Vitamin B12 testing

MBS Review
Vitamin B12 Testing
Protocol
July 2013
CONTENTS
APPENDIX B - SEARCH TERM STRATEGY ............................................................... 21
ABBREVIATIONS
MMA ng/ml
NTD oz
PA
PASC
PBS pg/ml
PICO
Pmol/L
RBC
RCC
RDA
TGA
DNA
ESC
FDA
HPLC holoTC
IF
MSAC
MBS
µg
AD
AIHW
ANZFSC
CMFM
CoA
CVD
Department
Microgram
Alzheimer’s Disease
Australian Institute of Health and Welfare
Australia and New Zealand Food Standards Code
Comprehensive Management Framework for the MBS
Coenzyme A
Cardiovascular disease
Department of Health and Ageing
Deoxyribonucleic acid
Evaluation Sub-Committee (of MSAC)
Food and Drug Administration
High performance liquid chromatography
Holotranscobalamin II
Intrinsic factor
Medical Services Advisory Committee
Medicare Benefits Schedule
Methylmalonic acid
Nanogram per millilitre
Neural Tube Defects
Ounce
Pernicious anaemia
Protocol Advisory Sub-Committee
Pharmaceutical Benefits Scheme
Picogram per millilitre
Population, intervention, comparator, outcome
Picomole per Litre
Red Blood Cell
Review Consultation Committee
Recommended Dietary Allowance
Therapeutic Goods Administration
1
INTRODUCTION TO MBS REVIEWS
In the 2011-12 Budget, the Australian Government committed to continue the systematic review of Medicare Benefits Schedule (MBS) items to ensure that they reflect contemporary evidence, improve health outcomes for patients and represent value for money under the
Comprehensive Management Framework for the MBS (CMFM).
Reviews support the public funding of evidence-based, cost-effective clinical practice through the MBS.
The MBS Reviews process includes the consideration of policy issues related to services funded under the MBS and is designed to have flexibility depending on the complexity of the issues pertaining to the particular review. For example, where there is a single MBS item or service the review may be focussed and timeframes may not be as exhaustive as a review that include multiple MBS items with related policy issues or non MBS issues. Non MBS issues that require a different process (such as pharmaceuticals or prostheses), and policy issues that are not appropriately dealt with by the Medical Services Advisory Committee (MSAC) process will be identified and addressed in separate processes which will inform the review.
The first stage of a review is the identification of the scope. Reviews with single MBS services/issues will follow the MBS pathway and will be considered by MSAC using the
MSAC process. For reviews with multiple MBS services or a specialty and policy issues, the scope and pathway (MBS pathway and policy pathway) will be confirmed by the Review
Consultation Committee (RCC), a time limited committee of nominated experts, determined and chaired by the Department.
The MBS pathway will follow the MSAC process and include the:
development of a protocol;
collection and evaluation of evidence; and
advice and recommendations to the Minister through the Department.
The pathway for policy and other issues depends on the issues identified in the scope. There will be interactions between the MBS and policy pathways and stakeholders will be consulted throughout the review process; ensuring alignment of processes and consistency in deliberations.
The engagement with stakeholders is a critical component of the reviews process and issues will be dealt with in a consultative fashion. The role of the RCC is advising the Department on policy issues and the MSAC and its subcommittees is advising on MBS matters. The review process is flexible, ensuring that new and emerging issues and feedback from the
RCC, MSAC or public consultations can be incorporated into the reports.
The advice and recommendations provided by the CRC and MSAC to the Department informs the advice for the Minister.
2
Principles to Guide MBS Reviews
Reviews will:
have a primary focus on improving health outcomes and the financial sustainability of the
MBS, through consideration of areas potentially representing:
patient safety risk;
limited health benefit; and/or
inappropriate use (under or over use)
be evidence-based and fit-for-purpose;
be conducted in consultation with key stakeholders including, but not limited to, the medical profession and consumers;
include opportunities for public submission;
be published; and
use Government resources efficiently.
Objectives of the Review
To ensure the clinical and financial sustainability of the MBS, reviews will assess specific services or MBS item(s) and associated policy issues in a focused, fit-for-purpose, evidence based process. Findings will recognise that MBS funding should align with contemporary evidence, reflecting appropriate patient groups and best clinical practice.
Purpose of the Protocol
This document outlines the methodology for providing evidence based analysis to support the review of services for vitamin B12 testing, specifically the frequency of testing and the appropriate patient population for testing. The Protocol outlines the review methodology, clinical research questions the review will focus on, methods to identify and appraise the evidence and key stakeholder groups and experts to be consulted during the conduct of the review.
Stakeholder Consultations
The Department is responsible for the review process including documents developed for policy and MBS issues and contractual arrangements for the development of the protocol and other report documents for the review. This includes ensuring that the relevant documents are available online for public consultation at the appropriate time and that comments are incorporated into informing the review process.
The Department’s management of stakeholder engagement and negotiations with the relevant medical craft groups and key stakeholders will ensure the review findings are informed by consultations.
Following the finalisation of the review process, the advice to the Minister for Health on the findings of the review will be informed by the review reports, advice and recommendations from MSAC and RCC, public consultations and also other information that is relevant to the review including budgetary considerations.
Questions to be delivered to the RCC include, but are not limited to the following:
(1) Is vitamin B12 testing appropriate for MBS reimbursement?
3
(2) What are the expected patient health outcomes with regard to patient groups, type of intervention and practitioners ordering and performing (accreditation and training) the vitamin B12 testing?
(3) What are the clinical indications for medically necessary vitamin B12 testing?
(4) Are current assays used for the detection of serum vitamin B12 levels accurate and reflect the true status of vitamin B12 in the Australian population?
(5) What are the safety, efficacy, effectiveness of the tests and the effect that the results of the test have on treatment?
Public Consultations
The invitations to the general public (which include all stakeholders - patients, consumer groups, individual service providers, health professionals and manufacturers) to provide comment on the draft documents during the review process are critical to the review process.
The documents will be available on the MSAC website ( www.msac.gov.au
) inviting the public to submit written comments over a four week period. The purpose of the feedback is to inform the final reports and recommendations to the Minister.
Medical Craft Groups / Key Stakeholders
The following clinical craft groups and key stakeholders have been identified as having an interest in this review:
Osteoporosis Australia;
IVD Australia;
Australia and New Zealand Bone and Mineral Society;
Endocrine Society of Australia;
National Prescribing Network;
Australian Association of Pathology Practices;
Australian Medical Association;
Consumers Health Forum of Australia;
National Coalition of Public Pathology;
Royal Australian College of General Practitioners; and
Royal College of Pathologists of Australasia.
4
BACKGROUND
Mechanism of vitamin B12 absorption
Vitamin B12, also called cobalamin, is a water soluble vitamin that plays a fundamental role in the normal functioning of the brain and nervous system, and for the formation of blood.
Dietary vitamin B12, obtained from animal food, is bound to animal protein. The acid and pepsin in the stomach breakdown these protein and release vitamin B12. The free vitamin
B12 then binds a protein called haptocorrin (previously known as Transcobalamin I or R-
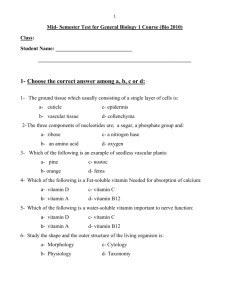
Factor or R-protein), which is produced by the salivary glands and parietal cells of the stomach whose essential function is to protect vitamin B12 from degradation from the acidic environment of the stomach. In the duodenum, the pancreatic enzymes degrade the haptocorrin, and vitamin B12 is released again which then binds to the intrinsic factor (IF) produced by parietal cells. Absorption of vitamin B12 occurs in the terminal ileum (i.e. most distal part of the small intestine) and is aided by binding the complex to the IF receptor on the mucosal surface (Figure 1). In addition to this method of absorption, evidence supports the existence of an alternate pathway that is independent of the IF. This pathway is important in relation to oral supplementation (approximately 1% of a large oral dose of vitamin B12 is absorbed by this second mechanism)
Once absorbed, vitamin B12 is bound to two carrierproteins in blood: haptocorrin and transcobalamin .The majority of vitamin B12 (70-80%) is bound to haptocorrin (named as holo-haptocorrin) and is not biologically active. Only less than 30% of the B12 is bound to trascobalamin II (named as holo-transcobalamin (HoloTC)) which is the active fraction that enters cells for metabolic reactions. Details of these carrier proteins will be discussed later. The interruption of one or any combination of these steps places a person at risk of developing vitamin B12 deficiencies.
Figure 1: Vitamin B12 absorption and transport
5
Functions of vitamin B12 in the human body
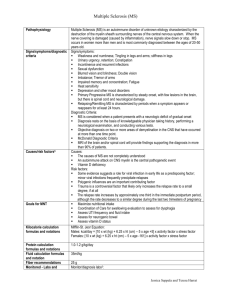
In humans, vitamin B12 and folate are linked by two enzymatic reactions where they function as cofactors (i.e. a cofactor is a component, other than the protein portion, of many enzymes to facilitate the catalytic activity of the enzyme)
. Vitamin B12 is required as a cofactor in both reactions, whereas folate is required in only one of the reactions (see Figure 2).
Figure 2: The enzymatic reactions that require vitamin B12 and folate (folic acid) as cofactors
In the first reaction, vitamin B12 is required for the conversion of methylmalonic acid
(MMA) to succinyl-CoA. MMA is a substance produced when proteins in the body are broken down.
Folate does not play any role in this reaction. Deficiency in vitamin B12 can lead to increased levels of serum MMA.
In the second reaction, both vitamin B12 (in the form of methylcobalamin) and folic acid act as cofactors in the conversion of the substrate homocysteine (a homologue of the amino acids cysteine and methionine) to methionine (an amino acid and one of the 20 building blocks of proteins) by the enzyme methionine synthase.
More importantly, this pathway is closely linked to the generation of thymidine which is vital for deoxyribonucleic acid (DNA, i.e. the building block of the human body which carries genetic information) synthesis. A deficiency in either vitamin B12 or folic acid or both can lead to increased homocysteine levels in plasma.
In addition, deficiency of either vitamins can result in perturbation of these two key pathways with consequent disruption of DNA synthesis caused by thymidine lack and resulting in megaloblastic anaemia, as well as other adverse effects on the nervous system and other organs.
It is this metabolic reaction that clearly links the two vitamins and is
6
responsible for the common or shared neuropsychiatric and haematologic disorders discussed in the following sections.
Vitamin B12: dietary sources, fortification, and supplements
Vitamin B12 is present in animal products such as meat, poultry, fish (including shell fish), and to a lesser extent milk, cheese and eggs, and it is not present in plant products.
The recommended dietary allowance for vitamin B12 is 2.4 µg/day
and most individuals can meet this level through dietary intake.
Table 1 lists some of the foods with substantial amounts of vitamin B12 along with their vitamin B12 content. Individuals over the age of 50 who have reduced protease secretions in the stomach (as well as strict vegetarians)
obtain their vitamin B12 from supplements or fortified foods (e.g. fortified cereal) because of the increased likelihood of food-bound vitamin B12 malabsorption.
Table 1: Examples of dietary sources of vitamin B12 and folate
Type of food
Clams, 3 oz (85 grams)
Mussels, 3 oz
Crab, 3 oz
Salmon, 3 oz
Beef, 3 oz
Chicken
Egg (whole)
Milk (8 oz, 1 glass)
Estimated vitamin B12 content (micrograms
µg)
84.0
20.4
8.8
2.4
2.1
0.3
0.6
0.9
Food fortification is defined as the process of adding micronutrients (such as vitamins and minerals) to food as permitted by the Australian and New Zealand Food Standards Code
(ANZFSC).
Regulations regarding the fortification of foods with vitamin B12 vary between countries. ANZFSC permits only a limited number of foods to be fortified with vitamin B12. This includes selected soy milks, yeast spread, and vegetarian meat analogues.
The risk of toxicity from vitamin B12 intake from supplements and/or fortified foods is low.
Vitamin B12 is a water soluble vitamin, and therefore any excess intake is usually excreted in the urine.
Causes of vitamin B12 deficiencies
Table 2 describes causes of vitamin B12 deficiencies which can be divided into four categories: nutritional deficiency, increased requirements, impaired absorption, and other gastrointestinal causes.
Table 2: Causes of vitamin B12 deficiencies
Nutritional deficiency
Poor intake of meats and dairy products in the elderly
population (aged 65
Strict vegan diets
Increased requirements
Due to pregnancy
Impaired absorption
Autoimmune disease with autoantibodies against the intrinsic factor (pernicious
Atrophic body gastritis (due to
Other gastrointestinal causes
Chronic gastrointestinal symptoms e.g. dyspepsia, recurrent peptic ulcer,
7
Malnutrition
and avoidance of fortified bread due to coeliac disease
autoantibodies to gastric parietal
Gastrectomy
Prolonged use of acid-suppression therapy or drugs
Patients with intestinal surgery gastric resection, sleeve or banding
Tapeworms and other intestinal
Ileocystoplasty (i.e. a surgical reconstruction of the bladder involving the use of an isolated segment of ileum to augment bladder capacity)
Vitamin B12 deficiency is usually the result of dietary insufficiency and is common in individuals who are strict vegetarians because vitamin B12 is only present in foods from animal origin. Because of the complex mechanism of vitamin B12 absorption, causes of malabsorption may also arise at several levels in the gastrointestinal tract.
At the gastric level, the most frequent cause of significant vitamin B12 malabsorption leading to deficiency is pernicious anaemia (PA), which is an autoimmune disorder caused by the frequent presence of gastric autoantibodies directed against IF and the parietal cells.
PA can affect both the elderly and young individuals.
Diseases caused by Vitamin B12 deficiencies
Vitamin B12 plays an important role in DNA synthesis and neurologic function.
Deficiency in vitamin B12 is associated with a wide spectrum of haematologic, neurologic and psychiatric disorders (Table 3) that can often be reversed by early diagnosis and prompt treatment.
Table 3: Clinical manifestations of vitamin B12 deficiencies
Megaloblastic
Neurologic
Paresthesias (i.e. a
Psychiatric
Irritability, anaemia
Panycytopenia
(Leukopenia, thrombocytopenia)
Pernicious anaemia
(i.e. large immature
RBCs) skin sensation such as burning or itching with no apparent physical cause)
Peripheral neuropathy
Combined systems personality change
Mild memory impairment, dementia
depression
psychosis
Alzheimer’s
Disease (48) disease
(demyelination of peripheral nerves, spinal cord, cranial nerves and the brain)
Vitamin B12 testing
Possible increased risk of myocardial infarction and stroke
Reliable and accurate assessment of vitamin B12 and folate status is required to determine the prevalence of deficiencies of these two vitamins in the Australian population and is necessary
8
for developing suitable strategies to prevent these nutritional problems. The haematologic complications of folate and vitamin B12 deficiencies are identical. Therefore, detecting the presence of folate or vitamin B12 deficiency, and distinguishing one from the other, depends critically on laboratory testing. These tests may be used singularly or in combination to establish the nutritional status and prevalence of deficiencies of the vitamins.
The methods used to assess folate and vitamin B12 status can either measure the:
concentrations of the vitamins in the blood (e.g. serum vitamin B12 levels, serum or plasma folate levels); and/or
increased levels of metabolites such as MMA and/or homocysteine.
The diagnosis of vitamin B12 deficiency has traditionally been based on measuring the total serum levels of vitamin B12. There is currently no internationally agreed definition for vitamin B12 deficiency based on clinical manifestations or on the ‘cut-off’ values that are used to define vitamin B12 deficiency which vary between 120-200 pmol/L. These could be partly because the analytical methods for vitamin B12 are not standardised and the results are variable among different methods. In addition, vitamin B12 carrier protein concentrations can vary in different individuals. Vitamin B12 is carried on two distinct binding proteins in plasma.
Transcobalamin II: binds vitamin B12 to form a complex called holotranscobalamin
(holoTC). HoloTC binds only 20–30% of vitamin B12 circulating in the blood, but is responsible for delivery of vitamin B12 to cells and is considered to be the functionally important fraction, thus it is named “active-B12” in layman’s term. HoloTC levels fall in vitamin B12 deficiency. Therefore, testing for HoloTC can identify low vitamin B12 status before total serum vitamin B12 levels drop.
Haptocorrin: binds the major portion of plasma vitamin B12 which is essentially inert as far as vitamin B12 delivery to cells is concerned, although it may reflect the general underlying state of vitamin B12 stores. The complex formed by the binding of haptocorrin to vitamin B12 is called holo-hapctocorrin (HoloHC)
. Haptocorrin deficiency is associated with low serum vitamin B12 concentrations.
Research has shown that assays that measure holoTC
are a more reliable indicator for identifying vitamin B12 deficiency, when used in conjunction with other available tests, such as serum MMA or homocysteine measurements.
Currently available assays to measure holoTC are developed by Axis-Shield. This company recently launched a new active-B12 assay (Abbott ARCHITECT) for use in high throughout laboratories.
MMA and homocysteines are functional markers of vitamin B12 status and levels increase when vitamin
B12 deficiency is present. They are particularly useful when HoloTC or total vitamin B12 are in the equivocal range and vitamin B12 deficiency can not be ruled out with confidence.
However, many other causes in addition to vitamin B12 deficiency can also raise MMA and homocyseine. These tests have very high negative predictive value, however, when their levels are elevated, other causes need to be excluded first before vitamin B12 deficiency can be made. MMA (in blood or urine specimens) can be measured using high performance liquid chromatography (HPLC)
but the test is not readily available in Australia. Serum homocysteine can be performed in most of the laboratories in Australia.
Table 4 compares the three tests that can be used to assess vitamin B12 status.
Table 4: Comparison of the three tests used to measure vitamin B12
9
Biomarkers
Assessing intake
Sensitivity
Specificity
Assessing long term and short term status of vitamin
B12
Serum/plasma B12
+
+
--
+
Long term status
Serum holoTC
++
+
-
++
Long term and short term status
Serum/plasma MMA
++
++
+
++
Long term and short term
Accepted cutoffs indicating deficient states
Subclinical deficiency: vitamin
B-12 <300 pg/mL
(<220 pmol/L)
TC <35 pmol/L >260 nmol/L deficient
Table 4 shows that sensitivity of serum vitamin B12 measurement for detection of vitamin
B12 depletion or deficiency is good overall, but specificity is poor, and the predictive value is improved when this test is combined with measurement of MMA. One study has shown that the use of a low serum vitamin B12 level as the sole means of diagnosis of vitamin B12 deficiency may miss up from 10 to 26% of patients with actual tissue B12 deficiency.
The holoTC assay used on its own is also not very predictive of vitamin B12 deficiency unless it is used in conjunction with plasma MMA or with the total plasma vitamin B12, and when combined may provide enhanced predictive power to identify true vitamin B12 deficiency.
The availability of the holoTC assay is currently somewhat limited. Therefore, for an accurate measure of vitamin B12 status and reserves, it is recommended that serum vitamin
B12 levels are combined with a measure of a metabolic marker of vitamin B12 reserves such as MMA, holoTC or homocysteine.
Serum vitamin B12 target values
The cut-off value for vitamin B12 deficiency varies markedly between laboratories worldwide. Table 5 presents the “usual or approximate” reference intervals for vitamin B12 deficiencies.
Table 5: Vitamin B12
reference intervals
Status
Vitamin B12 (pg/ml)†
Normal range 200-900 (130-850 pmole/L)
Deficient < 200* (< 130 pmol/L)
* This is an unsafe range as many in the population exhibit neurological symptoms of deficiency at much higher concentrations. The lowest concentration to be considered normal is 221 pmol/L.
† pmol/L = 0.738xpg/ml
(82)
As discussed earlier, elevated homocysteine levels can be a useful indicator for vitamin B12 deficiency, because serum homocysteine levels increase as vitamin B12 stores fall. Serum homocysteine levels greater than nine µmol/L suggest the beginning of depleted vitamin B12 reserves and levels greater than 15 µmol/L is indicative of depleted vitamin B12 reserves.
However, caution should be taken with this test as homocysteine levels may also increase with folate deficiency.
Prevalence of Vitamin B12 deficiencies in Australia
The true prevalence of vitamin B12 deficiency in the general Australian population remains unknown. The incidence appears to increase with age (>65 years) and with the ubiquitous use of gastric acid–blocking agents.
An Australian study published in 2012 found 14% of
130 patients living in residential aged care facilities in southern Tasmania were vitamin B12 deficient, with serum B12 levels less than 150 pmol/L.
Another study published in 2006
10
examined the prevalence of low serum vitamin B12 in a representative sample of 3,508 persons aged 50+ years between 1997 and 2000.
Low serum vitamin B12 (< 185 pmol/L) was found in 22.9% of participants.
11
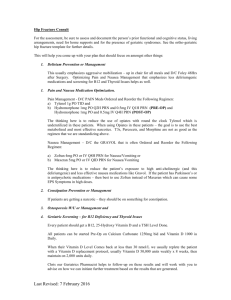
Clinical Flow Chart
The clinical decision pathway which determines whether vitamin B12 testing should be undertaken is provided in Figures 3.
Figure 3: Clinical flow chart for vitamin B12 testing
Patient presents to clinician (e.g. General
Practitioner, Obstetrician etc)
Does the patient have any of the following clinical symptoms of vitamin B12 deficiency?
Does the patient have any of the following risk factors associated with vitamin B12 deficiency?
Neuromotor symptoms including:
•
Paresthesia; or
• Ataxia; or
•
Decreased reflexes; or
•
Restless leg syndrome; or
• Peripheral neuropathy.
Neuropsychiatric symptoms including:
•
Dementia
• Depression
•
Psychosis
•
Personality changes
• Vegetarians
•
Patients >65
• Institutionalised patients or patients in aged care facilities
•
Newborn children of vegetarian or malnourished mothers
•
Gastric surgery patients
• Atrophic gastritis patients
•
H. Pylori infected patients
• Patients with gastrointestinal disorders e.g. Crohn’s, Coeliac disease
Does the patient have any of the following haematological symptoms of vitamin B12 deficiency?
Haematological symptoms including:
• Anaemia
•
Macrocytic anaemia
•
Macrocytosis
• Pernicious anaemia
Yes No
Patient ineligible to claim benefits under MBS item numbers 66599 or 66602
No
No Yes Is Vitamin B12/folate testing medically necessary?
Yes
Measure Vitamin B12 and claim MBS item number
66599
Is Vitamin B12/folate testing medically necessary?
No
Patient ineligible to claim benefits under MBS item numbers 66599 or 66602
Yes
Measure Vitamin B12/ and/or folate and claim
MBS item number 66602
12
METHODOLOGY
The main methodology for the review will be mini-health technology assessments:
a comprehensive systematic search of the scientific literature will be conducted to identify relevant studies addressing the key clinical/research questions.
To translate the evidence into the Australian context, the review will consider:
Secondary data analysis: o MBS and National Hospital Morbidity data will be analysed to examine the existing population utilisation of services and assess whether existing MBS item numbers for the services are appropriate.
Guideline concordance: o an analysis of the MBS services will be assessed relative to ‘best practice’ as recommended in relevant Clinical Practice Guidelines and relevant practice in
Australia.
Stakeholder consultation: o clinician engagement (e.g. CRC, MESP and submission authors) to understand existing services and practices in Australia; and o consumer engagement to determine consumer experiences with the services under review.
Economic evaluation o preliminary economic evaluation will be conducted as part of the review, relying on studies identified through the systematic literature review.
The above information will take on additional significance when there is a lack of clear, high quality evidence.
Population, Intervention, Comparator, Outcomes (PICO)
The PICO (Population, Intervention, Comparator, Outcomes) criteria
are used to develop well-defined questions for each review. This involves focusing the question on the following four elements:
the target population for the intervention;
the intervention being considered;
the comparator for the existing MBS service (where relevant); and
the clinical outcomes that are most relevant to assess safety and effectiveness.
The PICO criteria have been determined on the basis of information provided in the literature, as well as clinical advice. These criteria will be applied when selecting literature for these mini-HTAs. Additional criteria for selecting literature have also been outlined (i.e. relevant study designs for assessing the safety and effectiveness of the service, time period within which the literature will be sourced, and language restrictions as discussed above and in appendix C). The PICO for the review of vitamin B12 testing are shown in Table 6.
13
Table 6: Clinical research questions for the vitamin B12 testing
Intervention Comparator Population
(1) General Health population
(includes pregnant women, elderly, alcoholics, vegetarians)
(2) Infants with metabolic disease
(3) Patients with anaemia and haematologic diseases
(4) Patients with neurologic disease
(5) Patients with gastrointestinal and malabsorption disorders
Vitamin B12 testing Supplementation
Outcomes
Safety
Complications associated with the procedure (e.g. infection, needle injuries)
Effectiveness
Physical health outcomes as a consequence of the procedure
(e.g. all-cause mortality, anaemia, NTDs, CVD, neuropathy, depression and dementia).
(6) Patients with psychiatric disorders
Literature review
A comprehensive search of the scientific literature will be conducted to identify relevant studies addressing the key questions. The databases to be included in the search are:
MEDLINE® (from 1966 to present), MEDLINE® In-Process & Other Non-Indexed
Citations, EMBASE (Excerpta Medica published by Elsevier), the Cumulative Index to
Nursing & Allied Health Literature (CINAHL) and Cochrane databases. The search will be restricted to English language studies of humans. In electronic searches we will use various terms for, limited to humans, and relevant research designs as shown in Appendix 1.
Reference lists of related systematic reviews and selected narrative reviews and primary articles should be reviewed. Databases maintained by health technology assessment (HTA) agencies should be reviewed to identify existing assessments of vitamin B12 testing. In terms of supplementary search strategies, as part of consultations with pathologists and general practitioners, they should be asked if they are aware of any clinical guidelines, unpublished studies, reviews relevant to the review of vitamin B12 testing.
The research questions to be addressed as part of the review protocol using the literature review include:
(1) What are the appropriate clinical indications for medically necessary vitamin B12 testing?
(2) What is the strength of evidence for the effectiveness of vitamin B12 testing in improving outcomes in each target population (e.g. children, pregnant women, elderly, vegetarians, patients with hematologic and neurologic disorders) across the patient journey?
(3) What are the safety and quality implications (including morbidity, mortality and patient satisfaction) associated with vitamin B12 testing in each target population? How do safety and quality outcomes of vitamin B12 testing vary according to: a.
the difference in testing methodologies? b.
frequency of testing?
14
(4) What is the evidence regarding the cost implications associated with vitamin B12 testing services in each target population across the patient journey?
(5) What is the evidence regarding the cost implications associated with vitamin B12 testing in each target population compared with not testing?
MBS data
MBS data are available for MBS item numbers 66599 and 66602 since the early 1990s. A brief review of the available MBS data for the purposes of drafting the Review Protocol identified an overall increase in claims for vitamin B12/folate testing. The clinical/research questions to be addressed as part of the review using MBS data include: a.
How frequent are claims for the MBS item numbers under review (66599 and 66602)? b.
Are there any age, sex, temporal or geographic trends associated with usage of these item numbers? c.
What are the characteristics of patients undergoing vitamin B12/folate testing? d.
Are the Medicare claims data consistent with trends in the incidence/prevalence of the conditions/diseases being addressed by the services? e.
What is the prescriber profile of benefits claimed for vitamin B12/folate testing? f.
Are there other pathology tests claimed in association with vitamin B12/folate testing?
Guideline concordance
An analysis of the two vitamin B12 testing MBS item numbers will be assessed relative to
‘best practice’ as recommended in relevant clinical practice guidelines and relevant practice in Australia. Where formalised clinical practice guidelines do not exist, the review should take account of other guidelines in operation in comparable health systems overseas.
Differences in the purpose and intended audience of any such guidelines should be considered, documented and acknowledged in the process of undertaking the review.
The clinical/research questions to be addressed as part of the review using guideline concordance include:
(1) Is the descriptor for the MBS items 66599 and 66602 consistent with evidence-based (or in the absence of evidence, consensus-based) recommendations provided in relevant clinical practice guidelines?
Economic evaluation
Only a preliminary economic evaluation will be conducted as part of conducting the review, relying on studies identified through the systematic literature review. In the literature searches, acceptable evidence would include trial-based costing studies, cost analyses and economic modelling studies. Acceptable outcomes would include: cost, incremental costeffectiveness ratio e.g. cost per event avoided, cost per life year gained, cost per quality adjusted life year or disability adjusted life year. The applicability of any identified economic analyses to the Australian health system will be assessed.
The clinical/research questions to be addressed as part of the review using the economic evaluation component include:
(1) What is the evidence regarding the cost implications associated with vitamin B12 testing in each target population across the patient journey?
(2) Is the current fee structure associated with these items appropriate?
15
REFERENCES
1.
2.
3.
4.
5.
6.
7.
Elia M. Oral or parenteral therapy for B12 deficiency. Lancet. 1998 Nov 28;352(9142):1721-2.
Oh R, Brown DL. Vitamin B12 deficiency. American family physician. 2003 Mar 1;67(5):979-86.
Wikipedia. Cofactor (biochemistry). 2012; Available from: http://en.wikipedia.org/wiki/Cofactor_(biochemistry) .
Stabler SP. Screening the older population for cobalamin (vitamin B12) deficiency. J Am Geriatr Soc.
1995 Nov;43(11):1290-7. center UoMM. Methylmalonic acid. 2012; Available from: http://www.umm.edu/ency/article/003565.htm
.
Green R. Indicators for assessing folate and vitamin B-12 status and for monitoring the efficacy of intervention strategies. Am J Clin Nutr. 2011 Aug;94(2):666S-72S.
Medicine Io, Board FaN. Dietary Reference Intakes: Thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin, and choline. Washington, DC1998.
8.
9.
National Health and Medical Research Council, Health. NZMo. Nutrient reference values for Australia and New Zealand including recommended dietary intakes. Canberra, ACT2006; Available from: http://www.nhmrc.gov.au/guidelines/publications/n35-n36-n37 (accessed May 2012). .
Watanabe F. Vitamin B12 sources and bioavailability. Exp Biol Med (Maywood). 2007
Nov;232(10):1266-74.
10. Gilsing AM, Crowe FL, Lloyd-Wright Z, Sanders TA, Appleby PN, Allen NE, et al. Serum concentrations of vitamin B12 and folate in British male omnivores, vegetarians and vegans: results from a cross-sectional analysis of the EPIC-Oxford cohort study. Eur J Clin Nutr. 2010 Sep;64(9):933-9.
11. US Department of Agriculture ARS. USDA National Nutrient Database for Standard Reference, Release
24. 2011; Available from: http://www.ars.usda.gov/ba/bhnrc/ndl .
12. Food Standards ANZ. Adding vitamins and minerals to food. 2012; Available from: http://www.foodstandards.gov.au/consumerinformation/fortification.cfm
.
13. Zealand FSAN. NUTTAB 2010 online searchable database. 2012; Available from: http://www.foodstandards.gov.au/consumerinformation/nuttab2010/nuttab2010onlinesearchable database/onlineversion.cfm (accessed Nov 2011). .
14. Hathcock JN. Vitamins and minerals: efficacy and safety. Am J Clin Nutr. 1997 Aug;66(2):427-37.
15. Snow CF. Laboratory diagnosis of vitamin B12 and folate deficiency: a guide for the primary care physician. Arch Intern Med. 1999 Jun 28;159(12):1289-98.
16. Mangels R MV, Messina M. The dietitians’ guide to vegetarian diets: issues and applications. 3rd ed.
Sudbury M, editor: Jones & Bartlett Learning; 2010.
17. Halsted CH. Folate deficiency in alcoholism. Am J Clin Nutr. 1980 Dec;33(12):2736-40.
18. Lindenbaum J. Folate and vitamin B12 deficiencies in alcoholism. Semin Hematol. 1980 Apr;17(2):119-
29.
19. Nkrumah FK, Nathoo KJ, Sanders DM. Iron, folate and vitamin B12 in severe protein-energy malnutrition. Cent Afr J Med. 1988 Mar;34(3):39-43.
20. Thompson T. Folate, iron, and dietary fiber contents of the gluten-free diet. J Am Diet Assoc. 2000
Nov;100(11):1389-96.
21. Malterre T. Digestive and nutritional considerations in celiac disease: could supplementation help?
Altern Med Rev. 2009 Sep;14(3):247-57.
22. Higgins JR, Quinlivan EP, McPartlin J, Scott JM, Weir DG, Darling MR. The relationship between increased folate catabolism and the increased requirement for folate in pregnancy. Bjog. 2000
Sep;107(9):1149-54.
23. Gueant JL, Safi A, Aimone-Gastin I, Rabesona H, Bronowicki JP, Plenat F, et al. Autoantibodies in pernicious anemia type I patients recognize sequence 251-256 in human intrinsic factor. Proc Assoc Am
Physicians. 1997 Sep;109(5):462-9.
24. Kaushansky K BE, Seligsohn U, Lichtman MA, Kipps TJ, Prchal JT,. Folate, cobalamin, and megaloblastic anemias. 8th ed ed. R. G, editor. New York: McGraw-Hill; 2010.
25. Sipponen P, Laxen F, Huotari K, Harkonen M. Prevalence of low vitamin B12 and high homocysteine in serum in an elderly male population: association with atrophic gastritis and Helicobacter pylori infection.
Scand J Gastroenterol. 2003 Dec;38(12):1209-16.
26. Green R MJ. Handbook of Vitamins. 4th ed. Zempleni J RR, editor. Boca Raton, FL: Taylor & Francis
Group; 2007.
27. Schubert ML. Gastric secretion. Curr Opin Gastroenterol. 2007 Nov;23(6):595-601.
28. Ponziani FR, Cazzato IA, Danese S, Fagiuoli S, Gionchetti P, Annicchiarico BE, et al. Folate in gastrointestinal health and disease. Eur Rev Med Pharmacol Sci. 2012 Mar;16(3):376-85.
16
29. Yakut M, Ustun Y, Kabacam G, Soykan I. Serum vitamin B12 and folate status in patients with inflammatory bowel diseases. Eur J Intern Med. 2010 Aug;21(4):320-3.
30. Aarts EO, Janssen IM, Berends FJ. The gastric sleeve: losing weight as fast as micronutrients? Obes
Surg. 2011 Feb;21(2):207-11.
31. Vanderbrink BA, Cain MP, King S, Meldrum K, Kaefer M, Misseri R, et al. Is oral vitamin B(12) therapy effective for vitamin B(12) deficiency in patients with prior ileocystoplasty? J Urol. 2010
Oct;184(4 Suppl):1781-5.
32. Kapadia CR. Vitamin B12 in health and disease: part I--inherited disorders of function, absorption, and transport. Gastroenterologist. 1995 Dec;3(4):329-44.
33. Hershko C, Ronson A, Souroujon M, Maschler I, Heyd J, Patz J. Variable hematologic presentation of autoimmune gastritis: age-related progression from iron deficiency to cobalamin depletion. Blood. 2006
Feb 15;107(4):1673-9.
34. Lahner E, Annibale B. Pernicious anemia: new insights from a gastroenterological point of view. World J
Gastroenterol. 2009 Nov 7;15(41):5121-8.
35. Allen RH, Stabler SP, Savage DG, Lindenbaum J. Metabolic abnormalities in cobalamin (vitamin B12) and folate deficiency. Faseb J. 1993 Nov;7(14):1344-53.
36. Lindenbaum J, Healton EB, Savage DG, Brust JC, Garrett TJ, Podell ER, et al. Neuropsychiatric disorders caused by cobalamin deficiency in the absence of anemia or macrocytosis. The New England journal of medicine. 1988 Jun 30;318(26):1720-8.
37. Nygard O, Nordrehaug JE, Refsum H, Ueland PM, Farstad M, Vollset SE. Plasma homocysteine levels and mortality in patients with coronary artery disease. The New England journal of medicine. 1997 Jul
24;337(4):230-6.
38. Carmel R, Green R, Rosenblatt DS, Watkins D. Update on cobalamin, folate, and homocysteine.
Hematology / the Education Program of the American Society of Hematology American Society of
Hematology Education Program. 2003:62-81.
39. Herzlich B, Herbert V. Depletion of serum holotranscobalamin II. An early sign of negative vitamin B12 balance. Lab Invest. 1988 Mar;58(3):332-7.
40. Herrmann W, Obeid R, Schorr H, Geisel J. Functional vitamin B12 deficiency and determination of holotranscobalamin in populations at risk. Clin Chem Lab Med. 2003 Nov;41(11):1478-88.
41. Morkbak AL, Poulsen SS, Nexo E. Haptocorrin in humans. Clin Chem Lab Med. 2007;45(12):1751-9.
42. Carmel R. Mild transcobalamin I (haptocorrin) deficiency and low serum cobalamin concentrations. Clin
Chem. [Research Support, U.S. Gov't, P.H.S.]. 2003 Aug;49(8):1367-74.
43. Ulleland M, Eilertsen I, Quadros EV, Rothenberg SP, Fedosov SN, Sundrehagen E, et al. Direct assay for cobalamin bound to transcobalamin (holo-transcobalamin) in serum. Clin Chem. 2002 Mar;48(3):526-32.
44. Green R. Metabolite assays in cobalamin and folate deficiency. Bailliere's clinical haematology. 1995
Sep;8(3):533-66.
45. Axis-Shield. Active-B12 the next level of vitamin B12 testing. 2012; Available from: http://www.activeb12.com/Assays-Active-B12 .
46. Kara N, Senes M, Coskun O, Inan L, Saydam G, Yucel D. Urinary methylmalonic acid levels in patients with acute ischemic stroke. Clin Biochem. 2009 May;42(7-8):578-83.
47. Miller JW, Garrod MG, Rockwood AL, Kushnir MM, Allen LH, Haan MN, et al. Measurement of total vitamin B12 and holotranscobalamin, singly and in combination, in screening for metabolic vitamin B12 deficiency. Clin Chem. 2006 Feb;52(2):278-85.
48. Lindenbaum J, Savage DG, Stabler SP, Allen RH. Diagnosis of cobalamin deficiency: II. Relative sensitivities of serum cobalamin, methylmalonic acid, and total homocysteine concentrations. American journal of hematology. 1990 Jun;34(2):99-107.
49. Vorvick LaM, J. Vitamin B12 levels-Results. 2010; Available from: http://www.umm.edu/ency/article/003705res.htm
.
50. Ubbink J. What is a desirable homocysteine level? . In: Carmel R JD, editor. Homocysteine in health and disease. Cambridge, UK: Cambridge University Press; 2001. p. 485-90.
51. Selhub J. Homocysteine metabolism. Annu Rev Nutr. 1999;19:217-46.
52. Bradford GS, Taylor CT. Omeprazole and vitamin B12 deficiency. The Annals of pharmacotherapy.
1999 May;33(5):641-3.
53. Mirkazemi C, Peterson GM, Tenni PC, Jackson SL. Vitamin B12 deficiency in Australian residential aged care facilities. J Nutr Health Aging. 2012 Mar;16(3):277-80.
54. Flood VM, Smith WT, Webb KL, Rochtchina E, Anderson VE, Mitchell P. Prevalence of low serum folate and vitamin B12 in an older Australian population. Aust N Z J Public Health. 2006 Feb;30(1):38-
41.
55. Richardson WS, Wilson MC, Nishikawa J, Hayward RS. The well-built clinical question: a key to evidence-based decisions. ACP J Club. 1995 Nov-Dec;123(3):A12-3.
17
56. Merlin T, Weston A, Tooher R. Extending an evidence hierarchy to include topics other than treatment: revising the Australian 'levels of evidence'. BMC Med Res Methodol. 2009;9:34.
57. NHMRC. NHMRC levels of evidence and grades for recommendations for developers of guidelines.
[Internet]. Canberra, ACT: National Health and Medical Research Council; 2009. Available from: http://www.nhmrc.gov.au/_files_nhmrc/file/guidelines/evidence_statement_form.pdf
.
18
APPENDIX A – MBS DATA
The MBS item numbers relevant to vitamin B12 testing
Table A.1 shows the two MBS item number for vitamin B12 testing. Both of the items are subject to Rule 21 (i.e. no more than three of any combination of these tests are eligible for
Medicare subsidy per patient per year).
Table A.1: Description of vitamin B12 testing funded under the MBS
Item Number
66599
66602
MBS Item Number description
Serum B12 or red cell folate and, if required, serum folate
Schedule Fee: $23.75 Benefit: 75% = $17.85 85% = $20.20
Serum B12 and red cell folate and, if required, serum folate
Schedule Fee: $43.25 Benefit: 75%=$32.45 85%=$36.80
Both of the items are subject to Rule 21: No more than three of any combination of these tests are eligible for
Medicare subsidy per patient per year.
Source: Department of Human Services
Year of adoption in health system
Table A.2 shows when the in-scope MBS item numbers were included on the MBS.
Table A.2: Item, description and schedule fee start dates for MBS item numbers
MBS Item number
66599
Type of date
Item Start Date
Description Start Date
Date
01-Nov-1998
01-Mar-1999
66602 Item Start Date
Description Start Date
Source: Department of Human Services
01 Nov 1998
01 Mar 1999
MBS utilisation and expenditure
Utilisation of both in-scope MBS item numbers for vitamin B12 testing has increased substantially with services for item 66599 increasing by 106% and item 66602 increasing by
746% from 2000/01 to 2011/12 (Table A.3). In the financial year 2011/12, more than 2.3 million services were claimed for these two items.
Table A.3: Number of claims for vitamin B12 testing MBS items since 2000/2001
Financial year
MBS item no
08/09 09/10 10/11 11/12 12/13
66599
66602
382,241
1,476,465
Total 1,858,706
Source: Department of Human Services
399,282
1,586,968
1,986,250
447,211
1,667,155
2,114,366
520,688
1,821,490
2,342,178
The pattern of use for item numbers 66599 and 66602 is further analysed in Figures A.1 and
A.2 showing different patterns of usage by age, gender and time period. This analysis shows that vitamin B12 testing claimed under MBS item numbers 66599 and 66602 is performed for both males and females and across all age groups. However, the number of claims for both items is approximately double for females than for males. Figure A.1 and Figure A.2 both show an increase from 2008 to 2012, almost doubling (green line) compared to 2004-2008
(red line) and 2000 to 2004 (blue line) .
19
Figure A.1: Usage of MBS item 66599 by age and gender since 2000
Figure A.2: Usage of MBS item 66602 by age and gender since 2000
Figure A.3 shows the benefits paid for vitamin B12 testing MBS item numbers 66599 and
66602. The data show that there has been a significant increase in the benefits paid for both item numbers consistent with the increase in the volume of claims. Overall the total of benefits paid in 2011/12 for both items was $77.9m.
Figure A.3: Benefits paid for MBS item numbers 66599 and 66602 since 2000/01
80 000 000
70 000 000
60 000 000
50 000 000
40 000 000
30 000 000
20 000 000
10 000 000
0
00/01 01/02 02/03 03/04 04/05 05/06 06/07 07/08 08/09 09/10 10/11 11/12
66599 66602
Source: Department of Human Services Medicare
20
APPENDIX B - SEARCH TERM STRATEGY
Clinical questions
1.
What is the safety and effectiveness of vitamin B12 testing in patients undergoing the procedure for functional conditions?
Table B.1: Search term strategy for clinical question one
Population
1.
General healthy population
Search Terms
Embase and Medline
Population – ((‘pregnancy’/exp OR ‘pregnancy’) OR (‘infant’/exp OR
‘infant’) OR (‘human milk’/exp OR ‘human milk’) OR (‘lactation’/exp
OR ‘lactation’) OR (‘vegetarian’/exp OR ‘vegetarian’) OR
(‘malnutrition’/exp OR ‘malnutrition’) OR (‘elderly’/exp OR ‘elderly’)
OR (‘aged’/exp OR ‘aged’) OR (‘gluten free diet’/exp OR ‘gluten free diet’) OR (‘alcoholism’/exp OR ‘alcoholism’))
AND
Intervention – (Vit*B12 OR ‘vitamin B12’/exp OR’ vitamin B12’ OR cobalamin OR cyanocobalamin OR hydroxycobalamin OR methylcobalamin OR ‘methymalonic acid /exp OR ‘methylmalonic acid’/exp OR ‘methylmalonic acid’ OR ‘MMA OR ‘methylmalonate’ OR
‘malonic acid’ OR ‘holotranscobalamin’/exp OR ‘holotranscobalamin’
OR ‘holoTC’/exp OR ‘holoTC’ OR ‘folate’/exp OR ‘folate’ OR ‘folic acid’/exp OR ‘folic acid’ OR ‘vitamin B9’/exp OR ‘vitamin B9’ OR
‘tetrahydrofolic acid’ OR ‘methylenetetrahydrofolic acid’ OR ‘serum folate’/exp OR ‘serum folate’ OR’ red cell folate’/exp OR ‘red cell folate’
OR ‘erythrocyte folate’/exp OR ‘erythrocyte folate’ OR
‘homocysteine’/exp OR ‘homocysteine’ OR ‘Hcy’) AND (‘testing’/exp
OR ‘testing’ OR ‘haematologic test*’/exp OR ‘haematologic test*’)
AND
Limits – [humans]/lim AND [english]/lim
Cochrane
Population – ((MeSH descriptor Pregnancy explode all trees) OR (MeSH descriptor Infant explode all trees) OR (MeSH descriptor Human Milk explode all trees) OR (MeSH descriptor Lactation explode all trees) OR
(MeSH descriptor vegetarian explode all trees) OR (MeSH descriptor
Malnutrition explode all trees) OR (MeSH descriptor Aged explode all trees) OR (MeSH descriptor Alcoholism explode all trees) OR
((pregnancy) OR (pregnancy):ti,ab,kw) OR ((infant) OR (infant):ti,ab,kw)
OR ((human milk) OR (human milk):ti,ab,kw) OR ((lactation) OR
(lactation):ti,ab,kw) OR ((vegetarian) OR (vegetarian):ti,ab,kw) OR
((malnutrition) OR (malnutrition):ti,ab,kw) OR ((elderly) OR
(eldrely):ti,ab,kw) OR ((aged) OR (aged):ti,ab,kw) OR ((gluten free diet)
OR (gluten free diet):ti,ab,kw) OR ((alcoholism) OR
(alcoholism):ti,ab,kw))
AND
Intervention – ((MeSH descriptor Vitamin B12 explode all trees) OR
(Vitamin B12):ti,ab,kw OR (MeSH descriptor Cobalamin explode all trees) OR (cobalamin):ti,ab,kw OR (MeSH descriptor Cyanocobalamin explode all trees) OR (cyanocobalamin):ti,ab,kw OR (MeSH descriptor
Hydroxycobalamin explode all trees) OR (hydroxycobalamin):ti,ab,kw
21
Population
2.
Patients diagnosed with anaemia
Search Terms
OR (MeSH descriptor Methylcobalamin explode all trees) OR
(methylcobalamin):ti,ab,kw OR (MeSH descriptor Methylmalonic acid explode all trees) OR (methylmalonic acid):ti,ab,kw OR (MeSH descriptor Methymalonate explode all trees) OR
(methylmalonate):ti,ab,kw OR (MeSH descriptor Malonic acid explode all trees) OR (malonic acid):ti,ab,kw OR (MeSH descriptor
Holotranscobalamin explode all trees) OR (holotranscobalamin):ti,ab,kw
OR (MeSH descriptor HoloTC explode all trees) OR (holoTC):ti,ab,kw
OR (MeSH descriptor Folate explode all trees) OR (folate):ti,ab,kw OR
(MeSH descriptor Folic acid explode all trees) OR (folic acid):ti,ab,kw) )
OR (MeSH descriptor Vitamin B9 explode all trees) OR (vitamin
B9):ti,ab,kw OR (MeSH descriptor Tetrahydrofolic acid explode all trees)
OR (tetrahydrofolic acid):ti,ab,kw) ) OR (MeSH descriptor
Methylenetetrahydrofolic acid explode all trees) OR
(methylenetetrahydrofolic acid):ti,ab,kw OR (MeSH descriptor Serum folate explode all trees) OR (serum folate):ti,ab,kw) ) OR (MeSH descriptor Red cell folate explode all trees) OR (red cell folate):ti,ab,kw
OR (MeSH descriptor Erythrocyte folate explode all trees) OR
(erythrocyte folate):ti,ab,kw) ) OR (MeSH descriptor Homocysteine explode all trees) OR (homocysteine):ti,ab,kw ) AND ((MeSH descriptor
Testing explode all trees) OR (Testing):ti,ab,kw OR (MeSH descriptor
Haematologic test* explode al trees) OR (Haematologic test*):ti,ab,kw)
AND
Limits [humans]/lim AND [english]/lim
Embase and Medline
Population – ((‘anaemia’/exp OR ‘anaemia’ OR ‘anemia’/exp OR
‘anemia’) OR (‘macrocyt*’/exp OR ‘macrocyt*)’ OR (‘megaloblastic
’/exp OR ‘megaloblastic’) OR (‘pernicious’/exp OR ‘pernicious’) OR
(‘pancytopenia’/exp OR ‘pancytopenia’)) AND NOT (‘iron deficiency anaemia’/exp OR ‘iron deficiency anaemia’)
AND
Intervention – (Vit*B12 OR ‘vitamin B12’/exp OR’ vitamin B12’ OR cobalamin OR cyanocobalamin OR hydroxycobalamin OR methylcobalamin OR ‘methymalonic acid /exp OR ‘methylmalonic acid’/exp OR ‘methylmalonic acid’ OR ‘MMA OR ‘methylmalonate’ OR
‘malonic acid’ OR ‘holotranscobalamin’/exp OR ‘holotranscobalamin’
OR ‘holoTC’/exp OR ‘holoTC’ OR ‘folate’/exp OR ‘folate’ OR ‘folic acid’/exp OR ‘folic acid’ OR ‘vitamin B9’/exp OR ‘vitamin B9’ OR
‘tetrahydrofolic acid’ OR ‘methylenetetrahydrofolic acid’ OR ‘serum folate’/exp OR ‘serum folate’ OR’ red cell folate’/exp OR ‘red cell folate’
OR ‘erythrocyte folate’/exp OR ‘erythrocyte folate’ OR
‘homocysteine’/exp OR ‘homocysteine’ OR ‘Hcy’) AND (‘testing’/exp
OR ‘testing’ OR ‘haematologic test*’/exp OR ‘haematologic test*’)
AND
Limits – [humans]/lim AND [english]/lim
Cochrane
Population – ((MeSH descriptor Anaemia explode all trees) OR (MeSH descriptor Megaloblastic explode all trees) OR (MeSH descriptor
Pernicious explode all trees) OR (MeSH descriptor Pancytopenia explode all trees) OR ((anaemia) OR (anaemia):ti,ab,kw) OR ((megaloblastic) OR
(megaloblastic):ti,ab,kw) OR (macrocyt*) OR ((pernicious) OR
(pernicious):ti,ab,kw) OR ((pancytopenia) OR (pancytopenia):ti,ab,kw) )
22
Population
3.
Patients with neurologic disease
Search Terms
AND NOT ((MeSH descriptor Iron deficiency anaemia) OR (iron deficiency anaemia):ti,ab,kw)
AND
Intervention – ((MeSH descriptor Vitamin B12 explode all trees) OR
(Vitamin B12):ti,ab,kw OR (MeSH descriptor Cobalamin explode all trees) OR (cobalamin):ti,ab,kw OR (MeSH descriptor Cyanocobalamin explode all trees) OR (cyanocobalamin):ti,ab,kw OR (MeSH descriptor
Hydroxycobalamin explode all trees) OR (hydroxycobalamin):ti,ab,kw
OR (MeSH descriptor Methylcobalamin explode all trees) OR
(methylcobalamin):ti,ab,kw OR (MeSH descriptor Methylmalonic acid explode all trees) OR (methylmalonic acid):ti,ab,kw OR (MeSH descriptor Methymalonate explode all trees) OR
(methylmalonate):ti,ab,kw OR (MeSH descriptor Malonic acid explode all trees) OR (malonic acid):ti,ab,kw OR (MeSH descriptor
Holotranscobalamin explode all trees) OR (holotranscobalamin):ti,ab,kw
OR (MeSH descriptor HoloTC explode all trees) OR (holoTC):ti,ab,kw
OR (MeSH descriptor Folate explode all trees) OR (folate):ti,ab,kw OR
(MeSH descriptor Folic acid explode all trees) OR (folic acid):ti,ab,kw) )
OR (MeSH descriptor Vitamin B9 explode all trees) OR (vitamin
B9):ti,ab,kw OR (MeSH descriptor Tetrahydrofolic acid explode all trees)
OR (tetrahydrofolic acid):ti,ab,kw) ) OR (MeSH descriptor
Methylenetetrahydrofolic acid explode all trees) OR
(methylenetetrahydrofolic acid):ti,ab,kw OR (MeSH descriptor Serum folate explode all trees) OR (serum folate):ti,ab,kw) ) OR (MeSH descriptor Red cell folate explode all trees) OR (red cell folate):ti,ab,kw
OR (MeSH descriptor Erythrocyte folate explode all trees) OR
(erythrocyte folate):ti,ab,kw) ) OR (MeSH descriptor Homocysteine explode all trees) OR (homocysteine):ti,ab,kw ) AND ((MeSH descriptor
Testing explode all trees) OR (Testing):ti,ab,kw OR (MeSH descriptor
Haematologic test* explode al trees) OR (Haematologic test*):ti,ab,kw)
AND
Limits [humans]/lim AND [english]/lim
Embase and Medline
Population – ((‘paresthesias’/exp OR ‘paresthesias’) OR (‘peripheral neuropathy’/exp OR ‘peripheral neuropathy’) OR (‘combined system disease’/exp OR ‘combined systems disease’))
AND
Intervention – (Vit*B12 OR ‘vitamin B12’/exp OR’ vitamin B12’ OR cobalamin OR cyanocobalamin OR hydroxycobalamin OR methylcobalamin OR ‘methymalonic acid /exp OR ‘methylmalonic acid’/exp OR ‘methylmalonic acid’ OR ‘MMA OR ‘methylmalonate’ OR
‘malonic acid’ OR ‘holotranscobalamin’/exp OR ‘holotranscobalamin’
OR ‘holoTC’/exp OR ‘holoTC’ OR ‘folate’/exp OR ‘folate’ OR ‘folic acid’/exp OR ‘folic acid’ OR ‘vitamin B9’/exp OR ‘vitamin B9’ OR
‘tetrahydrofolic acid’ OR ‘methylenetetrahydrofolic acid’ OR ‘serum folate’/exp OR ‘serum folate’ OR’ red cell folate’/exp OR ‘red cell folate’
OR ‘erythrocyte folate’/exp OR ‘erythrocyte folate’ OR
‘homocysteine’/exp OR ‘homocysteine’ OR ‘Hcy’) AND (‘testing’/exp
OR ‘testing’ OR ‘haematologic test*’/exp OR ‘haematologic test*’)
AND
Limits – [humans]/lim AND [english]/lim
23
Population
4.
Patients with gastrointestinal and malabsoption diseases
Search Terms
Cochrane
Population – ((MeSH descriptor Paresthesias explode all trees) OR
(MeSH descriptor Peripheral Neuropathy explode all trees) OR (MeSH descriptor Combined Systems Disease explode all trees) OR
((paresthesias) OR (paresthesias):ti,ab,kw) OR ((peripheral neuropathy)
OR (peripheral neuropathy):ti,ab,kw) OR ((combined systems disease)
OR (combined systems disease):ti,ab,kw))
AND
Intervention – ((MeSH descriptor Vitamin B12 explode all trees) OR
(Vitamin B12):ti,ab,kw OR (MeSH descriptor Cobalamin explode all trees) OR (cobalamin):ti,ab,kw OR (MeSH descriptor Cyanocobalamin explode all trees) OR (cyanocobalamin):ti,ab,kw OR (MeSH descriptor
Hydroxycobalamin explode all trees) OR (hydroxycobalamin):ti,ab,kw
OR (MeSH descriptor Methylcobalamin explode all trees) OR
(methylcobalamin):ti,ab,kw OR (MeSH descriptor Methylmalonic acid explode all trees) OR (methylmalonic acid):ti,ab,kw OR (MeSH descriptor Methymalonate explode all trees) OR
(methylmalonate):ti,ab,kw OR (MeSH descriptor Malonic acid explode all trees) OR (malonic acid):ti,ab,kw OR (MeSH descriptor
Holotranscobalamin explode all trees) OR (holotranscobalamin):ti,ab,kw
OR (MeSH descriptor HoloTC explode all trees) OR (holoTC):ti,ab,kw
OR (MeSH descriptor Folate explode all trees) OR (folate):ti,ab,kw OR
(MeSH descriptor Folic acid explode all trees) OR (folic acid):ti,ab,kw) )
OR (MeSH descriptor Vitamin B9 explode all trees) OR (vitamin
B9):ti,ab,kw OR (MeSH descriptor Tetrahydrofolic acid explode all trees)
OR (tetrahydrofolic acid):ti,ab,kw) ) OR (MeSH descriptor
Methylenetetrahydrofolic acid explode all trees) OR
(methylenetetrahydrofolic acid):ti,ab,kw OR (MeSH descriptor Serum folate explode all trees) OR (serum folate):ti,ab,kw) ) OR (MeSH descriptor Red cell folate explode all trees) OR (red cell folate):ti,ab,kw
OR (MeSH descriptor Erythrocyte folate explode all trees) OR
(erythrocyte folate):ti,ab,kw) ) OR (MeSH descriptor Homocysteine explode all trees) OR (homocysteine):ti,ab,kw ) AND ((MeSH descriptor
Testing explode all trees) OR (Testing):ti,ab,kw OR (MeSH descriptor
Haematologic test* explode al trees) OR (Haematologic test*):ti,ab,kw)
AND
Limits [humans]/lim AND [english]/lim
Embase and Medline
Population – ((‘atrophic body gastritis’/exp OR ‘atrophic body gastritis’)
OR (‘gastrectomy’/exp OR ‘gastrectomy’) OR (‘gastric sleeve’/exp OR
‘gastric sleeve’) OR (‘peptic ulcer’/exp OR ‘peptic ulcer’) OR (‘
H.
Pylori
’/exp OR ‘
H. Pylori
’) OR (‘dyspepsia’/exp OR ‘dyspepsia’) OR
(‘diarrhoea’/exp OR ‘diarrhoea’) OR (‘coeliac disease’/exp OR ‘coeliac disease’) OR (‘Crohn’s disease’/exp OR ‘Crohn’s disease’) OR
(‘tapeworms’/exp OR ‘tapeworms’))
AND
Intervention – (Vit*B12 OR ‘vitamin B12’/exp OR’ vitamin B12’ OR cobalamin OR cyanocobalamin OR hydroxycobalamin OR methylcobalamin OR ‘methymalonic acid /exp OR ‘methylmalonic acid’/exp OR ‘methylmalonic acid’ OR ‘MMA OR ‘methylmalonate’ OR
‘malonic acid’ OR ‘holotranscobalamin’/exp OR ‘holotranscobalamin’
OR ‘holoTC’/exp OR ‘holoTC’ OR ‘folate’/exp OR ‘folate’ OR ‘folic acid’/exp OR ‘folic acid’ OR ‘vitamin B9’/exp OR ‘vitamin B9’ OR
24
Population Search Terms
‘tetrahydrofolic acid’ OR ‘methylenetetrahydrofolic acid’ OR ‘serum folate’/exp OR ‘serum folate’ OR’ red cell folate’/exp OR ‘red cell folate’
OR ‘erythrocyte folate’/exp OR ‘erythrocyte folate’ OR
‘homocysteine’/exp OR ‘homocysteine’ OR ‘Hcy’) AND (‘testing’/exp
OR ‘testing’ OR ‘haematologic test*’/exp OR ‘haematologic test*’)
AND
Limits – [humans]/lim AND [english]/lim
Cochrane
Population – ((MeSH descriptor Atrophic Body Gastritis explode all trees) OR (MeSH descriptor Gastrectomy explode all trees) OR (MeSH descriptor Gastric Sleeve explode all trees) OR (MeSH descriptor Peptic
Ulcer explode all trees) OR (MeSH descriptor H. pylori explode all trees)
OR (MeSH descriptor Dyspepsia explode all trees) OR (MeSH descriptor
Diarrhoea explode all trees) OR (MeSH descriptor Coeliac Disease explode all trees) OR (MeSH descriptor Crohn’s Disease explode all trees) OR (MeSH descriptor Tapeworms explode all trees) OR ((atrophic body gastritis) OR (atrophic body gastritis):ti,ab,kw OR (gastrectomy)
OR (gastrectomy):ti,ab,kw OR (gastric sleeve) OR (gastric sleeve):ti,ab,kw OR (peptic ulcer) OR (peptic ulcer):ti,ab,kw OR ( h. pylori ) OR ( h. pylori ):ti,ab,kw OR (dyspepsia) OR (dyspepsia):ti,ab,kw
OR (diarrhoea) OR (diarrhoea):ti,ab,kw OR (coeliac disease) OR (coeliac disease):ti,ab,kw OR (Crohn’s disease) OR (Crohn’s disease):ti,ab,kw OR
(tapeworms) OR (tapeworms):ti,ab,kw )
AND
Intervention – ((MeSH descriptor Vitamin B12 explode all trees) OR
(Vitamin B12):ti,ab,kw OR (MeSH descriptor Cobalamin explode all trees) OR (cobalamin):ti,ab,kw OR (MeSH descriptor Cyanocobalamin explode all trees) OR (cyanocobalamin):ti,ab,kw OR (MeSH descriptor
Hydroxycobalamin explode all trees) OR (hydroxycobalamin):ti,ab,kw
OR (MeSH descriptor Methylcobalamin explode all trees) OR
(methylcobalamin):ti,ab,kw OR (MeSH descriptor Methylmalonic acid explode all trees) OR (methylmalonic acid):ti,ab,kw OR (MeSH descriptor Methymalonate explode all trees) OR
(methylmalonate):ti,ab,kw OR (MeSH descriptor Malonic acid explode all trees) OR (malonic acid):ti,ab,kw OR (MeSH descriptor
Holotranscobalamin explode all trees) OR (holotranscobalamin):ti,ab,kw
OR (MeSH descriptor HoloTC explode all trees) OR (holoTC):ti,ab,kw
OR (MeSH descriptor Folate explode all trees) OR (folate):ti,ab,kw OR
(MeSH descriptor Folic acid explode all trees) OR (folic acid):ti,ab,kw) )
OR (MeSH descriptor Vitamin B9 explode all trees) OR (vitamin
B9):ti,ab,kw OR (MeSH descriptor Tetrahydrofolic acid explode all trees)
OR (tetrahydrofolic acid):ti,ab,kw) ) OR (MeSH descriptor
Methylenetetrahydrofolic acid explode all trees) OR
(methylenetetrahydrofolic acid):ti,ab,kw OR (MeSH descriptor Serum folate explode all trees) OR (serum folate):ti,ab,kw) ) OR (MeSH descriptor Red cell folate explode all trees) OR (red cell folate):ti,ab,kw
OR (MeSH descriptor Erythrocyte folate explode all trees) OR
(erythrocyte folate):ti,ab,kw) ) OR (MeSH descriptor Homocysteine explode all trees) OR (homocysteine):ti,ab,kw ) AND ((MeSH descriptor
Testing explode all trees) OR (Testing):ti,ab,kw OR (MeSH descriptor
Haematologic test* explode al trees) OR (Haematologic test*):ti,ab,kw)
AND
25
Population
5.
Patients with psychiatric disorders
Search Terms
Limits [humans]/lim AND [english]/lim
Embase and Medline
Population – ((‘dementia’/exp OR ‘dementia’) OR (‘depression’/exp OR
‘depression’) OR (‘psychosis’/exp OR ‘psychosis’) OR (‘Alzheimer’s disease’/exp OR ‘Alzheimer’s disease’))
AND
Intervention – (Vit*B12 OR ‘vitamin B12’/exp OR’ vitamin B12’ OR cobalamin OR cyanocobalamin OR hydroxycobalamin OR methylcobalamin OR ‘methymalonic acid /exp OR ‘methylmalonic acid’/exp OR ‘methylmalonic acid’ OR ‘MMA OR ‘methylmalonate’ OR
‘malonic acid’ OR ‘holotranscobalamin’/exp OR ‘holotranscobalamin’
OR ‘holoTC’/exp OR ‘holoTC’ OR ‘folate’/exp OR ‘folate’ OR ‘folic acid’/exp OR ‘folic acid’ OR ‘vitamin B9’/exp OR ‘vitamin B9’ OR
‘tetrahydrofolic acid’ OR ‘methylenetetrahydrofolic acid’ OR ‘serum folate’/exp OR ‘serum folate’ OR’ red cell folate’/exp OR ‘red cell folate’
OR ‘erythrocyte folate’/exp OR ‘erythrocyte folate’ OR
‘homocysteine’/exp OR ‘homocysteine’ OR ‘Hcy’) AND (‘testing’/exp
OR ‘testing’ OR ‘haematologic test*’/exp OR ‘haematologic test*’)
AND
Limits – [humans]/lim AND [english]/lim
Cochrane
Population – ((MeSH descriptor Dementia explode all trees) OR (MeSH descriptor Depression explode all trees) OR (MeSH descriptor Psychosis explode all trees) OR (MeSH descriptor Alzheimer’s disease explode all trees) OR((dementia) OR (dementia):ti,ab,kw) OR ((depression) OR
(depression):ti,ab,kw) OR ((psychosis) OR (psychosis):ti,ab,kw) OR
((Alzheimer’s disease) OR (Alzheimer’s disease):ti,ab,kw))
AND
Intervention – ((MeSH descriptor Vitamin B12 explode all trees) OR
(Vitamin B12):ti,ab,kw OR (MeSH descriptor Cobalamin explode all trees) OR (cobalamin):ti,ab,kw OR (MeSH descriptor Cyanocobalamin explode all trees) OR (cyanocobalamin):ti,ab,kw OR (MeSH descriptor
Hydroxycobalamin explode all trees) OR (hydroxycobalamin):ti,ab,kw
OR (MeSH descriptor Methylcobalamin explode all trees) OR
(methylcobalamin):ti,ab,kw OR (MeSH descriptor Methylmalonic acid explode all trees) OR (methylmalonic acid):ti,ab,kw OR (MeSH descriptor Methymalonate explode all trees) OR
(methylmalonate):ti,ab,kw OR (MeSH descriptor Malonic acid explode all trees) OR (malonic acid):ti,ab,kw OR (MeSH descriptor
Holotranscobalamin explode all trees) OR (holotranscobalamin):ti,ab,kw
OR (MeSH descriptor HoloTC explode all trees) OR (holoTC):ti,ab,kw
OR (MeSH descriptor Folate explode all trees) OR (folate):ti,ab,kw OR
(MeSH descriptor Folic acid explode all trees) OR (folic acid):ti,ab,kw) )
OR (MeSH descriptor Vitamin B9 explode all trees) OR (vitamin
B9):ti,ab,kw OR (MeSH descriptor Tetrahydrofolic acid explode all trees)
OR (tetrahydrofolic acid):ti,ab,kw) ) OR (MeSH descriptor
Methylenetetrahydrofolic acid explode all trees) OR
(methylenetetrahydrofolic acid):ti,ab,kw OR (MeSH descriptor Serum folate explode all trees) OR (serum folate):ti,ab,kw) ) OR (MeSH descriptor Red cell folate explode all trees) OR (red cell folate):ti,ab,kw
OR (MeSH descriptor Erythrocyte folate explode all trees) OR
(erythrocyte folate):ti,ab,kw) ) OR (MeSH descriptor Homocysteine
26
Population Search Terms explode all trees) OR (homocysteine):ti,ab,kw ) AND ((MeSH descriptor
Testing explode all trees) OR (Testing):ti,ab,kw OR (MeSH descriptor
Haematologic test* explode al trees) OR (Haematologic test*):ti,ab,kw)
AND
Limits [humans]/lim AND [english]/lim
2.
What is the evidence regarding the cost implications associated with vitamin B12 testing?
Table B.2: Search term strategy for clinical question two
Population
1.
Patients undertaking serum vitamin
B12/folate testing
Search Terms
Embase and Medline
Intervention – (Vit*B12 OR ‘vitamin B12’/exp OR’ vitamin B12’
OR cobalamin OR cyanocobalamin OR hydroxycobalamin OR methylcobalamin OR ‘methymalonic acid /exp OR ‘methylmalonic acid’/exp OR ‘methylmalonic acid’ OR ‘MMA OR
‘methylmalonate’ OR ‘malonic acid’ OR ‘holotranscobalamin’/exp
OR ‘holotranscobalamin’ OR ‘holoTC’/exp OR ‘holoTC’ OR
‘folate’/exp OR ‘folate’ OR ‘folic acid’/exp OR ‘folic acid’ OR
‘vitamin B9’/exp OR ‘vitamin B9’ OR ‘tetrahydrofolic acid’ OR
‘methylenetetrahydrofolic acid’ OR ‘serum folate’/exp OR ‘serum folate’ OR’ red cell folate’/exp OR ‘red cell folate’ OR ‘erythrocyte folate’/exp OR ‘erythrocyte folate’ OR ‘homocysteine’/exp OR
‘homocysteine’ OR ‘Hcy’) AND (‘testing’/exp OR ‘testing’ OR
‘haematologic test*’/exp OR ‘haematologic test*’)
AND
Economic Terms – (‘economic aspect’/exp OR ‘cost benefit analysis’ OR cost* OR ‘cost effectiveness’)
AND
Limits – [humans]/lim AND [english]/lim
Cochrane
Intervention – ((MeSH descriptor Vitamin B12 explode all trees)
OR (Vitamin B12):ti,ab,kw OR (MeSH descriptor Cobalamin explode all trees) OR (cobalamin):ti,ab,kw OR (MeSH descriptor
Cyanocobalamin explode all trees) OR (cyanocobalamin):ti,ab,kw
OR (MeSH descriptor Hydroxycobalamin explode all trees) OR
(hydroxycobalamin):ti,ab,kw OR (MeSH descriptor
Methylcobalamin explode all trees) OR (methylcobalamin):ti,ab,kw
OR (MeSH descriptor Methylmalonic acid explode all trees) OR
(methylmalonic acid):ti,ab,kw OR (MeSH descriptor
Methymalonate explode all trees) OR (methylmalonate):ti,ab,kw
OR (MeSH descriptor Malonic acid explode all trees) OR (malonic acid):ti,ab,kw OR (MeSH descriptor Holotranscobalamin explode all trees) OR (holotranscobalamin):ti,ab,kw OR (MeSH descriptor
HoloTC explode all trees) OR (holoTC):ti,ab,kw OR (MeSH descriptor Folate explode all trees) OR (folate):ti,ab,kw OR (MeSH descriptor Folic acid explode all trees) OR (folic acid):ti,ab,kw) )
OR (MeSH descriptor Vitamin B9 explode all trees) OR (vitamin
B9):ti,ab,kw OR (MeSH descriptor Tetrahydrofolic acid explode all trees) OR (tetrahydrofolic acid):ti,ab,kw) ) OR (MeSH descriptor
Methylenetetrahydrofolic acid explode all trees) OR
(methylenetetrahydrofolic acid):ti,ab,kw OR (MeSH descriptor
27
Population Search Terms
Serum folate explode all trees) OR (serum folate):ti,ab,kw) ) OR
(MeSH descriptor Red cell folate explode all trees) OR (red cell folate):ti,ab,kw OR (MeSH descriptor Erythrocyte folate explode all trees) OR (erythrocyte folate):ti,ab,kw) ) OR (MeSH descriptor
Homocysteine explode all trees) OR (homocysteine):ti,ab,kw )
AND ((MeSH descriptor Testing explode all trees) OR
(Testing):ti,ab,kw OR (MeSH descriptor Haematologic test* explode al trees) OR (Haematologic test*):ti,ab,kw)
AND
Economic Terms – (((economic aspect) OR (economic aspect):kw)
OR ((cost benefit) OR (cost benefit):kw)) OR ((cost effectiveness)
OR (cost effectiveness):kw) OR (MeSH descriptor Cost-Benefit
Analysis explode all trees) OR (MeSH descriptor Costs and Cost
Analysis explode all trees))
AND
Limits [humans]/lim AND [english]/lim
28
APPENDIX C – SEARCH STRATEGY
Search strategies generally include a combination of indexing terms (e.g. MeSH or Emtree headings) and text word terms. Tables B.1 and B.2 set out proposed terms to identify papers in EMBASE. These terms would also be adopted to search other databases as described above. Limits will be employed in a hierarchical manner according to the type of literature being sourced (i.e. Limit 1, and if no relevant literature then Limit 2 and if no relevant literature, then Limit 3).
The selection criteria in Table C.1 will be applied to all publications identified by the literature search to identify studies eligible for inclusion in the systematic review. Study eligibility will be assessed by at least two reviewers.
Table C.1: Inclusion/exclusion criteria for identification of relevant studies
Characteristic Criteria
Publication Clinical studies included. Non-systematic reviews, letters, editorials, animal, in vitro type and laboratory studies excluded.
Systematic reviews
Systematic reviews that have been superseded will be excluded
Primary studies
Primary studies published during the search period of included systematic reviews excluded
Effectiveness studies Emphasis will be placed on identifying comparative trials however in the absence of such evidence other study designs may be included such as cohort or case series studies (> 20? Patients)
prospective, comparative trial
>20 patients
Safety studies included if:
>50 patients included
Intervention B12/folate testing
Outcome
Language
No testing
Studies must report on at least one of the following outcomes:
Patient outcomes: (morbidity, mortality, quality of life )
Safety: (adverse physical health outcomes or complications associated with the procedure )
Non-English language articles excluded
All eligible studies will be assessed according to the National Health and Medical Research
Council (NHMRC) Dimensions of Evidence (Table C.2). There are three main domains: strength of the evidence, size of the effect and relevance of the evidence. The first domain is derived directly from the literature identified for a particular intervention. The last two require expert clinical input as part of their determination.
Type of evidence
Strength of the evidence
Level
Quality
Statistical precision
Table C.2: Dimensions of Evidence
Definition
The study design used, as an indicator of the degree to which bias has been eliminated by design.
The methods used by investigators to minimise bias within a study design.
The p-value or, alternatively, the precision of the estimate of the effect (as indicated by the confidence interval). It reflects the degree of certainty about the existence of a true effect.
29
Size of effect The distance of the study estimate from the “null” value and the inclusion of only clinically important effects in the confidence interval.
Relevance of evidence The usefulness of the evidence in clinical practice, particularly the appropriateness of the outcome measures used.
One aspect of the ‘strength of the evidence’ domain is the level of evidence, which will be assigned using the NHMRC levels of evidence outlined in Merlin et al 2009.
Study quality will be evaluated and reported using the NHMRC Quality Criteria (Table B.3) for randomised controlled trials, cohort studies, case control studies and systematic reviews.
Table C.3: Quality criteria for RCTs, cohort studies, case-control studies and systemic reviews
Study type Quality criteria
Randomised controlled trials a Was the study double blinded?
Cohort studies b
Was allocation to treatment groups concealed from those responsible for recruiting the subjects?
Were all randomised participants included in the analysis?
How were subjects selected for the ‘new intervention’?
How were subjects selected for the comparison or control group?
Does the study adequately control for demographic characteristics, clinical features and other potential confounding variables in the design or analysis?
Was the measurement of outcomes unbiased (i.e. blinded to treatment group and comparable across groups)?
Was follow-up long enough for outcomes to occur?
Was follow-up complete and were there exclusions from the analysis?
Case-control studies b
Systematic reviews c
How were cases defined and selected?
How were controls defined and selected?
Does the study adequately control for demographic characteristics and important potential confounders in the design or analysis?
Was measurement of exposure to the factor of interest (e.g. the new intervention) adequate and kept blinded to case/control status?
Were all selected subjects included in the analysis?
Was an adequate search strategy used?
Were the inclusion criteria appropriate and applied in an unbiased way?
Was a quality assessment of included studies undertaken?
Were the characteristics and results of the individual studies appropriately summarised?
Were the methods for pooling the data appropriate?
Were sources of heterogeneity explored?
Source: National Health and Medical Research Council (NHMRC), 2000. How to review the evidence: systematic identification and review of the scientific literature, NHMRC, Commonwealth of Australia, Canberra. a
Based on work of Schulz et al (1995) and Jadad et al
(1996) b
Based on quality assessment instruments developed and being tested in Australia and Canada c
Based on articles by Greenhalgh
(1997) and Hunt and McKibbon (1997)
Data will be extracted from individual studies using a standardised data extraction form designed specifically for this review. Data extraction will be performed by one reviewer and checked by a second reviewer.
30