below the renal arteries, above the bifurcation of the aorta Inflammatory AAA Occur in younger patients Present w/ back pain and elevated inflammatory markers (ex. C reactive protein) Characterized by abundant lymphoplasmacytic inflammation w/ many macrophages Caused by immune response to abdominal aortic wall (but NOT other aa.) Immunoglobulin G4 (IgG4)-related disease High plasma levels of IgG4 and tissue fibrosis associated w/ IgG4-expressing plasma cells May affect a variety of tissues (pancreas, biliary system, salivary gland) Aortitis and periaortitis weakens the wall sufficiently in some cases > aneurysm Responds well to steroid therapy Mycotic AAA Lesions that become infected by circulating microorganisms Suppuration further destroys the media > rapid dilation and rupture o Clinical Features Often asymptomatic until discovered incidentally on palpation Possible manifestations: Rupture into peritoneal cavity or retroperitoneal tissues (massive fatal hemorrhage) Obstruct vessels branching off the aorta > ischemic injury to supplied tissue Embolism from atheroma and mural thrombus Impingement on an adjacent structure (ex. ureter or erosion of vertebrae) Treatment: aneurysms >5cm are aggressively treated via surgical bypass or stents Thoracic Aortic Aneurysm o Associated w/ HTN (also Marfan syndrome and Loeys-Dietz syndrome) o Present w/: Respiratory difficulties due to encroachment on lungs and airways Difficulty swallowing due to compression of esophagus Persistent cough due to compression of recurrent laryngeal nn. Pain caused by erosion of bone (ribs and vertebrae) Cardiac disease as the aortic aneurysm leads to aortic valve dilation w/ valvular insufficiency Rupture Aortic Dissection o Blood separates the laminar planes of the media to form a blood-filled channel within the wall o Catastrophic if it ruptures through the adventitia > hemorrhages into adjacent spaces o May or may not be detectable as dilations radiologically o Occur in men 40-60yo w/ HTN, and younger adults w/ abnormalities of CT affecting the aorta (ex. Marfan) o Unusual in the presence of atherosclerosis or other medial scarring (ex. syphilis) b/c medial fibrosis inhibits propagation of the dissecting hematoma o Pathogenesis HTN is the major risk factor Ischemic injury to medial layer is contributory Also occurs in CT disorders (Marfan, Ehlers-Danlos, defects in copper metabolism) Trigger for the intimal tear is not known in most cases o Morphology Most frequent preexisting lesion = cystic medial degeneration Inflammation is characteristically absent Most spontaneous dissections occur in the ascending aorta (within 10cm of aortic valve) Rupture can reenter through 2nd tear if "lucky" but leads to development of chronic dissections o Clinical Features Most common (and dangerous) = proximal lesions (type A dissections) involving ascending and/or descending aorta DeBakey type I = ascending and descending aorta DeBakey type II = ascending aorta Distal lesions not involving the ascending part (type B dissections) being distal to subclavian a. DeBakey type III = descending aorta Classical symptoms: excruciating pain (begins in anterior chest > radiates to back between scapulae > moves downward as dissection progresses) Treated w/ anti-HTN medicine and surgery Vasculitis General term for vessel wall inflammation Due to immune-mediated inflammation or direct invasion of vascular walls by infectious pathogens Clinical features depend on which vascular bed is affected (CNS vs heart vs small bowel) Symptoms often include fever, myalgias, arthralgias, and malaise Noninfectoius Vasculitis o Immune Complex-Associated Vasculitis Seen in systemic immunologic disorders (ex. systemic lupus erythematosus) Associated w/ antibody production and immune complex deposition in vessels Also implicated in drug hypersensitivity vasculitis, and vasculitis secondary to infections o Antineutrophil Cytoplasmic Antibodies (ANCAs) Autoantibodies directed against neutrophil granules, monocyte lysosomes, and endothelial cells Anti-proteinase-3 (PR3-ANCA aka c-ANCA) PR3 = neutrophil azurophilic granule PR3-ANCA triggered by certain infections Associated w/ polyangiitis Anti-myeloperoxidase (MPO-ANCA aka p-ANCA) MPO = lysosomal granule constituent involved in ROS generation MPO-ANCA induced by several therapeutic agents (esp. propylthiouracil) Associated w/ microscopic polyangiitis and Churg-Strauss syndrome Mechanism for ANCA vasculitis: ANCAs react w/ cytokine-activated cells > direct injury to endothelial cells ANCAs activate neutrophils > injury by releasing granule contents and ROS o Antiendothelial Cell Antibodies Antibodies to endothelial cells induced by defects in immune regulation Related to Kawasaki Disease o Autoreactive T cells o Giant Cell (Temporal) Arteritis Most common form of vasculitis among older individuals Chronic inflammatory disorder of large to small-sized aa., principally affecting aa. in the head Especially the temporal arteries, but also vertebral and opthalmic aa. Opthalmic arterial involvement > abrupt to permanent blindness Can also involve the aorta (giant cell aortitis) Pathogenesis Stems from T-cell-mediated immune responses agaisnt vessel wall antigens Drive proinflammatory cytokine production (esp. TNF) Characteristic granulomatous response, correlation w/ MHC II haplotypes, and prompt therapeutic response to steroids Morphology Intimal thickening that reduces the luminal diameter Granulomatous inflammation of internal elastic lamina > elastic lamina fragmentation Clinical Features Rare before age 50 Symptoms may be vague (fever, fatigue, weight loss) or include facial pain or headache over the superficial temporal artery Ocular symptoms appear abruptly in 50% of pts Corticosteroids or anti-TNF therapies are effective o Takayasu Arteritis Granulomatous vasculitis of medium and larger arteries Characterized by ocular disturbances and weakening of the pulses in the upper extremities Transmural fibrous thickening of the aorta w/ severe stenosis of the major branch vessels Many similarities w/ giant cell arteritis (distinction is that Takayasu occurs in <50yo) Morphology Classically involves the aortic arch Pulmonary artery and coronary/renal arteries may be similarly affected Irregular thickening of vessel wall w/ intimal hyperplasia Clinical Features Initial symptoms are nonspecific (fever, weight loss, fatigue) Vascular symptoms (reduced bp and weak pulses in carotids and upper extremities) Ocular disturbances (visual defects, retinal hemorrhages, total blindness) Neurologic deficits Involvement of distal aorta > claudication of the legs Involvement of pulmonary artery > pulmonary HTN Involvement of coronary ostia > MI Involvement of renal aa. > systemic HTN o Polyarteritis Nodosa (PAN) Systemic vasculitis of small- or medium-sized muscular arteries Typically involves renal and visceral vessels, but sparing pulmonary circulation Associated w/ hepatitis B and depositions of HBsAg-HBsAb complexes Morphology Segmental transmural necrotizing inflammation of small/medium arteries Most often involves vessels of kidneys, heart, liver, and GI tract Inflammatory process weakens the arterial wall > can lead to aneurysm/rupture Acute phase accompanied by fibrinoid necrosis and possible luminal thrombosis Acute inflammatory infiltrate is replaced by fibrous thickening of vessel walls Clinical Features Typically a disease of young adults Clinical manifestations result from ischemia and infarction of affected tissues/organs Course is frequently remitting and episodic Classic presentation: rapidly accelerating HTN due to renal a. involvement, abdominal pain and bloody stools due to GI lesions, diffuse myalgias, and peripheral neuritis Immunosuppression effective in 90% of cases o Kawasaki Disease Acute febrile, usually self-limited illness of infancy and childhood Leading cause of acquired heart disease in children Associated w/ arteritis affected large to medium-sized, and even small vessels Predilection for coronary artery involvement that can cause aneurysms > rupture or thrombose Vascular damage mediated by activated T cells and monocytes/macrophages Morphology Resembles PAN (dense transmural inflammatory infiltrate and fibrinoid necrosis) Clinical Features Presents w/ conjunctival and oral erythema and blistering, edema of hands and feet, erythema of palms and soles, desquamative rash, and cervical lymphadenopathy 20% of untreated cases progress to cardiovascular sequelae Treatment w/ IV immunoglobulin and aspirin o Microscopic Polyangiitis Necrotizing vasculitis that affects capillaries and small arterioles/venules All lesions tend to be of the same age and are distributed widely Can affect skin, mucous membranes, lungs, brain, heart, GI tract, kidneys, and muscle Necrotizing glomerulonephritis and pulmonary capillaritis are especially common Pathogenesis Antibody responses to drugs, microorganisms, heterologous proteins, or tumor proteins Leads to immune complex deposition or generation of ANCAs Most cases associated w/ MPO-ANCAs Morphology Segmental fibrinoid necrosis of the media and focal transmural necrotizing lesions Lesions resemble PAN but spare mediums and large arteries Sometimes only dying infiltrating neutrophils are seen = "leukocytoclastic vasculitis" Little or no immunoglobulin found in most lesions = "pauci-immune injury" Clinical Features Features include hemoptysis, hematuria/proteinuria, bowel pain/bleeding, muscle pain/weakness, and palpable cutaneous purpura depending on location of lesion Immunosuppression works except in those w/ widespread renal or brain involvement o Churg-Strauss Syndrome (aka allergic granulomatosis and angiitis) Small-vessel necrotizing vasculitis associated w/ asthma, allergic rhinitis, lung infiltrates, peripheral hypereosinophilia, and extravascular necrotizing granulomata Lesions similar to PAN or microscopic polyangiitis, but w/ granulomas and eosinophils ANCAs (mostly MPO-ANCA) seen in 1/2 of cases Multisystemic: cutaneous (palpable purpura), GI bleeding, renal disease (glomerulosclerosis) Heart involved in 60% of pts > 1/2 of mortalities o Behcet Disease Small- to medium-vessel neutrophilic vasculitis Classically presents w/ recurrent oral aphthous ulcers, genital ulcers, and uveitis Can include GI and pulmonary manifestations Association w/ HLA-B51 and a cross-reactive immune response Immunosuppression w/ steroids or TNF-antagonist therapy generally effective o Granulomatosis w/ Polyangiitis (Wegener granulomatosis) Necrotizing granulomas of upper/lower respiratory tract Necrotizing or granulomatous vasculitis affecting small/medium vessels (lungs and upper airway) Focal necrotizing, often crescentic, glomerulonephritis Pathogenesis T-cell-mediated hypersensitivity response to inhaled microbes or environmental agents PR3-ANCAs present in 95% of cases Responds well to immunosuppression Morphology Upper respiratory tract lesions rimmed by granulomas w/ geographic patterns of central necrosis and accompanying vasculitis Necrotizing granulomas surrouned by zone of proliferating fibroblasts Renal lesions: focal and segmental necrotizing glomerulonephritis, crescentic glomerulonephritis Clinical Features Males affected more than females, w/ average age of 40yo Classical features: persistent pneumonitis w/ bilateral nodular and cavitary infiltrates, chronic sinusitis, mucosal ulcerations of nasopharynx, renal disease Other features: rashes, myalgias, articualr involvement, neural inflammation, and fever Treated w/ steroids, cyclophosphamide, and TNF antagonists > becomes relapsing/remitting instead of fatal (within 1 year if not treated) o Thromboangiitis Obliterans (Buerger Disease) Segmental, thrombosing, acute and chronic inflammation of medium/small arteries Principally tibial and radial arteries, w/ occasional extension into veins and nn. of extremities Occurs almost exclusively in heavy cigarette smokers, usually <35yo Pathogenesis Due to endothelial cell toxicity caused by tobacco or immune response to tobacco Most pts have hypersensitivity to intradermally injected tobacco extracts Prevalent in certain ethnic groups (Israeli, Indian, Japanese) Associated w/ particular HLA haplotypes Morphology Focal acute and chronic vasculitis of small/medium-sized arteries, mostly in extremities Thombus can contain small microabscesses (neutrophils surrounded by granulomata) Clinical Features Early manifestations = intermittent claudication, instep claudication, superficial nodular phlebitis (venous inflammation) Vascular insufficiency accompanied by severe pain, even at rest (neural involvement) Chronic extremity ulcerations develop > progress to gangrene Smoking cessation early on can prevent further attacks o Vasculitis Associated w/ Other Noninfectious Disorders Associated w/ rheumatoid arthritis, systemic lupus erythematous, malignancy, or systemic illness (mixed cryoglobulinemia, antiphosphilipid antibody syndrome, Henock-Schonlein purpura) Rheumatoid vasculitis affects small/medium-sized vessels > visceral infarction and aortitis Infectious Vasculitis o Due to direct invasion of infectious agents Bacteria = pseudomonas Fungi = aspergillus and mucos species o Can weaken arterial walls and culminate in mycotic aneurysms, or can induce thrombosis and infarction o Meningitis > vasculitis > infarction in brain Disorders of Blood Vessel Hyperreactivity Raynaud Phenomenon o Results from exaggerated vasoconstriction of arteries and arterioles in the extremities (esp. fingers/toes) o Induces paroxysmal pallor (cyanosis in extreme cases) o Digits show "red, white, and blue" coloration, proximal to distal o Primary Raynaud phenomenon Exagerrated central and local vasomotor responses to cold or emotion Predilection for young women Tends to affect extremities symmetrically Structural changes to vasculature is absent except in long-standing disease o Secondary Raynaud phenomenon Due to arterial disease (caused by SLE, scleroderma, Buerger disease, atherosclerosis, etc.) Tends to affect extremities asymmetrically Progressively worsens over time Myocardial Vessel Vasospasm (Cardiac Raynaud) o Excessive constriction of coronary arteries or myocardial arterioles > ischemia, or MI (if prolonged) o Due to intrinsic hyper-reactivity of medial SM cells or high levels of vasoactive mediators o Triggered by endognenous (epinephrine) or exogenous (cocaine/phenylephrine) factors o Elevated thyroid hormone can cause increased sensitivity to catecholamines o Can be triggered by stress (Takotsubo cardiomyopathy - broken heart syndrome) Veins and Lymphatics Varicose Veins o Abnormally dilated, tortuous veins produced by prolonged, inc. intraluminal pressure o Superficial veins of upper and lower leg are commonly involved o Obesity and pregnancy increase risk due to mass effect impeding venous drainage o Clinical Features Incompetence of venous valves > stasis, congestion, edema, pain, and thrombosis Secondary tissue ischemia results from chronic venous congesteion > "stasis dermatitis" Embolism from these superficial veins is rare (compared to DVT from deep veins) o Other sites: Esophageal varices Due to liver cirrhosis, portal vein obstruction, or hepatic vein thrombosis Portal HTN > opening of portosystemic shunts > inc. blood flow into veins o Esophageal junction = esophageal varices o Rectum = hemorrhoids o Abdomianl wall = caput maedusa Esophageal varices most important since they can lead to massive upper GI hemorrhage Hemorrhoids Prone to bleeding, thrombosis, and painful ulcerations Thrombophlebitis and Phlebothrombosis o Interchangeable designations for venous thrombosis and inflammation o Involvement of deep leg veins accounts for >90% of cases (DVT) o Prolonged immobilization resulting in venous stasis is the most important risk factor for DVT o Systemic hypercoagulability, including genetic syndromes, often also play a role o Pulmonary embolism is the most common serious complication of DVT (often the first manifestation) Superior and Inferior Vena Cava Syndromes o Superior Vena Cava Syndrome Caused by neoplasms that compress or invade the SVC Bronchogenic carcinoma or mediastinal lymphoma Obstruction produces marked dilation of veins of head, neck, and arms w/ cyanosis Pulmonary vessels can be compressed > respiratory distress o Inferior Vena Cava Syndrome Neoplasms that compress or invade the IVC or thrombosis of hepatic/renal/lower extremity vv. Hepatocellular carcinoma or renal cell carcinoma Induces marked lower extremity edema, distention of superficial collateral veins of lower abdomen, and massive proteinuria (w/ renal involvement) Lymphangitis and Lymphedema o Lymphangitis Acute inflammation elicited by spread of bacterial infection into lymphatics (commonly by GAS) Affected lymphatics are dilated and filled w/ neutrophil/monocyte exudate Manifested by red, painful subcutaneous streaks, and lymphadenitis (painful enlargement) o Primary Lymphedema Due to isolated congenital defect, or as Milroy disease o Secondary Lymphedema Obstructive lymphedema from blockage of previously normal lymphatics Due to malignant tumors, surgical procedures, postirradiation fibrosis, filariasis, postinflammatory thrombosis and scarring o Persistent lymphedema leads to deposition of interstitial CT > peau d'orange in overlying skin o Rupture of dilated lymphatics > accumulation of lymph (chylous ascites, chylothorax, chylopericardium) Vascular Tumors Benign Tumors and Tumor-Like Conditions Typically form obvious vascular channels lined by normal-appearing endothelial cells o Vascular Ectasias Ectasia = local dilation of a structure Telangiectasia = permanent dilation of preexisting small vessels > discrete red lesion NOT true neoplasms Nevus flammeus ("birthmark") Most common form of vascular ectasia Light pink to deep purple flat lesion on head or neck composed of dilated vessels Most regress spontaneously Port wine stain Special form of nevus flammeus Tend to grow during childhood, thicken the skin surface, and don't fade over time Distribution in the trigeminal nerve regions associated w/ Sturge-Weber syndrome o Associated w/ ipsilateral venous angiomas, mental retardation, seizures, hemiplegia, and skull radio-opacities Spider telangiectasias Nonneoplastic vascular lesions resembling a spider Commonly occur on face, neck, or upper chest Associated w/ hyperestrogenic states (pregnancy or liver cirrhosis) Hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu disease) Mutations in genes encoding components of TGF-β signaling Widely distributed over skin and oral mucous membranes, as well as in respiratory, GI, and urinary tracts Can spontaneously rupture > serious epistaxis, GI bleeding, or hematuria o Hemangioma Very common tumors Increased number of vessels filled w/ blood Most present from birth and increase in size, but eventually regress Typically confined to head or neck, but can occur internally Capillary hemangiomas Most common type Occur in the skin, subcutaneous tissues, and mucous membranes of oral cavities/lips, as well as liver, spleen, and kidneys Composed of thin-walled capillaries w/ scant stroma Juvenile hemangiomas ("strawberry type" hemangiomas) Extremely common in newborns Arise in skin and grow rapidly for a few months Fade by 1-3 years and completely regress by 7 years in most cases Cavernous hemangiomas Large, dilated vascular channels More infiltrative, frequently involving deep structures Don't spontaneously regress Intravascular thrombosis and dystrophic calcification are common Can be locally destructive > some may require surgery Component of von Hippel-Lindau disease Pyogenic granulomas Capillary hemangiomas Rapidly growing red pedunculated lesions on skin, gingival, or oral mucosa Bleed easily and are often ulcerated Curettage and cautery is usually curative o Lymphangiomas Benign lymphatic counterpart to hemangiomas Simple (capillary) lymphangiomas Slightly elevated, sometimes pedunculated, up to 1-2cm Occur primarily in the head, neck, and axillary subcutaneous tissue Network of endothelium-lined spaces Cavernous lymphangiomas (cystic hygromas) Typically found in neck or axilla or children Can reach up to 15cm Common in Turner syndrome Massively dilated lymphatic spaces lined by endothelial cells o Glomus Tumor (Glomangioma) Benign but exquisitely painful Arise from modified SM cells of the glomus bodies (arteriovenous structures involved in thermoregulation) Superficially resemble hemangiomas, but arise from SM cells instead of endothelial cells Most common in distal portion of the digits, especially under the fingernails o Bacillary Angiomatosis Vascular proliferation in immunocompromised hosts Caused by opportunistic gram-negative bacilli of Bartonella family Bartonella henselae: cat-scratch disease, cats are reservoirs Bartonella quintana: trench fever, transmitted by rice Can involve the skin, bone, brain, and other organs Skin lesions are red papules and nodules, or rounded subcutaneous masses Infection and lesions are cleared by macrolide antibiotics (ex. erythromycin) Intermediate-Grade (Borderline) Tumors o Kaposi Sarcoma Vascular neoplasm caused by human herpesvirus 8 (HHV8) Highly associated w/ AIDS Classic KS Older men of Mediterranean, Middle Eastern, or Eastern European descent (Ashkenazic Jews) Multiple red-purple skin plaques or nodules Usually in distal lower extremities Progressively increase in size and number and spread proximally Typically asymptomatic and remain localized to the skin and subcutaneous tissue Endemic African KS Involves lymph nodes much more frequently than classical variant Most common tumor in central Africa Severe form exists in prepubertal children (100% mortality within 3 years) Transplant-associated KS Occurs in solid organ transplant recipients in setting of T-cell immunosuppression Aggressive course that involves lymph nodes, mucosa, and viscera Cutaneous lesions may be absent Lesions regress w/ attenuation of immunosuppression, but at risk of organ rejection AIDS-associated (epidemic) KS AIDS-defining illness Most common HIV-related malignancy Often involves lymph nodes and disseminates widely to viscera early on Pathogenesis Virtually all KS lesions are infected by HHV8 HHV8 and altered T-cell immunity are required for KS development Morphology Classic KS cutaneous lesions progress through 3 stages: Patches: red/purple macules confined to distal lower extremities Raised: lesions spread proximally and become larger o Nodular: associated w/ nodal and visceral involvement in African and AIDS-associated KS Clinical Features Surgical excision is usually enough for early classic KS Radiation can be used for multiple lesions Chemotherapy for more disseminated disease, including nodular involvement Stopping imunosuppression treatment often effective for transplant-associated KS Anti-retroviral therapy effective in AIDS-associated KS Hemangioendothelioma Vascular neoplasms w/ characteristics between benign hmangiomas and anaplastic angiosarcomas Epithelial hemangioendothelioma Vascular tumor of adults occuring around medium/large-sized veins Most cured by excision, but 40% recur, and 20-30% metastesize Malignant Tumors o More often solid and cellular, exhibiting cytologic atypia and lacking well-defined vessels o Angiosarcoma Malignant endothelial neoplasm that primarily affects older adults May occur at any site, but most often involves skin, soft tissue, breast, and liver Hepatic angiosarcoma associated w/ carcinogens (arsenic, Thorotrast contrast agent, polyvinyl chloride) Arise in setting of lymphedema, classically in ipsilateral upper extremity, from lymphatic vessels Locally invasive and can readily metastasize Morphology Cutaneous angiosarcoma begin as multiple small, asymptomatic red papules/nodules Eventually become large, fleshy masses w/ central necrosis and hemorrhage All degrees of differentiation can be seen Endothelial origin can be demonstrated by staining for CD31 or von Willebrand factor o Hemangiopericytoma Tumors that arise from pericytes Pathology of Vascular Intervention Largely recapitulate changes that occur in setting of any vascular insult > stereotypical healing responses Endovascular Stenting o Arterial stenoses (esp. coronary arteries) can be dilated by inflating a balloon catheter to sufficient pressures in order to rupture the occluding plaque (balloon angioplasty) o Arterial dissection is also induced, but hopefully limited o Abrupt reclosure can occur as a result of compression of the lumen by extensive circumferential or longitudinal dissection, vessel wall spasm, or by thrombosis o 90% of procedures now involve angioplasty and concurrent coronary stent placement to avoid this o However, thrombosis is an important post-stenting complication > pts must receive antithrombotic agents o Long-term success limited by development of proliferative in-stent restenosis (intimal thickening due to SM cell ingrowth > occlusion) o Drug-eluting stents designed to avoid this complication by giving off drugs to block SM cell activation Vascular Replacement Large-bore synthetic conduits function well in high-flow locations (ex. aorta) Small-diameter artificial grafts generally fail as a result of early thrombosis or late intimal hyperplasia Small-diameter grafts are therefore fashioned from saphenous veins or left internal mammary aa. o 50% of saphenous vein grafts are still patent at 10 years o 90% of internal mammary aa. are still patent at 10 years