My thoughts re rehab programme pilot

O72
RENAL GRAFT OUTCOMES AFTER PREGNANCY: FOLLOW-UP FROM THE UK
OBSTETRIC SURVEILLANCE STUDY
Kate Bramham 1 , Marian Knight 2 , Kate Wiles 1 , David Bull 3 , Philip Webster 4 , Catherine
Nelson-Piercy 1
1
King’s Health Partners AHSC,
2
National Perinatal Epidemiology Unit,
3
UK Renal
Registry,
4 MRC Clinical Sciences Centre,
Imperial College London
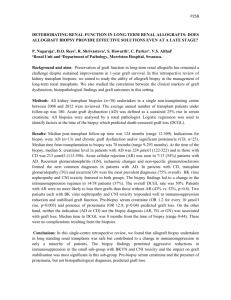
INTRODUCTION: Obstetric outcomes for women with renal transplants have recently been reported by a UK Obstetric Surveillance System (UKOSS) study. Pregnancy may be associated with an accelerated decline in graft function; however reports of postpartum graft outcomes are limited by small numbers from single centres, and few are contemporaneous reflecting current therapeutic strategies. Risk factors for graft loss are unknown.
METHODS: Women recruited in the UKOSS renal transplant study (Deliveries between 2007-
9) were matched with outcome data from the UK Renal Registry. Creatinine concentrations post delivery and timing of graft failure were recorded. Follow-up period was calculated from time of delivery/miscarriage to date of most recent creatinine recorded or graft loss. Risk factors for graft loss were compared between those with functioning and failed grafts and independent predictors identified with regression analysis.
RESULTS: 71/105 (68%) women were matched with Renal Registry data. 16 (22%) women developed graft failure during the follow-up period. The incidence of graft survival (78%) is comparable with National data (UK NHS Blood and Transplant) at 10 years - 59%, 71% and
78% in DCD, DBD and living donor grafts respectively. Five graft failures (7%) occurred within 12 months postpartum. There was no difference in maternal age, ethnicity, BMI, live donor allograft or time from transplantation to conception between women with functioning and failed grafts. Incidence of pre-eclampsia, maternal ITU admission, episodes of acute kidney injury, mode of delivery, gestation at delivery and infant birth-weight were also not significantly different. Pre-pregnancy creatinine and more than one previous transplant were identified as independent predictors of graft failure.
Women with functioning grafts had median (IQR) changes in creatinine of +3µmol/L (-11, +22) and -23 µmol/L (-85, 9.5) at 6 months postpartum and at most recent follow-up respectively compared to pre-pregnancy values.
Table 1: Risk factors for postpartum graft loss
Functioning Graft
N=55
Failed graft
N=16
Time of delivery to graft failure/most recent creatinine
Months (Median, IQR)
Total length of graft function
Months (Median, IQR)
Time from transplantation to conception
Months (Median, IQR)
Pre-pregnancy Creatinine
µmol/L (Median, IQR)
56 (44, 62)
111 (86, 184)
(9.25 years)
50 (24,120)
110 (94, 130)*
22 (9, 41)
108 (75, 137)
(9 years)
71 (34, 101)
120 (107, 192)*
Second or more transplant 6 (11%)* 8 (50%)*
*p<0.05
CONCLUSION: Pregnancy does not appear to affect graft survival. The majority of graft loss after pregnancy occurred after 12 months postpartum. Independent predictors of postpartum graft loss were pre-pregnancy serum creatinine and having more than one renal transplant.