Chromosome Rearrangement (eg translocation) Testing
advertisement
 Testing")
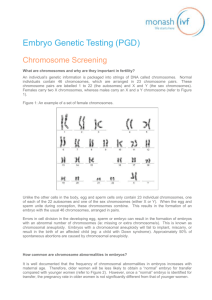
Embryo Genetic Testing (PGD) Chromosome Rearrangement (eg translocation) Testing What are chromosome rearrangements and how do they impact fertility? An individual’s genetic information is packaged into strings of DNA called chromosomes. Normal individuals contain 46 chromosomes, which are arranged in 23 chromosome pairs. These chromosome pairs are labelled 1 to 22 (the autosomes) and X and Y (the sex chromosomes). Females have two X chromosomes, whereas males have one X and one Y chromosome (refer to Figure 1). Figure 1: An example of a set of female chromosomes. Rather than carrying 46 regular chromosomes, some individuals carry a chromosome rearrangement. These chromosome rearrangements can be classified according to how the chromosome material has been rearranged (Figure 2): A reciprocal translocation occurs when two chromosomes break and then rejoin with the wrong segment. This results in the formation of two translocated chromosomes. A Robertsonian translocation occurs when two chromosomes break, and the long arms of each of the chromosomes join together. This results in the formation of a large “translocated chromosome” in the place of two regular chromosomes. A pericentric inversion occurs when one chromosome breaks twice, once on each arm of the chromosome. The chromosomal material located between these breakpoints rotates 180o and reinserts, with the breakpoints reuniting. A paracentric inversion occurs when one chromosome breaks twice, and both breakpoints are on the same arm of the chromosome. The chromosomal material located between these breakpoints rotates 180o and reinserts, with the breakpoints reuniting. Figure 2: Different types of chromosome rearrangements. Regular Chromosomes Reciprocal Translocation Robertsonian Translocation Pericentric Inversion* Paracentric Inversion* * Inverted regions are indicated by cross shading Carriers of these chromosome rearrangements are considered “balanced” because all their genetic information is present. They often experience no symptoms and are not aware that they carry the chromosome rearrangement. However, they may experience difficulties with reproduction due to the generation of chromosomally unbalanced embryos. This may result in difficulty to conceive, recurrent miscarriage or the birth of a child with a chromosome abnormality. ormal What is chromosome rearrangement PGD testing? Chromosomes PGD may be available to couples where one partner carries a balanced chromosomal rearrangement, such as a translocation. PGD with chromosome rearrangement testing can be used to screen IVF embryos to distinguish between normal/balanced embryos (which have the potential to produce a healthy baby) and unbalanced embryos (which would fail to implant, miscarry or result in an affected baby). PGD testing cannot distinguish between normal embryos and embryos that are balanced for the chromosome rearrangement. In addition to testing for the chromosome rearrangement, in some cases it may be possible to analyse all of the remaining chromosomes in the embryo (ie. chromosome screening). Some embryos can have an abnormal number of chromosomes (ie: missing or extra chromosome/s) due to errors in cell division in the developing egg, sperm or embryo. This is known as chromosomal aneuploidy. An aneuploid embryo will fail to implant, miscarry, or result in the birth of an affected child (eg: a child with Down syndrome). Only normal/balanced embryos will be selected for transfer to the uterus. This testing will help to ensure that the embryo that is selected for transfer has the best possible chance of developing into a healthy baby. How is chromosome rearrangement PGD testing done? Step 1: Chromosome testing on each partner In order to undertake PGD, one or both partners must have been found to carry a chromosome rearrangement (ie: translocation or inversion). The PGD team needs to know the precise chromosome rearrangement in order to develop a PGD test. Step 2: Genetic counselling in PGD clinic and PGD test selection Once the specific chromosome rearrangement has been identified, the couple attend an appointment with a clinical geneticist and/or genetic counsellor. During this appointment the couple will be provided with information relating to PGD and will have an opportunity to have any questions answered. This appointment is free of charge and enables couples to decide if PGD is the right option for them. Monash IVF currently offers chromosome rearrangement testing using three different test types, called SNP array testing, Array-CGH and Fluorescent in-situ hybridisation (FISH). Each of these tests is capable of detecting some, but not all, chromosome rearrangements. Therefore, the test type/s available will depend on the specific chromosome rearrangement that has been identified in each couple. Genetic counselling is an important step to help patients understand the differences between the tests, so that they make an informed decision regarding which test is best in their case. The PGD testing option that is performed will be decided by the patient in consultation with their IVF specialist and Genetic Counsellor. A comparison of the different PGD test types is provided in Table 1. Table 1: Comparison of the different PGD test types for chromosome rearrangement testing. SNP array ArrayCGH Screen 24 chromosomes x Detect haploidy Some x Some x (the presence of two copies of a given chromosome from one parent and none from the other. This can result in particular genetic syndromes or medical, cognitive or physical disabilities). x x Determine the parental origin of chromosome abnormalities x x Confirm genetic parentage x x Detect extraneous DNA contamination x x Cost for feasibility testing x x 1 month 1 month 3 - 6 months ICSI ICSI Standard insemination or ICSI per cycle per embryo per cycle D3 or D5/6 D3 or D5/6 D3 only Frozen Frozen Fresh or Frozen Criterion Detect unbalanced chromosome rearrangement (Reciprocal and Robertsonian translocations, Pericentric inversions) (a missing set of all chromosomes, which results in implantation failure) FISH (if targeted) Detect triploidy (an extra set of all chromosomes, which results in implantation failure or miscarriage) Detect uniparental disomy Estimated time frame for feasibility Fertilisation method (Standard insemination or Intracytoplasmic sperm injection) Embryo biopsy fee charged Day of embryo biopsy Embryo transfer Step 3: Feasibility testing Prior to commencement of an IVF/PGD cycle, it is necessary for the couple to undergo a feasibility test in order to determine if PGD will be possible for their particular chromosome rearrangement. The purpose of feasibility testing is to determine which test type/s is appropriate for the chromosome rearrangement in question. The feasibility test will also ensure that the final PGD test can adequately distinguish between normal/balanced embryos (suitable for transfer) and all possible unbalanced embryos (not suitable for transfer). The feasibility process is slightly different for each test type: 1. SNP array testing (performed using “parental support”) Feasibility testing will require a copy of the carrier’s genetic report. Based on this genetic report, the Genetics team will determine whether or not SNP array testing is capable of distinguishing between embryos which are normal/balanced for the chromosome rearrangement and embryos which are unbalanced for the chromosome rearrangement. Assuming PGD is feasible, a repeat chromosome test will be performed to ensure that the final PGD test is targeting the correct chromosome rearrangement. There is no charge for this feasibility testing process. 2. Array-CGH (performed using 24Sure technology) Feasibility testing is performed using the same process as outlined for the SNP array testing. 3. Fluorescent in situ hybridisation (FISH) Feasibility testing will require a blood sample from both partners. Cells will be extracted from this blood sample and used for test development. The PGD scientists will identify a set of fluorescent DNA probes which are capable of distinguishing between embryos which are normal/balanced for the chromosome rearrangement and embryos which are unbalanced for the chromosome rearrangement. Once an accurate test has been developed, it will be validated on cells from embryos which have been donated for succumbed research and training. This will help the Monash IVF PGD laboratory to ensure that the final test is sensitive enough to provide a result from a single cell from an IVF embryo. There is a non-refundable fee for this feasibility test. A feasibility report outlining the results of the feasibility testing will be sent to the couple’s IVF doctor and genetic counsellor. The IVF doctor or genetic counsellor will contact the couple to go through the results of the feasibility testing process. In some instances it may not be possible to develop an accurate test and PGD may not be available. Step 4: IVF and embryo biopsy Once feasibility testing has been completed and PGD is feasible, the couple are able to undertake an IVF/PGD cycle. All couples undergoing PGD testing must undertake an IVF cycle to stimulate the woman’s ovaries to produce a number of eggs. These eggs are collected and fertilised using the male partner’s sperm. If the couple are planning to undertake SNP array testing or array-CGH, the embryos must be created using a fertilisation method called Intracytoplasmic Sperm Injection (ICSI). ICSI involves the injection of a single sperm into the egg and is specifically used for these test types to reduce the risk of misdiagnosis due to the presence of additional sperm around the egg/embryo. If the couple are planning to undertake FISH testing, they can elect to have ICSI or standard fertilisation. This decision will be made in consultation with their IVF clinician. After fertilisation, embryos are cultured in the laboratory and their growth is monitored on a daily basis. Embryo biopsy (sampling cell/s from the embryo for genetic testing) can potentially be performed at two different stages during an embryo’s development. The stage of embryo biopsy will be influenced by the PGD test type chosen (Refer to Table 1): 1. Day 3 embryo biopsy is performed 3 days after fertilization, when the embryo is at the cleavage stage and is typically composed of 6 to 8 cells. Embryos that have developed to at least 5 cells on Day 3 are suitable for biopsy. A hole is drilled in the outer shell of the embryo and 1 or 2 cells are removed for genetic analysis (refer to Figure 3). This type of embryo biopsy can be performed for SNP array testing, array-CGH or FISH. Figure 3: Day 3 embryo biopsy 2. Day 5/6 embryo biopsy is performed 5 or 6 days after fertilization. By this time, the embryo should have developed to the blastocyst stage, and should be comprised of an inner cell mass (which will go on to form the fetus) and trophectoderm cells (which will go on to form the placenta). Embryos need to have a clear inner cell mass and a suitable number of healthy trophectoderm cells to be considered suitable for biopsy. Approximately 5 trophectoderm cells are removed for genetic analysis (Refer to Figure 4). This type of embryo biopsy is only available for SNP array testing or array-CGH (ie: Day 5/6 biopsy is not available for FISH testing). Figure 4: Day 5/6 embryo biopsy Where possible, Monash IVF recommends Day 5/6 biopsy. This is due to the following reasons: Randomised control trials have shown that Day 5/6 biopsy is better for the embryo compared with Day 3 biopsy (Scott et al, 2013). The embryo has more cells on Day 5/6 of development (~100 to 150 cells) compared with Day 3 of development (~6 to 8 cells). This means: - More cells can be biopsied for genetic testing on Day 5/6 of development compared with Day 3 of development (ie: approximately 5 cells versus 1-2 cells, respectively). The availability of more cells improves the accuracy of the PGD test results. - Despite biopsying more cells from Day 5/6 embryos, a smaller percentage of cells is removed from the embryo following a Day 5/6 biopsy compared with a Day 3 biopsy (ie: we are removing approximately 5/100 (5%) cells on Day 5/6, compared with 1/6 (17%) cells on Day 3). Day 5/6 embryos are more likely to be chromosomally normal then Day 3 embryos (as some of the embryos that are abnormal on Day 3 do not have the developmental capacity to grow to Day 5/6 in culture). Therefore, growing the embryos to Day 5/6 before performing the PGD testing provides an element of natural selection. Day 5/6 embryo biopsy enables the patient to confirm that their embryos are capable of developing to an advanced stage in culture before proceeding with PGD testing. The alternative is to perform PGD testing on Day 3 with the knowledge that the embryos may not continue to develop and therefore may not be suitable for transfer from an Embryology perspective. Step 5: Genetic testing Following embryo biopsy, the genetic testing can proceed. The genetic testing process will depend on the PGD test type being performed: 1. SNP array testing (performed using “parental support”) In this procedure, the biopsied cells are transferred to a small test tube for genetic testing. The DNA from the embryonic cells is multiplied thousands of times (to generate enough DNA for testing) and is placed on a microarray platform. This microarray platform contains probes for over 300,000 different DNA sites. The DNA from the embryo biopsy sample binds to the DNA probes on the microarray platform. Following binding, it is possible to “read” the DNA code at each of these DNA sites. By screening a blood sample from each partner in parallel with the embryonic cells, it is possible to determine whether each embryo is normal/balanced or unbalanced for the chromosome rearrangement. An analysis of all chromosomes is also performed to determine how many chromosome copies are present in each embryo (Figure 5). Only embryos which are diagnosed as normal/balanced, have the correct number of chormosomes are are developing normally will be considered suitable for transfer. Embryos which are unbalanced and/or have an abnormal number of chromsomes (ie: missing or extra chromosome/s) will not be considered suitable for transfer. Figure 5: PGD testing method using SNP arrays. + Test cell/s DNA from male partner Test DNA DNA from female partner A T G C T T A T G C A T A T G C A T A T G C G C A T G C G G A T G C C C A T G C A T A T G C T A A T G C A T A T G C C A A T G C A C A T G C A A A T G C G G A T G C C G A T G C C G Chromosomes inherited by embryo 2. Array-CGH (performed using 24Sure technology) In this procedure, the biopsied cells are transferred to a small test tube for genetic testing. The DNA from the embryonic cells is multiplied thousands of times (to generate enough DNA for testing) and is then fluorescently labelled. Once labelled, the DNA sample is placed on a microarray platform. This microarray platform consists of a matrix of thousands of different DNA probes which are specific to each chromosome. The fluorescently labelled DNA from the embryo biopsy sample binds to the DNA probes on the microarray platform. By comparing the fluorescent intensity of the embryo biopsy sample with that of a control male and control female sample, it is possible to determine whether each embryo is normal/balanced or unbalanced for the chromosome rearrangement. An analysis of all chromosomes is also performed to determine how many chromosome copies are present in each embryo (Figure 6). Only embryos which are diagnosed as normal/balanced, have the correct number of chormosomes are are developing normally will be considered suitable for transfer. Embryos which are unbalanced and/or have an abnormal number of chromsomes (ie: missing or extra chromosome/s) will not be considered suitable for transfer. Figure 6: Array-CGH procedure + Test cell/s Test DNA 46,XY (male) Control DNA 46,XX (female) Control DNA Loss of fluorescence relative to controls indicates the embryo is missing a portion of one of the translocation chromosomes Same fluorescence as controls indicates the embryo has the normal number of chromosomes Gain of fluorescence relative to controls indicates the embryo has an extra portion of one of the translocation chromosomes 3. FISH testing In this procedure, embryo biopsy must be performed on Day 3 after egg collection. The biopsied cell/s are fixed to a microscope slide for testing. Fluorescent dyes are used to tag the specific chromosomes involved in the chromosome rearrangement. When analysing the cell under a fluorescent microscope, these tags show as coloured dots. The number of coloured dots present in the cell/s is used to indicate whether the embryo is normal/balanced for the chromosome rearrangement or carries an unbalanced form of the chromosome rearrangement (Figure 7). Normal/balanced embryos should have two tags for each chromosome region, whereas unbalanced embryos will have extra or missing tags. This testing will only provide an analysis of the chromosomes involved in the chromosome rearrangement, and will not provide any information on the remaining chromosomes in the embryo. Figure 7: Example of chromosome rearrangement testing using FISH. Normal/balanced cells should have two red signals, two green signals and two aqua signals. Parental Profile (Carrier) Embryo 1 (Normal/Balanced) Embryo 2 (Unbalanced) Embryo 3 (Unbalanced) Step 6: Embryo transfer The time of embryo transfer will also be dependent upon the PGD test type performed, as follows: 1. SNP array testing (performed using “parental support”) Because of the time taken to perform the genetic testing, the embryos must be frozen following biopsy. Final results are usually available 2 to 3 weeks after biopsy. If available, one or two normal/balanced embryos can be thawed for use in a frozen embryo transfer cycle. A PGD scientist/Embryologist will discuss the PGD results with the patient prior to transfer. The patient’s IVF nurse will organise a pregnancy test to be performed on Day 16 of the frozen embryo transfer cycle. This process should increase the chance of a successful pregnancy and significantly reduce the risk of miscarriage. Surplus normal/balanced embryos will remain in storage. These embryos may be used in a subsequent cycle. Chromosomally abnormal embryos will be removed from storage and allowed to succumb. 2. Array-CGH (performed using 24Sure technology) Embryo transfer is performed using the same process as outlined for the SNP array testing. 3. FISH testing Final results are usually obtained 24 hours after biopsy. The embryo is kept in culture while testing of the biopsied cell/s proceeds. Embryos identified as being normal/balanced for the chromosome rearrangement can be transferred fresh on Day 5 of development. A PGD scientist/Embryologist will discuss the PGD results with the couple prior to transfer. The couple’s nurse will organise a pregnancy test to be performed on Day 16 of the cycle. This process should increase the chance of a successful pregnancy and significantly reduce the risk of miscarriage. When a number of normal/balanced embryos are identified, morphological criteria are also used to select the best embryo/s for transfer. Surplus normal/balanced embryos which are not transferred but which continue to develop satisfactorily to the blastocyst stage may be frozen. These embryos may be used in a subsequent IVF cycle. Chromosomally abnormal embryos are allowed to succumb. Why choose Monash IVF for PGD? Monash IVF has offered PGD as a clinical service since 1996 and is one of the few centres in Australia that specialises in this area of reproductive medicine. In 1996 we were proud to report the birth of Australia’s first PGD babies and since then we have performed over 3,000 PGD cycles with proven high success rates. Our specialised genetics team contains highly qualified experts in PGD, ensuring the best quality of care for patients. The genetics team at Monash IVF is responsible for providing a specialised PGD service not only to our own patients, but also to patients undergoing IVF cycles at fourteen different IVF clinics throughout Australia and New Zealand. While the main PGD laboratory is located in Clayton, Melbourne, Australia, embryo biopsy can be performed away from the genetics laboratory and the embryonic cells sent by courier to Clayton. Centralising the genetic testing enables patients to access the highest levels of expertise without having to leave their home state. Where can I get more information? If you would like further information regarding the PGD program at Monash IVF, please feel free to contact a member of the Genetics team on +61 3 9543 2833.