1st - 6th Grade 2015-2016 Registration Form
advertisement

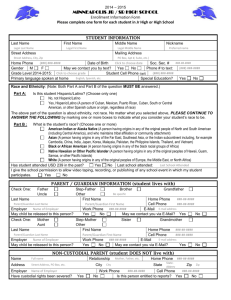
The Park District of La Grange Before and After School Recreational Experience 2015-16 Registration / Emergency Form 1ST – 6TH Grade Only CHILD’S HOME SCHOOL_________________ Student’s Legal Name________________________________________ Address___________________________________________________ Please indicate choice: Home Phone _______________________Cell Phone_______________ 1). Before School Care (____) (7:00-8:15 a.m. M-F) ( ) Male ( ) Female *Birth date _________ *Age_______Grade_______ 2). After School Care (3:15-6:00 p.m. M-F) (2:30-6:00 p.m. W) PLEASE WRITE LEGIBLY In order to provide the best care for your child, please answer the following: (____) 3). Before and After School (____) Does your child have any health or dietary problems that may affect his/her activities or diet (e.g. epilepsy, rheumatic fever, diabetes, allergies, heart trouble etc.)? Yes___ No___ If yes, please attach a separate explanation with details. Registration for 1st- 6th Grade Fee $30.00 per child Does your child have any special needs or is your child receiving any special services from school or other agencies? Yes___ No___ If yes, please attach a separate explanation with details. Make checks payable to: Park District of La Grange No Cash Accepted NO REFUNDS Father’s Name______________________________ _______ Employer______________________________ Email_____________________________________________ Work Phone __(____)____________________ Pre- Mother’s Name_____________________________ ________ Employer _____________________________ Email______________________________________ ____ Work Phone __(____)_______________________ Guardian __________________________________ ________ Employer _____________________________ Email__________________________________ ________ Work Phone _______________________________ Child resides with: both parents____ mother____ father____ other____________ In addition to those listed above, in case of an emergency, we have your permission to contact and or release your child(ren) to: Name _______________________________Phone ____________________ Relationship__________________ Name _______________________________Phone ____________________ Relationship__________________ Name _______________________________Phone ____________________ Relationship__________________ Name _______________________________Phone ____________________ Relationship__________________ Doctor’s Name / phone _______________________________________Hospital Preference_________________ *IF ANY INFO CHANGES, PLEASE NOTIFY THE BASE SUPERVISOR. _____________________________ Signature of Parent/ Guardian _______________ Date Note- Students may begin BASE after their information is reviewed and verified Parents will receive an email confirmation 5/22/15