Os odontoideum. Antônio Santos de Araújo Jr.1, Pedro Alberto
advertisement

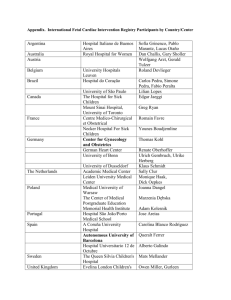
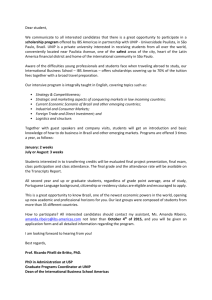
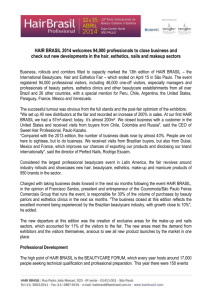
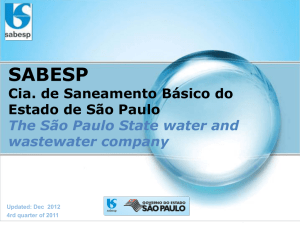
Os odontoideum. Antônio Santos de Araújo Jr.1, Pedro Alberto Arlant1, Arnaldo Salvestrini Jr.1, Orlando Parise2, Paulo Roberto Lazarini3, Carlo Domenico Marrone4, Mirella Martins Fazzito5, Raphael R. Pratali6, Edison Luis Dezen6, Marcelo Bordalo Rodrigues7. 1. Neurosurgeon, Sírio Libanês Hospital, São Paulo, Brazil 2. Head and neck surgeon, Sírio Libanês Hospital, São Paulo, Brazil 3. Ear, nose and throat surgeon, Sírio Libanês Hospital, São Paulo, Brazil 4. Neurophysiologist, Ricardo Ferreira Neurophysiology Clinics, São Paulo, Brazil 5. Neurologist, Sírio Libanês Hospital, São Paulo, Brazil 6. Orthopedist, Sírio Libanês Hospital, São Paulo, Brazil 7. Spine radiologist, Sírio Libanês Hospital, São Paulo, Brazil Abstract Introduction: ‘Os odontoideum’ is a rare craniovertebral junction (CVJ) disease that presents itself as a dystopic ossicle from a hypoplastic C2 dens, contributing to a craniocervical instability. Objective and Methods: We report a 45-year old woman harboring a dystopic ‘os odontoideum’, who sustained a progressive neurological deterioration with marked circumferential spinal cord compression. She was submitted to a prior posterior suboccipital craniectomy with occipitocervical fixation, followed by an anterior transoral transpharyngeal odontoidectomy. Results and Discussion: Both procedures were performed uneventfully, and the patient had a remarkable improvement afterwards. We believe that our step-wise surgical management to ‘os odontoideum’ is feasible and accomplishes excellent outcomes. Key Words: Os odontoideum, craniocervical instability, craniovertebral junction diseases. Antônio Santos de Araújo Júnior Correspondence Address: Rua Peixoto Gomide, 515, cj 96, Cerqueira César, São Paulo, São Paulo, Brazil. CEP 01409-001. Phone/Fax: 05511-32890411 Cel: 05511-84567404 Email: dr.antonioaraujojr@gmail.com; Website: araujoefazzito.com.br Introduction ‘Os odontoideum’ was first described by Giacomini in 18861. ‘Os odontoideum’ is radiographically defined as an isolated ossicle with smooth circumferential cortical margins and no osseous continuity with the body of C2 2. It represents an uncommon craniovertebral junction (CVJ) abnormality that exists as a separate ossicle apart from a hypoplastic C2 dens 3. Anatomically, there are two types of ‘os odontoideum’: the orthotopic and the dystopic one 4. Orthotopic refers to an ossicle that moves with the anterior arch of C1 and that can be reduced in a normal alignment with the dens 4. Dystopic means an ossicle that has migrated toward the clivus and that is functionally fused to the basium, sometimes it may be even dislocated anteriorly to the C1 arch 4. Since ‘os odontoideum’ is a rare lesion its pathogenesis is controversial. Some authors suggest that it is congenital, while others believe that it is a result of remote trauma with a chronic nonunited fracture of the odontoid process 2. Some evidences support both etiologies. According to the congenital hypothesis, the incomplete ossification across the vestigial intervertebral disc separating the odontoid process from the body of the axis (a cartilage known as a ‘neurocentral synchondrosis’) would be responsible for the formation of the ossicle 4. A familial case of ‘os odontoideum’ with an autosomal dominant pattern of inheritance5, and a report of identical twins sisters with ‘os odontoideum’ 6 support this theory. Proponents of the traumatic hypothesis suggest an unrecognized odontoid type II fracture followed by avascular necrosis and osseous remodeling as the cause of os odontoideum 4. This remodeling makes ‘os odontoideum’ indistinguishable from an old nonunion type II odontoid fracture 2,4. This theory is sustained by the fact that previous history of trauma is observed in a majority of patients. Biomechanics Regarding its biomechanics, craniovertebral junction (CVJ) may be divided in two motion segments, with different mechanical properties. The mechanical properties of ‘occiput-C1’ are largely determined by bony elements, while those of the C1-C2 segment are largely determined by ligamentous elements 7. The primary movement at Oc-C1 is flexion and extension, while the primary movement at C1-C2 is axial rotation. Rotational movement is limited by C1-C2 articulation, the contralateral alar ligament, the capsular ligaments, and last but not the least by the ipsilateral transverse ligament 7. By its time, translational motion is prevented by the transverse ligament trapping the intact odontoid process within the anterior arch of C1 2. ‘Os odontoideum’ compromises the integrity of the odontoid-transverse ligament complex, leading consequently to atlantoaxial instability. This instability results in translation of the C1 vertebra and ‘os’ relative to C2 2. During flexion motion, anterolisthesis of the C1-os complex in relation to C2 may compress the spinal cord against the posterior arch of C1. During extension, posterior subluxation of the C1-os complex may compress anteriorly the spinal cord. Therefore, the instability produced by os odontoideum is biomechanically identical to the atlantoaxial instability seen in a Type II odontoid fracture 2. Case report We report a 45 year-old woman, housewife, who presented with a 2 years history of constant neck pain associated with gait disturbance and intermittent upper-extremity paresthesias. According to her, all symptoms had worsened after an unwitnessed fall to ground, just after an inadverted neck flexion. After that episode, she sustained progressive upper and lower limbs weakness. At first evaluation, neurological examination revealed a disproportionate spastic tetraparesis, with crural predominance, and obvious signs of cervical myelopathy (hyperactive deep tendon reflexes, Hoffmann’s, Babinski and Lhermitte’s signs). She was promptly submitted to plain radiographies, CT and MRI scans, and diagnosed as harboring a dystopic ‘os odontoideum’ (Figure 1). On further dynamic craniocervical radiographies, the CVJ instability was obvious. C1 Os C2 Os C1 C2 B A C D Figure 1: ‘Os odontoideum’ image diagnosis. (A) Sagital computed tomography (CT), bone window, showing altered CVJ with three bone segments, tubercle of C1, Os and C2; (B) Axial bone CT, revealing the relationship between the three segments; (C) Sagital T2 weighted magnetic resonance image (MRI), marked anterior and posterior spinal cord compression; (D) Sagital T2 MRI, myelomalacia secondary to severe spinal cord compression. Before the first surgical procedure, the patient experienced a progression of her myelopathic symptoms. In order to alleviate the cord compression and stabilize the CVJ, it was proposed a posterior approach with suboccipital craniectomy, C1 and C2 laminectomy, duroplasty, and occipitocervical fixation, with intraoperative somatosensitive evoked potential (SSEP) monitoring. During this procedure an attempted occiput to C1-C2 transarticular screws fixation was not feasible, because the SSEP alterations after alignment. In view of it, occiput to C2-C3 lateral mass screws fixation was then performed with intraoperatively gains in SSEP. Postoperatively, the patient was symptoms-free, with regained motor and sensory functioning, and a normal gait. She gradually recovered normal daily activities, with full extremities coordination, despite some limitation of neck mobility. On further postoperative CT and MRI scans, posterior decompression was satisfactory, instead our concerns about anterior compression (Figure 2). B A C D E Figure 2: Postoperative images after posterior decompression and occipitocervical fixation (OCF). (A) Lateral CT reconstruction, showing screws and rods from OCF; (B-C) Posterior CT reconstruction, revealing lateral limits from suboccipital craniectomy; (D) Sagital CT image, bone window, superior and inferior margins from decompression, including C1 and C2 laminectomy; (E) Axial bone CT scan, C1 posterior arch removal. One year after the first procedure, this patient started to complain of recurrent right arm and left leg weakness. At this time, progressive paresis was noticed associated two months later to a swallowing problem and hoarseness. At hospital admission, neurological examination revealed severe motor impairment, tetraparesis with strength grade 0/V in right arm, 4/5 in left arm, 4/5 in right leg, and 3/5 left leg, tetraparesthesia and lower cranial nerves signs. Transoral-transpharyngeal approach was then proposed under a neuronavigation protocol (Figure 3). A multidisciplinary surgical team was conveyed to handle this unusual surgical problem. Laryngeal fibroscopy intubation was performed. Monitoring devices were connected, in followed by tracheostomy. Transoral- transpharyngeal approach, crossing the soft palate, was accomplished by our ENT surgeon. Neurosurgeons, under microscopic magnification, performed a C1, Os and C2 osteotomy with high-speed drill (Medtronic Midas Rex, Fort Worth, Texas, U.S.A.) under real-time neuronavigation (BrainLab VectorVision Neuronavigation System, Heimstetten, Germany). Bone drilling was advanced up to the duramater level. Internal cortical bone from C2 was removed with 1 mm Kerrison rongeur up to reestablishment of normal duramater pulsation. Just after, SSEP from all limbs were normalized. A B C Figure 3: (A) Preoperative neuronavigation: C1 tubercle and odontoid process are targeted; (B)Intraoperative neuronavigation, real-time drill monitoring while resecting C1 Intraoperative tubercle; (C) neuronavigation, drilling at the tip of odontoid process. Postoperatively patient evolved once more assymptomatic, with complete recovering of sensorimotor deficits, with mild velopharyngeal insufficiency, nasal regurgitation and nasal quality of the voice during speech. Tracheostomy was closed after three days. Nasoenteric feeding tube was removed by the 5th postoperative day, with normal swallowing. Postoperative MRI scans were performed (Figure 4). Patient was discharged by the 8th postoperative day. A B C Figure 4: MRI scan after transoral transpharyngeal odontoidectomy. (A-B) Sagital T2 weighted MRI, showing extension from the C1, Os and C2 osteotomy; (C) Anterior decompression accomplished, without much lateral bone removal. Discussion ‘Os odontoideum’ is a rare craniocervical disease, with harmful consequences over the craniovertebral junction. Patients can present with whole gamut of neurological symptoms 4. It is reported that even minor trauma can result in severe neurological injury and may result in sudden death 2. Standard plain radiographies are sufficient to diagnose this condition, but the advent of MRI has improved its precision, revealing in details the spinal cord compromise. Assymptomatic patients should be followed closely, while every patient with unstable or compressive disease should be offered surgery 4. Surgical indication should be tailored according to the patient’s status, and respecting the surgical team experience. We believe that circumferential spinal cord compression by ‘os odontoideum’ can be first managed via the posterior route (suboccipital craniectomy, C1 and C2 laminectomy, and duroplasty), with C1-C2 or occipitocervical fixation in the same surgical stage. Most neurosurgeons are very familiar with this approach, with minimal morbidity and high successful rates of complete fusion. After the first procedure, closely follow-up is mandatory to identify impending neurological deterioration. Since symptoms progress despite posterior decompression, anterior approach should not be postponed. A multidisciplinary surgical team, with neurosurgeons and ENT- head and neck surgeons, is indispensable to best perform the transoral transpharyngeal approach to the upper cervical spine. Conclusion We believe that this step-wise surgical management to ‘os odontoideum’ is feasible and reasonable. It accomplishes favorable neurological prognosis with minimal intraoperative morbidity, as shown in our case. Despite its potential severity, ‘os odontoideum’ is a treatable disease. Surgery may allow patients to return early to normal daily activities, with excellent outcomes. References 1. Giacomini C. Sull’ esistenza dell’ ‘os odontoideum’ nell’ uomo. Gior Accad Med Torino. 1886;49:24-28. 2. Klimo P Jr, Kan P, Rao G, Apfelbaum R, Brockmeyer D. Os odontoideum: presentation, diagnosis, and treatment in a series of 78 patients. J Neurosurg Spine. 2008;9(4):332-42. 3. Menezes AH. Pathogenesis, dynamics, and management of os odontoideum. Neurosurg Focus. 1999;15(6):e2. 4. Arvin B, Fournier-Gosselin MP, Fehlings MG. Os odontoideum: etiology and surgical management. Neurosurgery. 2010;66(3 Suppl):22-31. 5. Morgan MK, Onofrio BM, Bender CE. Familial os odontoideum. Case report. J Neurosurg. 1989;70(4):636:639. 6. Kirlew KA, Hathout GM, Reiter SD, Gold RH. Os odontoideum in identical twins: perspectives on etiology. Skeletal Radiol. 1993;22(7):525527. 7. Steinmetz MP, Mroz TE, Benzel EC. Craniovertebral junction: biomechanical considerations. Neurosurgery. 2010;66(3 Suppl):7-12.