Synergistic effects of low-level laser and mesenchymal stem cells on
advertisement

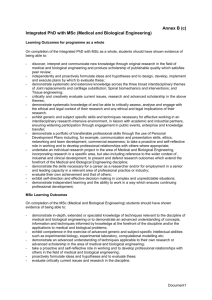
Synergistic effects of low-level laser and mesenchymal stem cells on functional recovery in rats with crushed sciatic nerves Chen-Chia Yang1, John Wang2, Shyh-Chang Chen2, Yueh-Ling Hsieh3* 1 Department of Physical Medicine and Rehabilitation, Taichung Tzu Chi General Hospital, Taichung 42743, Taiwan 2 Department of Pathology and Laboratory Medicine, Taichung Veterans General Hospital, Taichung 40705, Taiwan 3 Department of Physical Therapy, Graduate Institute of Rehabilitation Science, China Medical University, Taichung 40402, Taiwan Yang CC and Wang J contributed equally to this work. *Correspondence to: YL. Hsieh, Department of Physical Therapy, China Medical University, #91, Hsueh-Shih Road, Taichung 40402, Taiwan. Tel: 886-4-22053366 ext. 7312; Fax: 886-4-22065051; E-mail: sherrie@mail.cmu.edu.tw 1 Short title: Combination of laser and stem cells for peripheral nerve injury This study was supported by the National Science Council of Taiwan (Grant number: NSC 96-2314-B-039-029-MY3) and China Medical University (Grant number: CMU100-S-07). . No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit upon the authors or upon any organization with which the authors are associated. 2 Abstract Mesenchymal stem cells (MSC) transplantation has been proposed to exert beneficial effects on peripheral nerve regeneration after a peripheral nerve injury, but the functional recovery in the denervated limb is still limited. In this study, we used low-level laser therapy (LLLT) as an adjunct therapy for MSC transplantation on functional recovery of crushed sciatic nerve in rats. Peripheral nerve injury was induced in 48 Sprague-Dawley rats by crushing the unilateral sciatic nerve using a vessel clamp. The animals with crushed injury were randomly divided into four groups: Control group, with no treatment; MSC group, treated with MSC alone; LLLT group, treated with LLLT alone; and MSCLLLT group, treated with combination of MSC and LLLT. Sciatic function index (SFI), vertical activity of locomotion (VA), ankle angle (AA) of rats were examined for functional assessments after treatments. Moreover, electrophysiological, morphological and S100 immunohistochemical studies were also conducted. The MSCLLLT group showed a greater recovery in SFI, VA and AA, with significant difference from MSC, LLLT and control groups (p < 0.05). Moreover, markedly enhanced electrophysiological function and expression of S100 immunoreactivity, as well as less inflammatory cells and vacuoles formation were also demonstrated after nerve crush injury in the MSCLLLT group when compared with the groups receiving a single treatment (p < 0.05). MSC transplantation combined with 3 LLLT could achieve better results in functional recovery than a conventional treatment of MSC or LLLT alone. LLLT has a synergistic effect in providing greater functional recovery with MSC transplantation after nerve crush injury. Keywords: nerve regeneration; functional recovery; mesenchymal stem cell; low-level laser therapy; nerve crush injury; synergistic effect 4 1. Introduction Injuries of peripheral nerves are common and debilitating, resulting in considerable long-term disability (Noble et al., 1998). While regeneration of peripheral nerves may eventually occur, it is slow and frequently incomplete, misdirected, or associated with debilitating neuropathic pain (Navarro et al., 2007). Understandably, therefore, numerous attempts have been made to enhance and/or accelerate the recovery of injured peripheral nerves. Stem/precursor cells from different sources are being studied for their potential application in the scenario of peripheral nerve injury. Transplant cells, the most promising candidate, are derived from easily accessible sources, such as embryonic, neural and mesenchymal stem cells (MSCs). They have all demonstrated to act as a nerve guide and direct the outgrowing nerve fibers towards the distal nerve stump, and have been proposed to exert beneficial effects on peripheral nerve regeneration (Cho et al., 2011, Murakami et al., 2003, Pan et al., 2006, Pan et al., 2007). Although regimens of stem cell implantation can elicit functional recovery following peripheral nerve injury, the extent of outcome is still limited after such a lesion. Many experimental and clinical studies have reported the positive effects of low-level laser therapy (LLLT) on peripheral nerve regeneration by promoting the repair processes of peripheral nerves (Gigo-Benato et al., 2005, Gigo-Benato et al., 5 2010, Rochkind 2009, Rochkind et al., 2009). Animal studies showed that LLLT has a protective effect on maintenance of functional activity of the injured nerve, decreases scar tissue formation at the injury site, reduce degeneration in corresponding motor neurons of the spinal cord, and increases significantly axonal growth and Schwann cell proliferation (Gigo-Benato et al., 2004, Rochkind 2009, Rochkind et al., 1990, Shamir et al., 2001, Van Breugel and Bar 1993, Wollman et al., 1996). Numerous therapeutic interventions, mostly pharmacotherapeutic, have been tested to evaluate their effects on functional recovery of peripheral nerve injury in combination with either stem cell transplantation therapy (Pan et al., 2007, Pan et al., 2009a, Pan et al., 2009b). Few investigations have been made to explore the possibility of applying LLLT combined with stem cell therapy for such a peripheral nerve lesion. In this study, we investigate the usage of combined methods of LLLT to enhance the outcome of MSC transplantation on nerve repair. The main objective is to examine whether LLLT has a synergistic effect in providing greater functional recovery with transplantation of MSC after nerve crush injury. Our hypothesis is that MSC transplantation combined with LLLT will yield greater improvement in function than MSC therapy alone. 2. Materials and Methods 6 2.1. General design To observe the synergistic effects of LLLT and MSC transplantation on functional recovery of crushed sciatic nerve, all rats (n = 48) received unilateral sciatic nerve crush injury. They were then randomly divided into four groups: (1) the MSCLLLT group (n = 12) comprising injured animals transplanted with MSC and receiving LLLT, (2) the MSC group (n = 12) comprising injured animals transplanted with MSC and receiving sham-operated LLLT; (3) the LLLT group (n = 12) comprising injured animals receiving non-MSC culture media but with LLLT applied; and (4) the non-treated control group (n = 12) comprising injured animals receiving non-MSC culture media and sham-operated LLLT. Assessments of functional recovery included serial changes in sciatic function index (SFI), vertical activity of locomotion (VA), and ankle angle (AA) measured at the conditions before (pre-op), after surgery (post-op), and at four weekly post-treatment (post-tr) timepoints, i.e., immediately and 1-3 weeks after ceasing treatment (0wpost-tr, 1wpost-tr, 2wpost-tr, and 3wpost-tr, respectively). Electrophysiological evaluations were performed at the conditions of post-op (10 hours after surgery), 0wpost-tr and 3wpost-tr (immediately after treatment and end of the experiment). The rats were sacrificed after completion of electrophysiological studies on the final day of the four-week period for analysis of nerve morphology. The experimental design and experimental groups are shown in Figure 1. 7 2.2. Animal model ® Adult male Sprague-Dawley rats (CD (SD) IGS BR; purchased from BioLASCO Taiwan Co., Ltd., Taipei, Taiwan) weighing 250 to 300 g were individually housed in a 12/12 h light/dark vivarium with food and water ad lib. All experimental procedures were approved by the Committee on Animal Care and Use of China Medical University. Animals were anesthetized with 4% isoflurane (AErrane, Baxter Healthcare of Puerto Rico, Guayama, Puerto Rico) in induction, followed by a 1-2% maintenance dose. Body temperature during anesthesia was stabilized by placing the rats on an electric warming pad. All rats received unilateral sciatic nerve crush. The hindlimbs of anesthetized rats were shaved and cleaned with povidone-iodine solution. By using a double-headed operative microscope, the sciatic nerve on one randomly selected side was exposed by skin incision along the femur and separation of biceps femoris and superficial gluteal muscles. A vessel clamp (B-3; pressure, 1.5 g/mm2; S&T Marketing LTD, Neuhausen, Switzerland) was applied 10 mm from the internal obturator canal for 20 minutes. The crush site was sutured with 9-0 nylon over the epineuria as a mark. Then 0.2 ml of collagen gel medium containing MSC cells was injected close to the crush site of nerve with a microsyringe. The wound of muscle layers and skin were then sutured with 4/0 reabsorbable suture (Ethicon, Cornelia, GA) to allow recovery. 8 Non-MSC-transplanted animals underwent the same procedures but injected with 0.2 ml of culture media that contained no MSC. 2.3. Preparation and graft of rat mesenchymal stem cells MSCs isolated from rat bone marrow and cryopreserved at the second passage were purchased from Cell Applications Inc. (San Diego, CA). These MSCs were induced to differentiate into Schwann-like cells according to previous studies with a modified protocol (Dezawa et al., 2001; Murakami et al., 2003; Pan et al., 2006). The cells were then centrifuged and plated in rat MSC growth medium (RMSCGM, R419-500, Cell Applications Inc. San Diego, CA) supplemented with 10% fetal bovine serum (FBS, Invitrogen. Grand Island, NY), 100 U/ml penicillin (Invitrogen. Grand Island, NY), and 100 μg/ml streptomycin (Invitrogen. Grand Island, NY). The cells were passed or were supplied with differentiation medium containing 1.5% of DMSO and 2.5% of FBS once they reached 60% confluence, mostly 24 hours after plating (and before the rats’ surgery). The passage cells were used for in vivo transplantation after in vitro transdifferentiation. MSCs treated with beta-mercaptoethanol followed by retinoic acid and then incubated with Schwann cell induction medium consisted of consisted of α-MEM (Invitrogen. Grand Island, NY), 10% FBS, 5 Y, forskolin (Sigma-Aldrich, Inc. St. Louis, MO), 4 ng/ml recombinant human basic fibroblast growth factor (b-FGF, 9 R&D System, Minneapolis, MN), 200 ng/ml recombinant human heregulin-beta1 (Her-m1, Sigma-Aldrich, Inc. St. Louis, MO) and 5 ng/ml recombinant human platelet derived growth factor-AA (PDGF-AA, PeproTech Inc, Rocky Hill, NJ) for 1 week. As soon as the transdifferentiation process was finished, 1 × 105 MSC cells were placed in 0.2 ml of collagen gel medium. The cells were suspended evenly by repeated flushing using a micropipette. A volume of 0.2 ml of MSCs embedded in collagen gel was infused into the crush site using a micropipette. 2.4. Low-level laser irradiation Twelve hours after surgery, a continuous 660-nm Ga-Al-As diode laser (Aculas-Am series, Multi-channel LLLT system; Konftec Corporation, Taipei, Taiwan) was used in this study. The conditions and parameters of LLLT were performed as previously described with modification (Hsieh et al. 2012). Briefly, after sterilization, the hand-held delivery probe was lightly placed on the skin surface of rat’s thigh directly above the crush sciatic nerve for four spots per area (Figure 2). The spot size was approximately 0.2 cm2. The output power of the laser irradiation was 30 mW per session with irradiation time for 60 sec per spot for 7 consecutive days. The energy density is 9 J/cm2. The output of the equipment was routinely checked by the Laser Check Power Meter (Coherent, Santa Clara, CA). A similar procedure was applied to 10 the control group with sham-operated LLLT, and the output power of laser irradiation was adjusted to 0. 2.5. Analysis of functional recovery For each rat, a series of functional assessments including SFI, VA and AA were performed to evaluate the animal’s motor functional recovery. A technical assistant who was blinded to treatment allocation evaluated sciatic nerve function with the interval of 1 week after surgery. 2.5.1. Sciatic function index The degree of recovery was monitored by evaluating the walking patterns of rats to obtain a SFI according to the method described by de Medinaceli et al. (de Medinaceli et al., 1982). Before the recording, a few conditioning trials were performed to accustom the animals to the track. All animals underwent preoperative walking-track analysis. Briefly, the feet of the rat’s hindlimbs were wetted with ink, and they were allowed to walk along a specially designed alley (84 cm length × 8.5 cm width) lined with scaled paper. Clear footprints were left by the released animals with red ink on the plantar surfaces of both hind paws. Recordings continued until five measurable footprints were collected. The data taken from the footprint for calculations were as 11 follows: (1) distance from the heel to the third toe, the print length (PL); (2) distance from the first to fifth toe, the toe spread (TS); and (3) distance from the second to the fourth toe, the intermediary toe spread (ITS). All three measurements were obtained from the experimental (E) and normal (N) sides. Prints were then calculated using the formula described by Bain et al. (Bain et al., 1989): SFI= −38.3 ([EPL−NPL]/NPL) + 109.5 ([ETS−NTS]/NTS) + 13.3 ([EIT−NIT]/NIT) −8.8. An SFI equal to -100 indicates total impairment, such as would result from a complete crush injury of the sciatic nerve, while an SFI oscillating around 0 is considered to reflect normal function. 2.5.2. Vertical activity of locomotion A Digiscan Animal Activity Monitor (Automated Digiscan, model RXYZCM 16, Columbus, OH) was employed to monitor the rats’ locomotion by using a procedure previously established in our laboratory (Hsieh et al., 2012, Wang et al., 2010). Animals were placed singly in a clear acrylic activity monitor cage (40 cm width × 40 cm depth × 30.5 cm height). Infrared monitoring sensors were located every 2.54 cm along the perimeter (16 infrared beams along each side) and 4.5 cm above the floor. Two additional sets of 16 sensors were located 10.5 cm above the floor on opposite sides. Data were collected and analyzed by a Digiscan Analyzer (Accuscan Model 12 CDA-8, Columbus, OH), which in turn sent information to a computer where it was stored for future analysis. One of the activity variables, VA, calculated directly by the Digiscan Analyzer, was selected for examination. The unanesthetized rats were not previously habituated to the cage in order to elicit more vertical exploratory locomotion after repeated exposures. 2.5.3. Measurement of ankle angle As described previously (Wang et al., 2010), animals’ AA were assessed by a kinematic gait analysis. Animals walked on a wooden track mounted on a table (20 cm width × 150 cm length × 15 cm height). Before data collection, several trials of walks were conducted to habituate the rats to the testing environment, and then 10 successful walks were collected for analysis. To ensure locomotion in a straight line, the width of the apparatus was adjusted to the size of the rats during the experiments, and a darkened cage was connected at the end of the corridor to attract the animals. Moreover, food was placed at the other end of the track as an incentive for further walking. The Expert Vision HiRes motion analysis system (Motion Analysis Corporation, Santa Rosa, CA) equipped with 5 CCD cameras were employed to capture the rat’s gait motion at 60 Hz sample rate. Data collection was made using the Sun Sparc workstation. The skin landmarker sets consisting of three reflexive markers were 13 tattooed at points at the proximal edge of the tibia, in the lateral malleolus and, in the fifth metatarsal head. AA was defined by the intersection of the lines extending from the knee to the ankle joint and from the ankle joint to the metatarsal head. The angles were expressed as degrees. The computer software “EVA 4.2” (Motion Analysis Corporation, Santa Rosa, CA) was employed to analyze the AA at terminal stance phase (the last moment at which the foot is in contact with the ground). In the sagittal plane analysis, the following formula was used in the mechanical analysis of the rat ankle: θankle = θfoot-θleg. The foot with θankle > 90° was considered plantarflexion; otherwise, the foot was considered dorsiflexion. 2.6. Electrophysiological studies The electrophysiological recordings were made with the dual-channel portable digital miniature EMG equipment (Neuro-EMG-Micro, ©Neurosoft, Ivanovo, Russia). The nerve was given a single electrical pulse of 50 μs duration up to supramaximal intensity stimulus through a pair of needle electrodes applied directly to the proximal side of the injured site. Amplitudes and latencies of compound muscle action potential (CMAP) were recorded with an active electrode needle 10 mm below the tibia tubercle and a reference needle 20 mm from the active electrode with 37-mm, disposable, monopolar Teflon-coated EMG needle electrodes. The onset latency (ms) was 14 measured from the stimulus to the takeoff of the first negative deflection. The peak amplitude (mV) of the CMAP curve from the baseline to the maximal negative peak was measured. The stimulation intensity and filtration ranges were 10-20 mA and 20-2000 Hz, respectively. For comparison, the ratio between the values of crush and intact sides (crush side/intact side) of peak amplitude and onset latency, expressed in percentage, were respectively calculated as % amplitude and % latency of CMAP to adjust for the effect of anesthesia. 2.7. Histopathological and immunohistochemical examinations Four weeks after the crush injury, the rats were sacrificed after being deeply anaesthetized with saturated KCl (300 g/ml, i.p.) while completing the final recording of the electrophysiological study. Then the sciatic nerve segment of the operated parts were harvested from the animals, which included the marked ‘‘crush site’’ in the middle of the nerve (1 cm in length). The normal sciatic nerve segments contralateral to the injured side in the same animals were also harvested for comparison. Nerve specimens were fixed in 10% neutral formalin, and embedded in paraffin for 12 h at room temperature. Then the specimens were subjected to diafanization using Xylene, dehydrated using graded ethanol, embedded in paraffin, and then cut longitudinally into 5-μm-thick sections using a microtome. Each nerve specimen produced 15 approximately 120 sections. The starting position for sampling was randomly selected by determining the first location of the specimen where the entire longitudinal section of the nerve could be recognized. A set of equidistantly spaced sections containing two consecutive sections was prepared for staining of hematoxylin and eosin (H&E) and S100 (DakoCytomation, Glostrup, Denmark) immunohistochemistry. Then each set at a distance of 50 μm was systematically harvested. A total of 10 sets containing 20 sections were then harvested from each specimen. Therefore, each staining assay was examined in 10 alternate sections, which were selected by a systematic-random series with a random start for analysis. For histopathological assessments, sections were stained with H&E (Muto Pure Chemicals Co., Ltd., Tokyo, Japan) to determine the infiltration of inflamed nerve cells and the vacuole formation proximal to the nerve stumps that presented the maximum diameter. For immunohistochemical staining, the slides of sciatic nerve sections were first incubated overnight at 4C with polyclonal rabbit anti-Schwann cells primary antibody (S100, 1:400, DakoCytomation, Glostrup, Denmark). After washing three times in PBS and then incubated with biotinylated goat anti-rabbit IgG secondary antibody (Jackson ImmunoResearch Laboratories, Inc., West Grove, PA) for 1 hour at room temperature. Following washing with phosphate buffer three times, sections were incubated with a streptavidin-horseradish peroxidase conjugate (Jackson ImmunoResearch Laboratories, 16 Inc., West Grove, PA). Finally, the sections were visualized as brown precipitates by adding 3, 3′-diaminobenzidine (DAB, Pierce, Rockford, IL) as a substrate. The sections were then counterstained with hematoxylin. Negative control sections received the same treatment without the addition of primary antibody. All H&E and immunohistochemical staining sections were examined using a light microscope (BX43, Olympus America Inc. Melville, NY). 2.8. Quantitative analysis of histopathological and immunohistochemical staining images The slides were examined and photographed at five randomly selected fields at 200× magnification using a light microscope (BX43, Olympus America Inc. Melville, NY) and a cooled digital color camera with a resolution of 1360 × 1024 pixels (DP70, Olympus America Inc. Melville, NY). The digital images were analyzed using a computer-based morphometry, ImageScope software package with the Color Deconvolution v9 tool (v9.1.19.1571, Aperio, Vista, CA). The area of the entire nerve specimen in each image was selected and outlined for analysis for all sections using a pen tool. The artifacts were excluded from the analyses using a negative pen of the ImageScope viewing software manipulated by two independent pathological experts who were unaware of the section origins. The measurement of each image was 17 repeated three times for statistical analysis. According to the automatically calculated parameters, the percentage of the positive and strong pixels to total stained pixels (%) was determined. The area of the inflamed cell, nerve nuclei and vacuole (%) in H&E-stained sections and the DAB-stained area of positive nuclear and cytoplasmic staining cells (%) for S100 immunohistochemistry were measured. 2.9. Statistical analysis All values of SFI, VA, AA, amplitudes and onset latencies of CMAP variables were expressed as mean ± standard deviation (SD). The results of these parameters for comparing the differences among groups and the serial changes within a group were analyzed using repeated measures ANOVA. One-way ANOVA was performed to compare individual group means for assessing parametric results of histopathology and immunohistochemical studies. Post hoc analysis was conducted with either Scheffé’s method or Dunnett’s test. The accepted level of statistical significance for the tests was set at p < 0.05 for all comparisons. All statistical analyses were performed using the Statistical Package for the Social Sciences Version 12.0 for Windows (SPSS Inc., Chicago, IL). 3. Results 18 3.1. Increase in functional recovery by LLLT combined with MSC therapy 3.1.1. Sciatic function index Comparison of serial time-dependent changes within each group. The serial alterations of SFI at pre-op, post-op, and four post-tr timepoints (0wpost-tr, 1wpost-tr, 2wpost-tr, 3wpost-tr) for each group were demonstrated in Figure 3A and Table 1. As can be seen, SFI was significantly different among observation timepoints and groups (F = 140.5, df = 15, p < 0.001). After sciatic nerve crush surgery, the SFI values were around -100 and decreased significantly when compared with the pre-op values of zero in each group, indicating that the nerve has been successfully crushed (all p < 0.001). After treatment, the 0wpost-tr, 1wpost-tr, 2wpost-tr and 3wpost-tr SFI values in the four groups showed significant recovery as compared with the post-op values, respectively (all p < 0.001). There were significant differences among the 0wpost-tr, 1wpost-tr, 2wpost-tr and 3wpost-tr SFI values, which showed a tendency of gradual increase in each group (all p < 0.01). However, the trend of increase in SFI among the four groups was different with the highest positive trend found in the MSCLLLT group (Figure 3A). The mean SFI values of the MSCLLLT group at final observation reached -24.60 ± 3.08, which were higher than those of the MSC (-50.38 ± 4.76), LLLT (-51.60 ± 3.85) and non-treated control (-69.93 ± 2.82) groups. Moreover, the 1wpost-tr SFI values were markedly increased when compared with those of 0wpost-tr in the MSC, 19 LLLT and MSCLLLT groups (all p < 0.001), but no significant improvement was observed in non-treated control animals (p > 0.05). Significant increase in SFI was found in each group at 2wpost-tr timepoint when compared with those of SFI at 1wpost-tr (all groups: 1wpost-tr vs. 2wpost-tr, p < 0.05). However, the 2wpost-tr and 3wpost-tr values in the MSC and LLLT and MSCLLLT groups revealed no significant differences. Comparison of serial changes among four groups. After treatment, the SFI values at each timepoint showed significant differences among groups (all p < 0.001). The SFI value immediately after treatment and observed at 0wpost-tr timepoint was significantly higher in both LLLT and MSCLLLT groups than in the non-treated control group (LLLT vs. control: p < 0.05; MSCLLLT vs. control: p < 0.001). No significant differences existed between MSC and non-treated control groups (p = 0.58), and between MSCLLLT and LLLT groups (p = 0.432). In addition, marked discrepancy also existed between MSCLLLT and MSC groups (p < 0.01). The SFI value one week after ceasing treatments and observed at 1wpost-tr timepoint was significantly higher in MSC, LLLT and MSCLLLT groups than in the non-treated control group (MSC vs. control: p < 0.001; LLLT vs. control: p < 0.001; MSCLLLT vs. control: p < 0.001). SFI also showed significant increase in the MSCLLLT group as compared with either MSC or LLLT group (MSCLLLT vs. MSC: p < 0.001; 20 MSCLLLT vs. LLLT: p < 0.001). No marked difference existed between MSC and LLLT groups (p = 0.112). The presentation of SFI at 2wpost-tr and 3wpost-tr timepoints also showed the same statistical results as those at 1wpost-tr timepoint. 3.1.2. Vertical activity of locomotion Comparison of serial time-dependent changes within each group. The serial alterations of the VA at pre-op, post-op, and four post-tr timepoints for each group were demonstrated in Figure 3B and Table 1. VA was significantly different among groups and observation timepoints (F = 12.68, df = 15, p < 0.001). After sciatic nerve crush surgery, the VA values were significantly decreased when compared with the pre-op values in each group, indicating that motor function was impaired by nerve crushed (all p < 0.001). After treatment, the 0wpost-tr, 1wpost-tr, 2wpost-tr and 3wpost-tr VA values in the four groups showed significant recovery as compared with the post-op values, respectively (all p < 0.001). However, marked differences among the 0wpost-tr, 1wpost-tr, 2wpost-tr and 3wpost-tr VA values, which showed a tendency of gradual increase, were only found in LLLT and MSCLLLT groups (LLLT: p < 0.01; MSCLLLT: p < 0.001) not in MSC and non-treated control groups. There was no significant difference in the results of these two groups throughout the four weekly observation (MSC: p = 0.12; control: p = 0.40). The 1wpost-tr, 2wpost-tr and 21 3wpost-tr VA values were significantly increased when compared with those of 0wpost-tr in the MSCLLLT group (all p < 0.001). However, significant increase in VA was found in the LLLT group at 2wpost-tr and 3wpost-tr timepoints when compared with VA at 0wpost-tr (2wpost-tr vs. 0wpost-tr, p < 0.05; 3wpost-tr vs. 0wpost-tr, p < 0.01). Moreover, the 3wpost-tr VA value of MSCLLLT group was no significant difference when compared with VA at pre-op (p > 0.05). The MSCLLLT group showed the highest positive trend among the four groups (Figure 3B). The mean VA values of the MSCLLLT group at the final observation reached 1007.92 ± 18.05, which approached the pre-op level and was higher than that of MSC (749.83 ± 23.00), LLLT (755.83 ± 16.43) and non-treated control (558.25 ± 17.69) groups. Comparison of serial changes among four groups. After treatment, there were significant differences in VA values among the four groups observed at 0wpost-tr, 1wpost-tr, 2wpost-tr and 3wpost-tr timepoints (ANOVA, all p < 0.001). The VA values immediately after treatment and observed at 0wpost-tr timepoint were significantly higher in the MSCLLLT group than in LLLT (p < 0.05), MSC (p < 0.05) and non-treated control groups (p < 0.01). The VA values of both MSC and LLLT groups revealed no significant difference from those of the non-treated control group (MSC vs. control: p = 0.89; LLLT vs. control: p = 0.69). The presentation of VA at 1wpost-tr and 2wpost-tr timepoints also showed the same statistical results as those at 0wpost-tr 22 timepoint. Nevertheless, three week after ceasing treatments, VA values at the final observation were significantly higher in MSC, LLLT and MSCLLLT groups than in the non-treated control group (MSC vs. control: p < 0.001; LLLT vs. control: p < 0.001; MSCLLLT vs. control: p < 0.001). Moreover, VA values of the MSCLLLT group were significantly higher than those of either the MSC or LLLT group (MSCLLLT vs. MSC: p < 0.001; MSCLLLT vs. LLLT: p < 0.001). No marked difference existed between MSC and LLLT groups (p = 0.99). 3.1.3. Angle of ankle Comparison of serial time-dependent changes within each group. The serial alterations of the AA at pre-op, post-op, and four post-tr timepoints for each group were demonstrated in Figure 3C and Table 1. As can be seen, there was marked difference in AA among observation timepoints and groups (F = 50.38, df = 15, p < 0.001). AA was significantly decreased at post-op condition in animals with nerve crush compared with that at the pre-op condition (all p < 0.001), indicating that the ankle plantar flexion in toe-off stance phase of gait was impaired by the nerve crushed. AA gradually recovered at four post-tr timepoints in each group (all p < 0.001), but the trend of increase in each group differed (Figure 3C). The highest positive trend was found in the MSCLLLT group when compared with the other groups. The mean AA 23 values at the final observation of the MSCLLLT group reached 103.57 ± 17.23, which were higher than those of MSC (64.75 ± 4.29), LLLT (70.85 ± 3.63) and non-treated control (54.62 ± 6.00) groups. After LLLT treatment, the AA values were significantly increased at 0wpost-tr timepoint when compared with those at post-op in LLLT and MSCLLLT groups (all p < 0.001), but there was no significant improvement in MSC and non-treated control animals that did not receive LLLT treatment (0wpost-tr vs. post-op in MSC group: p > 0.05; 0wpost-tr vs. post-op in control: p > 0.05). The significant increase in AA values did not occur until timepoints of 2wpost-tr in the MSC group and 3wpost-tr in the non-treated control group when compared with their post-op values (2wpost-tr vs. post-op in MSC group: p < 0.001; 3wpost-tr vs. post-op in control: p < 0.001). Comparison of serial changes among four groups. AA values were significantly different among groups at 0wpost-tr, 1wpost-tr, 2wpost-tr and 3wpost-tr timepoints (ANOVA, all p < 0.001), not at pre-op and post-op timepoints (All p > 0.05). AA values immediately after treatment and observed at 0wpost-tr timepoint were significantly higher in the MSCLLLT group than in LLLT, MSCLLLT, and non-treated control groups (MSCLLLT vs. LLLT: p < 0.01; MSCLLLT vs. MSC: p < 0.01; MSCLLLT vs. control: p < 0.001). No significant difference existed among MSC, LLLT and non-treated control groups (p > 0.05). One week after ceasing treatments, 24 AA observed at 1wpost-tr timepoint was significantly higher in MSC, LLLT and MSCLLLT groups than in the non-treated control group (MSC vs. control: p < 0.001; LLLT vs. control: p < 0.001; MSCLLLT vs. control: p < 0.001). AA was significantly higher in the MSCLLLT group when compared with either MSC or LLLT group (MSCLLLT vs. MSC: p < 0.001; MSCLLLT vs. LLLT: p < 0.001). No significant difference existed between MSC and LLLT groups (p = 0.13). The presentation of AA at 2wpost-tr and 3wpost-tr timepoints also showed the same statistical results as those at 1wpost-tr timepoint. 3.2. Improvement of compound muscle action potential by LLLT combined with MSC therapy The alterations of CMAP amplitude and latency percentages at post-op, 0wpost-tr and 3wpost-tr timepoints were shown in Figure 4. Immediately after LLLT treatment, CMAP percentage amplitude increased significantly in the MSCLLLT group when compared with that in the non-treated control (p < 0.01). At the final observation at 3wpost-tr timepoint, CMAP amplitude percentage increased significantly in MSC, LLLT and MSCLLLT groups as compared with the non-treated control group (all p < 0.001). There was also significant increase found in the MSCLLLT group when compared with MSC and LLLT groups (All p < 0.001). However, there was no 25 significant difference between MSC and LLLT groups (p = 0.96). CMAP latency percentage showed a general trend of decrease at 0wpost-tr timepoint where the decrease was more marked in the MSCLLLT group when compared with MSC, LLLT, and non-treated control groups (p < 0.05). No significant difference was seen when comparing MSC with control, LLLT with control, and MSC with LLLT group (p > 0.05). At the final observation at 3wpost-tr timepoint, significant differences were also seen when comparing the control with MSCLLLT, MSC and LLLT groups, respectively (p < 0.05). There was no significant difference among MSC, LLLT and MSCLLLT groups (p > 0.05). The above findings reveal that treatment with either MSC or LLLT alone promoted nerve regeneration better than the non-treated control. MSC combined with LLLT treatment showed the most beneficial effects. 3.3. Improvement of morphological changes by LLLT combined with MSC therapy The parameters of morphological changes such as inflamed cells, vacuole and myelination as evidenced by the expression of S-100 were presented in Figure 5. In the H&E study, the nuclei percentage was diffusely increased, showing more inflammation and cell infiltration after nerve crush when compared with non-injured nerve (Figure 5A). A pronounced infiltration of the immune cells was detected around the 26 MSC-transplanted area in the MSC group (Figure 5C) when compared with LLLT (Figure 5D) and non-treated control (Figure 5B) groups, which did not receive MSC transplantation (p < 0.05, Figure 5F). Moreover, infiltration of the immune cells was significantly decreased in the MSCLLLT group compared with the MSC group (p < 0.05, Figure 5F). The vacuole formation was also increased after nerve crush when compared with the non-injured nerve (Figure 5G). Crush-induced vacuole formation (Figure 5H) and this event was reduced by the administration of MSC alone (p < 0.01, Figure 5I), LLLT alone (p < 0.01, Figure 5J) and combination of MSC and LLLT (p < 0.001, Figure 5K). The combined treatment enhanced the results when compared with either MSC or LLLT alone (MSCLLLT vs. MSC: p < 0.01; MSCLLLT vs. LLLT: p < 0.01, Figure 5L). Less expression of S-100 was observed after crush injury in the non-treated control group (Figure 5N), but a significant amount of S-100 expression was observed in MSC (p < 0.001), LLLT (p < 0.001) and MSCLLLT (p < 0.001) groups. However, the combined treatment reinforced the effect when compared with either MSC or LLLT alone (MSCLLLT vs. MSC: p < 0.001; MSCLLLT vs. LLLT: p < 0.001). 4. Discussion In the current study, we demonstrated that 660-nm-GaAlAs LLLT at a dose of 9 27 J/cm2 promotes significant functional recovery in crush nerve rats. Similar to previous findings, the results demonstrated that crushed nerves irradiated with laser can exhibit myelinated fibers of greater diameter and a better recovery of functions (Santos et al., 2012). Moreover, we also demonstrated that MSC transplantation can augment more functional recovery than non-treatment, which is consistent with other studies (Gigo-Benato et al., 2010, Pan et al., 2006). The deterioration of neurological function was attenuated by single treatment of either MSC or LLLT alone. However, these effects on incremental improvement in crush nerve studies are considered to be limited (Pan et al., 2006, Santos et al., 2012). Many studies have reported greater functional recovery by stem cell transplantation when other forms of therapeutic interventions are also applied (Pan et al., 2009a, Pan et al., 2009c). However, from our results, it is evident that the combined treatment of LLLT and MSC transplantation would achieve more beneficial restoration than either of the single treatments, leading to sufficient electrophysiological, morphological and functional recovery in rats with crush nerve injury. The SFI scores changed throughout the course of the experiment, indicating a true neurotmesis for the rats, because partial recovery was seen without signs of total recovery when the SFI remained close to -100. Sciatic nerve and nerve sheath were disrupted by crush injury, almost producing total paralysis in rats. Dramatic 28 improvement in SFI scores was seen immediately after LLLT treatment in both groups that received LLLT regardless whether MSC was transplanted. LLLT is evident as an instant form of treatment to promote function recovery of the damaged nerves; however, MSC transplantation does not appear to be a rapid effective treatment. When comparing the single-treatment groups with the combined-treatment group, the group treated with combination of MSC and LLLT shows better improved SFI with significant difference from the groups treated with MSC or LLLT alone. VA count is associated with the rearing behavior for exploration of rats and the gain in VA value could indicate that the hind limbs have managed to regain sufficient strength to bear the body weight due to nerve reinnervation of the gastrocnemius muscle. Immediately after treatment, only the MSCLLLT group that received combination of MSC and LLLT treatments showed improvement and recovered to ~70%, which was much more than the MSC (~55%), LLLT (~54%) and nontreated (~44%) groups. At follow-up observation, the MSC and LLLT groups had steady increases in VA recovery over time, which were better than the non-treated group, but still lower than the MSCLLLT group. The AA values were similar to the VA values, with the MSCLLLT group achieving better recovery than MSC, LLLT and non-treated control groups. Better recovery of the MSCLLLT group compared with that of the MSC or LLLT group could indicate that combination of MSC and LLLT enhances 29 more nerve reinnervation of the gastrocnemius muscle than single treatment. This fact was further supported by the electrophysiological studies on CMAP. It appears that greater amounts of depolarized muscle fibers were successfully recruited with combination of MSC and LLLT by showing significant improvement in amplitudes and latencies of CMAP. The host adverse immune response plays an important role in the survival of transplanted cells and nerve regeneration (Luo et al., 2012). However, intense inflammation conversely induces apoptosis and impairs nerve restoration (Hotchkiss and Nicholson 2006). Many studies have shown that transplantation of stem cells triggered inflammation and macrophage infiltration (Luo et al., 2012, McGrath et al., 2012) and posed a deleterious effect on stem cells. Stem cell-triggered inflammation also failed to enhance axonal regeneration (McGrath et al., 2012). The transplantation of MSCs might require immunosuppressant on immune responses to achieve and improve axonal regeneration (McGrath et al., 2012). In our morphological study, four weeks after surgery, H&E staining showed that the degree of inflammatory cell invasion in the MSC group was greater than that in the other groups. In contrast, combination of MSC and LLLT resulted in a significant decrease of inflammatory cells. Thus, we propose that the MSC transplant-induced inflammatory cell accumulation may be suppressed by LLLT intervention to enhance functional recovery. 30 Several studies have already shown that LLLT promotes functional recovery and accelerates the peripheral nerve regeneration process (Anders et al., 2004, Gigo-Benato et al., 2010, Hsieh et al., 2012, Rochkind 2009, Rochkind et al., 2009). There are growing evidences that several aspects of the inflammatory process can be modulated by LLLT in experimental models of inflammation (Albertini et al., 2007, Hashmi et al., 2010, Moriyama et al., 2005, Rizzi et al., 2006). Our previous study also demonstrated that the use of LLLT could decrease inflammation to accelerate functional recovery by modulating and interacting with some biochemicals, such as proinflammatory cytokines and S100 proteins (Hsieh et al., 2012). Laser delivered transcutaneously induced a statistically significant suppression of immune cell invasion and pro-inflammatory cytokine and chemokine gene expression to improves recovery after acute spinal cord injury (Byrnes et al., 2005). Therefore, the reduction of inflammatory cell accumulation by LLLT would be an essential step for nerve regeneration. LLLT may be used as a novel applicable therapeutic approach for the improvement of tissue inflammation in nerve entrapment neuropathy, as well as for the promotion of nerve regeneration (Hsieh et al., 2012). In this study, the MSC therapy combined with addition of LLLT could further decrease the inflammatory cell infiltration to suppress the transplant-induced inflammatory responses and to promote nerve functional recovery by enhancing S100 expression. 31 In addition, the effects of LLLT on the proliferation of MSCs have also been validated in many studies. Multiple exposures to LLLT at 630-nm wavelength enhances proliferation and osteogenic differentiation of bone marrow MSCs (Li et al., 2010). Using LLLT also enhances bone marrow MSC differentiation into neurons (Soleimani et al., 2012). LLLT is an effective biostimulator of transplanted adipose-derived MSCs in wound healing that enhances the survival of MSCs and stimulates the secretion of growth factors in the wound bed (Kim et al., 2012). LLLT also increases growth factors secretion from MSCs (Hou et al., 2008). Therefore, we propose LLLT not only reduces MSC transplant-induced inflammation, but also may enhance the growth of MSCs. Taken together, LLLT is potentially amenable to be an adjuvant therapeutic manipulation for clinical application of MSCs. The limitation of this study was the fate of MSC in all transplanted rats not tracked during the 4-week observation. The deficiency in confirming whether LLLT inflicted severe damage on the transplanted MSCs in crush nerve may be criticized. However, some conclusions based on many studies may support our findings that LLLT reasonably applied on transplanted cells, because they demonstrated that LLLT can promote proliferation and growth of MSCs (Hou et al., 2008; Li et al., 2010; Kim et al., 2012; Soleimani et al., 2012). In addition, our preliminary study (unpublished data) also found the bromodeoxyuridine (BrdU)-labeled MSC was still abundant in injured 32 site immediately and 1 week after ceasing LLLT. Further studies in this direction are needed to assess the interaction occurring between LLLT and transplanted MSCs. 5. Conclusion MSC transplantation combined with LLLT did achieve better functional recovery than a conventional treatment of MSC or LLLT alone. It appears that LLLT has a synergistic effect on functional recovery with MSC transplantation as was assumed by our hypothesis. Combination therapeutics strategies may be the way to tap into the potential benefits that the MSC has to offer towards functional recovery in the future. Acknowledgments The authors would like to thank Ms. Tu PW for her skills and technical assistance with the assessments of functional recovery and Dr. Wu PC for his valuable advice regarding neurosurgery. References Albertini R, Villaverde AB, Aimbire F, et al. 2007; Anti-inflammatory effects of low-level laser therapy (LLLT) with two different red wavelengths (660 nm and 684 nm) in carrageenan-induced rat paw edema. J Photochem Photobiol B 89: 50-55. 33 Anders JJ, Geuna S, Rochkind S. 2004; Phototherapy promotes regeneration and functional recovery of injured peripheral nerve. Neurol Res 26: 233-239. Bain JR, Mackinnon SE, Hunter DA. 1989; Functional evaluation of complete sciatic, peroneal, and posterior tibial nerve lesions in the rat. Plast Reconstr Surg 83: 129-138. Byrnes KR, Waynant RW, Ilev IK, et al. 2005; Light promotes regeneration and functional recovery and alters the immune response after spinal cord injury. Lasers Surg Med 36:171-185. Cho YB, Cho HH, Jang S, et al. 2011; Transplantation of neural differentiated human mesenchymal stem cells into the cochlea of an auditory-neuropathy guinea pig model. J Korean Med Sci 26: 492-498. Dezawa M, Takahashi I, Esaki M, et al. 2001; Sciatic nerve regeneration in rats induced by transplantation of in vitro differentiated bone-marrow stromal cells. Eur J Neurosci 14:1771-1776. de Medinaceli L, Freed WJ, Wyatt RJ. 1982; An index of the functional condition of rat sciatic nerve based on measurements made from walking tracks. Exp Neurol 77: 634-643. Gigo-Benato D, Geuna S, Rochkind S. 2005; Phototherapy for enhancing peripheral nerve repair: a review of the literature. Muscle Nerve 31: 694-701. 34 Gigo-Benato D, Russo TL, Tanaka EH, et al. 2010; Effects of 660 and 780 nm low-level laser therapy on neuromuscular recovery after crush injury in rat sciatic nerve. Lasers Surg Med 42: 673-682. Gigo-Benato D, Geuna S, de Castro Rodrigues A, et al. 2004; Low-power laser biostimulation enhances nerve repair after end-to-side neurorrhaphy: a double-blind randomized study in the rat median nerve model. Lasers Med Sci 19: 57-65. Hashmi JT, Huang YY, Sharma SK, et al. 2010; Effect of pulsing in low-level light therapy. Lasers Surg Med 42: 450-466. Hotchkiss RS, Nicholson DW. 2006; Apoptosis and caspases regulate death and inflammation in sepsis. Nat Rev Immunol 6: 813-822. Hsieh YL, Chou LW, Chang PL, et al. 2012; Low-level laser therapy alleviates neuropathic pain and promotes function recovery in rats with chronic constriction injury: Possible involvements in hypoxia-inducible factor 1alpha (HIF-1alpha). J Comp Neurol 520: 2903-2916. Hou JF, Zhang H, Yuan X, et al. 2008; In vitro effects of low-level laser irradiation for bone marrow mesenchymal stem cells: proliferation, growth factors secretion and myogenic differentiation. Lasers Surg Med 40:726-733. Kim H, Choi K, Kweon OK, et al. 2012; Enhanced wound healing effect of canine adipose-derived mesenchymal stem cells with low-level laser therapy in athymic 35 mice. J Dermatol Sci pii: S0923-1811(12)00291-5. Li WT, Leu YC, Wu JL. 2010; Red-light light-emitting diode irradiation increases the proliferation and osteogenic differentiation of rat bone marrow mesenchymal stem cells. Photomed Laser Surg Suppl 1:S157-165 Luo H, Zhang Y, Zhang Z, et al. 2012; The protection of MSCs from apoptosis in nerve regeneration by TGFbeta1 through reducing inflammation and promoting VEGF-dependent angiogenesis. Biomaterials 33: 4277-4287. McGrath AM, Brohlin M, Kingham PJ, et al. 2012; Fibrin conduit supplemented with human mesenchymal stem cells and immunosuppressive treatment enhances regeneration after peripheral nerve injury. Neurosci Lett 516:171-176. Moriyama Y, Moriyama EH, Blackmore K, et al. 2005; In vivo study of the inflammatory modulating effects of low-level laser therapy on iNOS expression using bioluminescence imaging. Photochem Photobiol 81: 1351-1355. Murakami T, Fujimoto Y, Yasunaga Y, et al. 2003; Transplanted neuronal progenitor cells in a peripheral nerve gap promote nerve repair. Brain Res 974: 17-24. Navarro X, Vivo M, Valero-Cabre A. 2007; Neural plasticity after peripheral nerve injury and regeneration. Prog Neurobiol 82: 163-201. Noble J, Munro CA, Prasad VS, et al. 1998; Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries. J Trauma 36 45: 116-122. Pan HC, Yang DY, Chiu YT, et al. 2006; Enhanced regeneration in injured sciatic nerve by human amniotic mesenchymal stem cell. J Clin Neurosci 13: 570-575. Pan HC, Cheng FC, Chen CJ, et al. 2007; Post-injury regeneration in rat sciatic nerve facilitated by neurotrophic factors secreted by amniotic fluid mesenchymal stem cells. J Clin Neurosci 14: 1089-1098. Pan HC, Chin CS, Yang DY, et al. 2009a; Human amniotic fluid mesenchymal stem cells in combination with hyperbaric oxygen augment peripheral nerve regeneration. Neurochem Res 34: 1304-1316. Pan HC, Chen CJ, Cheng FC, et al. 2009b; Combination of G-CSF administration and human amniotic fluid mesenchymal stem cell transplantation promotes peripheral nerve regeneration. Neurochem Res 34: 518-527. Pan HC, Yang DY, Ho SP, et al. 2009c; Escalated regeneration in sciatic nerve crush injury by the combined therapy of human amniotic fluid mesenchymal stem cells and fermented soybean extracts, Natto. J Biomed Sci 16: 75. Rizzi CF, Mauriz JL, Freitas Correa DS, et al. 2006; Effects of low-level laser therapy (LLLT) on the nuclear factor (NF)-kappaB signaling pathway in traumatized muscle. Lasers Surg Med 38: 704-713. Rochkind S. 2009; Phototherapy in peripheral nerve regeneration: From basic science 37 to clinical study. Neurosurg Focus 26: E8. Rochkind S, Vogler I, Barr-Nea L. 1990; Spinal cord response to laser treatment of injured peripheral nerve. Spine (Phila Pa 1976) 15: 6-10. Rochkind S, Geuna S, Shainberg A. 2009; Chapter 25: Phototherapy in peripheral nerve injury: effects on muscle preservation and nerve regeneration. Int Rev Neurobiol 87: 445-464. Santos AP, Suaid CA, Xavier M, et al. 2012; Functional and morphometric differences between the early and delayed use of phototherapy in crushed median nerves of rats. Lasers Med Sci 27: 479-486. Shamir MH, Rochkind S, Sandbank J, et al. 2001; Double-blind randomized study evaluating regeneration of the rat transected sciatic nerve after suturing and postoperative low-power laser treatment. J Reconstr Microsurg 17: 133-137. Soleimani M, Abbasnia E, Fathi M, et al. 2012; The effects of low-level laser irradiation on differentiation and proliferation of human bone marrow mesenchymal stem cells into neurons and osteoblasts – an in vitro study. Lasers Med Sci 27: 423-430. Van Breugel HH, Bar PR. 1993; He-Ne laser irradiation affects proliferation of cultured rat Schwann cells in a dose-dependent manner. J Neurocytol 22: 185-190. Wang J, Yang CC, Chen SC, et al. 2010; No synergistic effect of mesenchymal stem 38 cells and exercise on functional recovery following sciatic nerve transection. Funct Neurol 25: 33-43. Wollman Y, Rochkind S, Simantov R. 1996; Low power laser irradiation enhances migration and neurite sprouting of cultured rat embryonal brain cells. Neurol Res 18: 467-470. 39 Figure legends Figure 1. Sequences of crush nerve surgery, MSC/non-MSC transplantation, LLLT/sham treatment and assessments throughout the experiment. Abbreviations: 0wpost-tr, 1wpost-tr, 2wpost-tr, and 3wpost-tr, immediately and 1-3 weeks after ceasing treatment; AA, ankle angle; CMAP, compound muscle action potential; LLLT, low-level laser therapy; MSC, mesenchymal stem cell; post-op, after surgery; pre-op, before surgery; SFI, sciatic function index; VA, vertical activity of locomotion. Figure 2. Illustration of laser application points (black circles) through transcutaneous method. Figure 3. Effects of MSC and LLLT treatments on sciatic function index (A), vertical activity of locomotion (B) and ankle angle (C) before (pre-op), after surgery (post-op), and immediately and 1-3 weeks after ceasing LLLT treatment (0wpost-tr, 1wpost-tr, 2wpost-tr, 3wpost-tr). * indicates p < 0.05 among four groups at the same timepoint tested by repeated measures ANOVA. Figure 4. Effects of MSC and LLLT treatments on electrophysiological studies including ratios of intact/injured CMAP amplitudes (A) and onset latencies (B) recorded 10 hours after surgery (post-op), immediately and 3 weeks after ceasing LLLT treatment (0wpost-tr and 3wpost-tr). * indicates p < 0.05 tested by the Scheffé’s post hoc test. 40 Figure 5. Assessments of inflammation (A-E), vacuole formation (G-K) and S100 expressions (M-Q) in longitudinal sections of sciatic nerves by using H&E staining and S100 immunohistochemistry. Representative sections of sciatic nerves (bar = 50μm) obtained from animals with non-injured, non-treated, MSC, LLLT and combined LLLT and MSC (MSCLLLT) treatments. The quantitative analysis of H&E and immunostaining for inflamed cells, vacuole formation and S100 expressions are shown as F, L, and R, respectively. Values in each bar with different superscripts (a, b, c) indicate significant difference between each other at confidence level of p < 0.05 tested by the Scheffé’s post hoc test. The scale is 50 μm. Arrows indicate the crush and MSC-injected sites with a sutured mark. 41