Morbidity and Mortality Review Form
Conference Date:
Patient Initials:
MRN:
Patient Demographics
Admit Date:
Discharge Date:
Business Unit:
UH UHE James PCN Ross Other:_____________
Resident Staff at Time of Event (list all):
Admitting Diagnosis:
Date of Event:
Attending Physician at Time of
Event:
Unit at Time of Event:
Service at Time of
Event:
Physician at Time Event if not the Attending (list all):
Brief Case Summary:
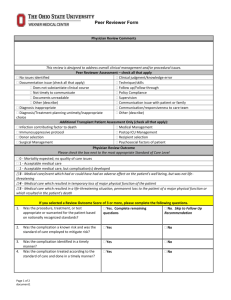
This review is designed to address overall clinical management and/or procedural issues.
Case Assessment (All Patients) – check all that apply
No issues identified
Clinical judgment/knowledge error
Documentation issue (check all that apply)
Technique/skills
Does not substantiate clinical course
Follow up/Follow through
Not timely to communicate
Policy Compliance
Documents unreadable
Other (describe)
Supervision
Diagnosis inappropriate
Communication issue with patient or family
Diagnostic/Treatment planning untimely/inappropriate choice
Workload
Communication/responsiveness to care team (includes handoff)
Other (describe)
Transplant Patient Assessment Only (check all that apply):
Orthopedic Patient Assessment Only (check all that apply)
Return to OR for unplanned procedure within 6
Infection contributing factor to death
weeks of primary procedure
Immunosuppressive protocol
Intraop or postop neurovascular injury or deficit
Donor selection
Intraop or postop PE, DVT, or thrombophlebitis
Intraop or postop major medical complication
Surgical Management
(cardiopulmonary, neurological, GI, GU, etc)
Medical Management
Technique/skill
Postop ICU Management
Inappropriate implant
Recipient selection
Implant failure
Psychosocial factors of patient
Early loss of bone fixation
Intraop or postop fracture or dislocation
Please briefly describe assessment findings:
Page 1 of 2
This information is confidential per Ohio Revised Code Sec 2305.25 and may not be shared, discussed or distributed outside of the quality process. If the
reader of this communication is not an intended recipient, you are hereby notified that any dissemination, distribution or copying of this communication is
strictly prohibited.
document1
Morbidity and Mortality Review Form
Conference Date:
Assessment of Impact – please check only one
0 - Mortality expected or no quality of care issues
1 - Acceptable medical care
2 - Acceptable medical care, but complication(s) developed
3 - Medical care/event which had or could have had an adverse effect on the patient’s well being, but was not lifethreatening
4 - Medical care which resulted in temporary loss of major physical function of the patient
5 - Medical care which resulted in a life-threatening situation, permanent loss to the patient of a major physical function or
which resulted in the patient’s death
If you selected a Review Outcome Score of 3 or more, please complete the following questions.
1. Was the procedure, treatment, or test appropriate or warranted
Yes. Complete
No. Skip to Follow
for the patient based on nationally recognized standards?
remaining questions
Up Recommendation
2.
Was the complication a known risk and was the standard of care
employed to mitigate risk?
Yes
No
3.
4.
Was the complication identified in a timely manner?
Was the complication treated according to the standard of care
and done in a timely manner?
Yes
Yes
No
No
Case Follow Up Recommendation – check all that apply
No further action necessary
Referral to Medical Director
Education pertinent to findings
Referral to another department (please specify)
Potential peer review issue identified, please forward to
Department Chair and Physicians Executive Council Chair
Other (please specify)
Reviewer Signature:
Division Director or Department Chair Signature:
Date:
Date:
Proposed Solutions for any Identified Opportunity for Improvement
Educational intervention
Personal judgment
Supervision
Workload
Systems
Communication
Other
Page 2 of 2
This information is confidential per Ohio Revised Code Sec 2305.25 and may not be shared, discussed or distributed outside of the quality process. If the
reader of this communication is not an intended recipient, you are hereby notified that any dissemination, distribution or copying of this communication is
strictly prohibited.
document1
 0
0