HEALTH HISTORY
advertisement

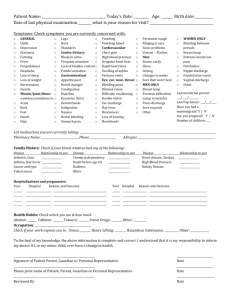
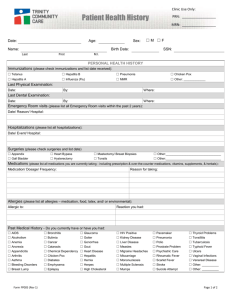
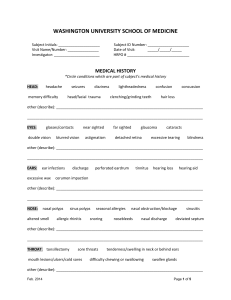
HEALTH HISTORY Today’s date Name Birthdate Reason for visit: SYMPTOMS: (Circle symptoms related to today’s visit or, if here for a physical exam, check those you’ve had in past year) GENERAL: Fever Chills Sweats Fatigue Sleep Problems Weight Gain Weight Loss Depression Anxiety EYES: Blurred vision Double vision Loss of vision Eye pain Eye Discharge Itchy Eyes EARS/NOSE/THROAT: Earaches Ear Discharge Ringing in ears Sore throat Wear Glasses? Contacts? Hearing loss Congestion Nosebleeds Sinus pain/congestion Difficulty Swallowing Hoarseness Dental problems Bleeding Gums LUNGS/HEART: Cough Coughing up blood Chest pain Shortness of breath Wheezing Irregular heart beat GASTROINTESTINAL: Poor appetite Bloating Abdominal Pain Nausea/vomiting Diarrhea Constipation Indigestion Hemorrhoids Rectal pain/itching/bleeding Have you had a colonoscopy? (year) URINARY: Painful urination Frequency Urgency Blood in urine Incontinence (or lack of control) Recurring infections MUSCULOSKELETAL: Painful joints Joint swelling Weakness Neck Pain Back Pain NEUROLOGICAL: Headaches Dizziness/Vertigo Fainting spells Numbness Tingling Tremor SKIN: Rash Itchiness Sores that will not heal Bruises Hives Change in moles MEN ONLY: Breast lump Testicular lump Erection difficulties WOMEN ONLY: Breast lump Breast pain Nipple discharge Irregular periods Painful periods Hot Flashes Night Sweats Vaginal discharge Pain with intercourse Birth Control Method: Pill Ring Patch Condom Vasectomy Tubal IUD Other: First day of last period: Are you pregnant or planning to get pregnant in next 3 months: Last pap smear: Last mammogram: Last bone density: ALLERGIES: (Substance or medicine, Reaction) MEDICATIONS/SUPPLEMENTS: (Name of medication, dose and how taken) LYNN ALBERTSON ARNP, PS 13110 NE 177 PL STE B102 WOODINVILLE WA 98072 (425)415-8300 HEALTH HISTORY (continued) HEALTH CONDITIONS: Diagnosis: Health Care Provider: SURGERIES OR HOSPITALIZATIONS: (Procedure or reason, Approximate date/year) PREGNANCY HISTORY: Total pregnancies Deliveries Tubal Miscarriages Terminations Children’s names and ages: HEALTH HABITS: Exercise: Type and times per week: Diet: General description Tobacco: Never Former (packs/cans per day x # years Current: (# packs/cans per day x # years ) ) When did you quit? Do you want to quit? YES Alcohol: (type and amount per day or week or year) Other Substances Used: (type) Do you want to quit (alcohol/other drugs)? FAMILY HEALTH HISTORY: Relation: Age (if alive): Age of death: Health Conditions (or cause of death): Father: Mother: Brothers: Sisters: Paternal Grandfather: Grandmother: Maternal Grandfather: Grandmother: REVIEWED BY: LYNN ALBERTSON ARNP DATE: NO