S2. Independent CFU - Springer Static Content Server
advertisement

Online AAPS Supplement
Stochastic Process Pharmacodynamics
Dose Timing in Neonatal Gentamicin Therapy as an Example
Table of Contents
S1. Preview .................................................................................................................................1
S2. Independent CFU ................................................................................................................1
S2.1 Deterministic and stochastic formalisms. ..................................................................................... 1
S2.2 Lineages ....................................................................................................................................... 2
S2.3 Intuitive remarks about the lineage non-extinction function ε(t). ................................................ 3
S2.4 Tracking the number of CFU per patient ..................................................................................... 4
S3. Details of the calculations: equations used, R scripts, tables of results ..........................5
S3.1 Equations used in paper. .............................................................................................................. 5
S3.2 PKPD.R script .............................................................................................................................. 6
S3.3 Other scripts ................................................................................................................................. 9
S4 A Front Boosting Theorem ................................................................................................10
S4.1 Stochastic process theory in radiation biology and tumor radiotherapy treatment planning. .... 10
S4.2 Notation and assumptions .......................................................................................................... 11
S4.3 Results ........................................................................................................................................ 12
S5. Supplement Bibliography .................................................................................................13
S1. Preview
This supplement contains technical details on calculations for drug dosing regimens designed to eradicate CFU.
Section 2 generalizes to drug treatments some results obtained in radiotherapy treatment planning. Section 2 is
intended mainly for mathematicians; others may find it useful for its intuitive comments. Section 3 contains
details on the computations of the paper, including heavily commented open-source R scripts. Section 4 gives a
table, excerpts from which constitute Tables I and II of the paper. Section 5 derives a mathematical theorem on
stochastic effects favoring front loading. The theorem is applicable to essentially all dosing regimens, but only
under restrictive PD assumptions that exclude its direct application to the gentamicin calculations.
S2. Independent CFU
S2.1 Deterministic and stochastic formalisms.
The standard deterministic model for the growth or decrease of a population of independent CFU is a linear
ordinary differential equation (ODE), Eq. (S2.1.1A), and its solution (S2.1.1B):
(A) dm/dt=( t )m ( B ) m( t ) m( 0 )exp 0 ( )d 0.
t
(S 2.1.1 )
Here and throughout we consider times t ≥0; μ(t) is the Malthusian rate, interpreted as the difference between
per CFU birth and death rates, and can be negative. Stochastic process models are usually preferred to
deterministic ones such as S.2.1.1 in population dynamics studies (Kimmel and Axelrod 2002). The stochastic
process corresponding to Eq. (S2.1.1) is a continuous time birth-death process for CFU that are independent
identically distributed (IID), with per-CFU rates that can be time-dependent but must be state-independent. It is
sometimes called the Feller-Arley-Kendall process (Kendall 1948). In general, the stochastic process that
“corresponds” to a given deterministic population dynamics ODE is not unique and the time course of the
expected value is typically not given by that ODE (Campillo et al. 2013). The correspondence between the
Feller-Arley-Kendall process and its deterministic counterpart is much closer than the ambiguous
correspondences that are needed in analyzing other CFU PD, e.g. sigmoid population dynamics. For example,
for the Feller-Arley-Kendall process the expected value is simply the function m(t) in Eq. (S2.1.1), i.e. just the
average calculated deterministically (Tan 2002).
S2.2 Lineages
For IID CFU it is useful to focus on processes originated by a single cell (“lineages”) so in this subsection we
assume that there is exactly one CFU at t=0 and correspondingly take the initial average number in the
deterministic equation (S.2.1.1) to be m(0)=1. Subsection 2.4 below concerns generalizations to the case of
many CFU at t=0. Assume the Malthusian rate μ(t) is a real-valued piecewise continuous function of the time;
denote the per-CFU birth rate, a continuous non-negative function, by b(t). For the per-CFU death rate
d(t)=b(t)-μ(t), assume d(t)>0 unless explicitly stated to the contrary since we are analyzing treatments designed
to eradicate the CFU.
Tan (Tan 2002) gives analytic solutions of the Feller-Arley-Kendall process in terms of two auxiliary
functions:
é t
ù
( A ) x ( t ) = exp ê- ò m( t )d t ú ; (B) z ( t ) =
ë 0
û
ò
t
0
b( t )x ( t )d t . ( S2.2.1)
We shall also use a third:
( t ) b( y )exp ( )d dy d /dt=b(t)+ ( t ) (t); ( 0 ) 0. ( S 2.2.2 )
t
0
t
y
Tan’s results include the following. First, the expected value of the CFU number is 1/ξ(t). Second, the
probability that there is exactly 1 CFU at time t, P{X(t)=1|X(0)=1} in Tan’s notation, is given by ξ/(ζ+ξ)2.
Third, and most importantly for the paper, Tan derives the probability ε(t)=P{X(t)≠0|X(0)=1} that a CFU
lineage is not yet eradicated (has one or more CFU at time t); using notation ε(t) is our mnemonic device,
chosen because ε(t)≪1 in the situations of main interest here wherein useful treatments are applied between
times 0 and t, and many CFU exist at the time of diagnosis t=0. Tan shows the lineage non-extinction
probability ε(t) is 1/(ζ+ξ). Manipulating the integrals ζ and ξ in the equation ε(t) = 1/(ζ+ξ) with standard onevariable calculus operations, using ξ(t)=1/m(t), and using Eq. (S2.2.2) gives a remarkably interesting “stochastic
corrections” equation for ε(t):
( t )
m(t)
. (S 2.2.3 )
1(t )
We now discuss some intuitive interpretations of this equation and its implications.
S2.3 Intuitive remarks about the lineage non-extinction function ε(t).
1. The paper is concerned mainly with situations where ε(t) is very small, e.g. ε(t)= 0.5x10-9. The reason
for such very small numbers is that combining the deterministic PK estimates of initial blood volume
(Nielsen et al. 2009) with those of initial CFU/mL (Mohamed et al. 2012) indicates that at birth an
infected neonate may harbor, very roughly, a billion bacterial CFU, and we are asking about treatments
that eradicate each one of the resulting lineages.
2. Suppose first, in preparation for interpreting less trivial cases, that b(t)=0 for all t. Then Eqs. (S2.2.2)
and (S2.2.3) show that Φ=0 and thus ε(t)= m(t). The interpretation is the following. In the stochastic
model with b(t)=0, the probability of having a lineage with 2 or more CFU is always zero because no
births ever occur. So the time dependent probability of exactly one cell must be ε(t). On the other hand
the deterministic model Eq. 1 shows that the average CFU number per lineage is m(t). In this special
case the average happens to tell us the whole probability distribution: having the probability for one cell
be m(t) and the probability for zero be 1-m(t) is the only way to get an average of m(t) when the
probability of two or more cells is zero (formally: the expected value of a Bernoulli distribution must
equal the success parameter). Thus we must have ε=m as Eq. (S2.2.3) implies.
The case d(t)=0 is also instructive. Then Eq. (S2.2.2) becomes
( t ) b( y )exp b( )d dy dy
t
t
0
y
t
0
d exp b( )d
t
y
dy
m( t ) 1. ( S 2.2.4 )
Inserting into Eq. (S.2.2.3) gives ε(t)=1, which is clearly correct since with no deaths there can be no
eradication.
3. Now and throughout the rest of this section consider the more realistic case that b(t)>0 and d(t)>0 for all
t. Then for all t>0, Φ(t)>0 by Eq. (S2.2.2) so ε(t) < m(t) by Eq. (S2.2.3), a key inequality replacing the
equality of comment 2 above. This inequality has a useful intuitive interpretation: for b(t)>0, d(t)>0 all
kinds of stochastic fluctuations occur; and such churning is known to favor eradication (Ovaskainen and
Meerson 2010). Specifically, let P(j,t) be the probability that there are j CFU at time t. Then the
equations for the mean m and for the non-extermination probability ε obey the following inequality:
m j 1 jP( j,t ) j 1 P( j,t ) , with the inequality strict unless P( j ) 0 j>1.
(S 2.3.1 )
Therefore ε<m unless all the non-eradicated lineages have P(1,t)=1 and P(j,t)=0 for j≠1, i.e. there can
be no fluctuations among the non-eradicated lineages. However, the explicit solution for P(j,t) (Hanin
2004) shows that, to the contrary, P(j,t)>0 for all j when t>0, implying ε<m.
4. In comment 3 note from Eq. (S2.2.2) that Φ is an increasing function of time so that from the stochastic
corrections equation (S.2.3) ε/m is a decreasing one. In this sense the effects of stochastic fluctuations,
and thus of stochastic corrections to deterministic predictions, grow more important as time increases.
5. Suppose we compare two Feller-Arley-Kendall models with the same Malthusian rate, so their
deterministic description is identical. Suppose the birth rate of the first model is strictly greater than that
of the second model at all times. Then Eq. (S2.2.2) implies Φ(t) is greater for the first model and thus by
the stochastic corrections equation (S2.2.3) ε(t) is smaller. The intuitive reason is that increasing the
birth rate necessarily involves an equal increase in death rate to keep the Malthusian rate the same.
When both birth and death rates increase, the stochastic fluctuations they imply also increase; these extra
fluctuations cause extra eradications (see comment 3 above), so the lineage non-extinction function ε(t)
is smaller [compare (Michor et al. 2005)].
6. Since CFU are considered IID, intuitive comments such as the above, about lineages that start from a
single CFU at time t=0, can be extended to intuitive comments about populations that initially have
more than 1 CFU without much trouble. The next subsection gives examples
S2.4 Tracking the number of CFU per patient
The initial average number of CFU per mL at t=0 is taken to be 4.83x105 CFU/mL in all cases (Mohamed et al.
2012). Thus we took the initial average number of CFU per neonate to be N(0)=4.83x105xVC(0), where VC(0)
is the deterministic PK estimate (Nielsen et al. 2009) of the average initial volume of the central compartment in
mL. The order of magnitude of the result is N(0) ≈109. It is an average, so for a stochastic PD calculation we
must choose some distribution with expected value N(0). All plausible choices have variance that is the same
order of magnitude as N(0) and for the final results all such choices will give the same answers to relevant
accuracy because the standard deviation will then be of order [N(0)]1/2<10-4 N(0); indeed, even the (rather
unreasonable) assumption that all starting values are exactly the same would give the same final results to
within a relative accuracy of 10-4. In such situations it is standard to choose the Poisson distribution, which is
among the most plausible and is the most convenient mathematically (reviewed in (Jacquet and Szpankowski
1998)). Then all relevant results for CFU per neonate can be readily computed from the results in Section S2.2.
The most important example for our purposes is the final eradication probability EF, which is given in terms
of the lineage non-extinction function ε(t) as
E( t ) exp[ (t) N( 0 )] EF exp[ (F) N( 0 )]. (S 2.4.1 )
Often deterministic analyses of similar situations regard Eq. (S.2.4.1) as a self-evident result. It isn’t, but under
our assumptions it follows from the fact that ε(F) is the parameter of a random thinning of CFU lineages. The
fundamental Poisson color theorem (Grimmett and Stirzaker 2001) states that the final CFU-lineage/patient
distribution is Poisson with parameter N(0)ε(F). Thus the final probability of the zero class is exp[-N(0)ε(F)],
i.e. Eq. (S2.4.1) holds. Aside: in contrast to the lineage per patient distribution, the CFU per lineage distribution
starts out deterministically, as a point mass at 1, and can eventually become very different from Poisson, with a
variance much larger than its mean (Hanin 2004).
S3. Details of the calculations: equations used, R scripts, tables of results
S3.1 Equations used in paper.
Collecting results from our paper, from S2.1 and S2.4 above, and from (Nielsen et al. 2009, Mohamed et al.
2012, Nielsen and Friberg 2013), we can write out the ODE used in our calculations. The meaning and values of
the parameters, taken from the references, are reviewed in section S3 below.
The PK model uses two auxiliary functions of time, a concentration input function val(t) and the time
dependent clearance CL(t). These are defined as follows, where σ is a step function.
val( t )
dose0 * (t,0 , ) dose1* (t,T 1,T 1 ) ...
with ( t ,t1,t 2 ) 1 for t1 t t 2 & 0 otherwise.
thetaVC * 1 GAVc* ( GA - GAmed )*
CL( t ) thetaCL*WT 0.75 * 1 thetaGACL* ( GA GAmed )* 1 ( t / 24 )thetaPNACL .
(S 3.1.1)
The three compartment PK ODE for the three concentrations c(t), p1(t), and p2(t) are:
Qi* c Qi* pi
Qi* pi Qi* c CL( t )* c
; dc / dt i
val( t ),
VC
Vi
VC
VC
Vi
where c( 0 ) 0 pi ( 0 ).
(S3. .1 )2
for i 1,2 : dpi / dt
Using c(t) calculated from Eq. S3.1.2 we can define the key auxiliary function DRUG(t), a killing rate for
bacteria, and define ksr(t), as follows.
DRUG( t )
Emax 0 * c(t)* AR50
;
EC 50 c( t ) ARon( t ) AR50
ksr( t ) ( Kgrowth Kdeath )* ( s r ) / Bmax. (S3.1.3)
For reasons explained in the text, ksr(t) plays only a minor role in the deterministic calculations and was set
equal to zero outright in the stochastic calculations.
The deterministic and stochastic PKPD ODE are, using c(t) from Eq. 3.1.2 and using Eq. 3.1.3:
ds / dt Kgrowth - Kdeath -DRUG( t ) - ksr( t )* s
dr / dt ksr( t )* s - Kdeath* r
(S3.1.4)
dm / dt Kgrowth - Kdeath - DRUG( t )* m
d / dt Kgrowth Kgrowth - Kdeath - DRUG( t )*
dARoff / dt Koff * ARon - Kon* ARoff * c(t)
dARon / dt Kon* ARoff * c( t ) - Koff * ARon.
For t=0: s 4.83* 10 , r 0 , m 1, 0 , ARoff 1, ARon 0.
5
Here Φ is the stochastic correction factor of section S2.4 and, which is unusual in stochastic process theory, the
stochastic results can be calculated using an ODE instead of more complicated methods.
Solving the equations 2.5.4 computationally (next Section) gives the eradication probability E(t) by using Eqs.
S2.2.1 and S2.4.3. E(t) and c(t) give the entries in the tables that are our main results.
S3.2 PKPD.R script
This section describes source codes we used for the paper. We believe that in the long run only an open-source,
free (gratis), free (libre) software approach can make in silico PK/PD a sound, powerful, credible tool for
clinicians; therefore our R scripts and auxiliary files are freely available from the widely used github repository,
https://github.com/radivot/gentaPKPD, or from our server http://epbi-radivot.cwru.edu/gentaPKPD/ or from the
corresponding author by email.
Our PK calculations used some, but not all, of the methods in Nielsen et al (Nielsen et al. 2009). We
considered the premature neonate with GA=25 weeks and birth weight WT=0.778 kg and the term neonate with
GA=40 weeks and WT= 3.5 kg. All other parameters were fixed at the central values in table III, column
“combined data set” in (Nielsen et al. 2009). Thus we omitted the Monte-Carlo based population PK aspect of
(Nielsen et al. 2009) and our subsequent PD estimates concern how stochastic effects affect a particular neonate
rather than a population of neonates. Perhaps because of this difference our numerical results and our graphs
differ somewhat from those shown in (Nielsen et al. 2009, Mohamed et al. 2012). For our purposes, e.g.
comparing front with back loading for some reasonable scenarios, these differences are not vital. For selfconsistency, consistency with other literature, and to avoid subscripts and Greek letters in R scripts, the notation
of (Nielsen et al. 2009) has been modified as follows: (1) subscripts are written on the main line and θ->theta.
An example which uses both these changes is θGACL thetaGACL; (2) CL->thetaCL; (3) V1->thetaVC (with
thetas added for self-consistency and C as usual standing for the central compartment); (4) TVV1->VC , Q2>Q1, V2->V1, Q3->Q2, V3->V2.
Our PD calculations applied the methods and parameters of (Mohamed et al. 2012) to the results of our PK
calculations, with two additions. The main addition consisted of using the IID-CFU stochastic process of
Section S2 on the S compartment (see Fig. 2 of the paper) to calculate an eradication probability E(t). The other
addition was using deterministic PK to calculate some comparatively familiar effectiveness and toxicity indices
based on free drug concentration. The main outputs were Figs. 4 and 5 of the paper. The following script,
PKPD_6.R, implements these calculations.
#This script uses methods similar to (Nielsen et al 2009 Clin Pharmacokinet 48:253) for neonatal gentamicin dosing and
#corresponding PK/PD calculations in Mohamed et al. 2012, Antimicrob Agents Chemother 56:179. It adds stochastic calculations.
#in the stochastic calculation of eradication probability E(t) the simplified model with ksr=0=r at all times was used.
#Written and commented by Nopphon Siranat April 2014; tested, modified and further commented by Rainer Sachs
#sachs@math.berkeley.edu. Further edits were done by Tom Radivoyevitch. Distributed under the GNU GPLv3; Contact Sachs for .txt or.R versions.
library (deSolve) #We will solve systems of non-linear first order ODE (ordinary differential equations)
#The next few commands are adjustable by the user; they set the dosing pattern and the gestational age GA.
#For details, including meaning of parameters, see Nielsen et al. For self consistency and consistency with other literature,
#the notation of Nielsen et al. has been modified as follows: (1) subscripts are written on the main line and (Greek lower case theta)->"theta"
# an example which uses both these changes is (Greek lower case theta)_GACL->thetaGACL;
#(2) CL->thetaCL; (3) V1->thetaVC (with C standing for the central compartment); (4) TVV1->VC, Q2->Q1, V2->V1, Q3->Q2, V3->V2.
GA =40 #gestational age (weeks); possible values are 25, 29, 34, 40; determines neonate parameters such as weight
#dose<-rep(2.2,4); interval<-c(0,rep(12,3),4) #
#drug doses (mg/kg); intervals (hours) between doses. For example dose= c(5,4,4) and interval=c(0,24,24,4)
#would mean a bolus of 5 at t=0, fractions of 4 at 24h intervals, and then a 4 h dose-free recovery period.
#dose<-c(4,4); interval<-c(0,24,52) #may give an error message later when running multiregimenPKPD.R
dose<-c(4,4,0,0); interval<-c(0,rep(24,3),4)#But This works later (any 76 hour regimen with 3 or four doses)
#dose<-rep(4,6); interval<-c(0,rep(36,5),60)#Fig. From Nielsen et al.
time = cumsum(interval[-length(interval)])
step<-.01; SPH<-1/step #ODE output times: step=time (h) for one output step; SPH=steps per hour.
#Generally in this script, time can refer to hours, days, weeks, or number of steps; one has to keep track.
times<-seq(0,sum(interval),by=step) #Time ranges for the ODE output, for example 76 hours in 7601 steps
#************** end of user adjusted parameters *************
weight=c('25'=0.778,'29'= 1.200,'34'=2.710,'40'=3.500) #WT=weight (kg) of neonate at post natal age (PNA)=0 days;
#Next define a PK response to one dose, assuming 3 compartments: central, 1, and 2
concentration<-function(t,state,parameter){ #t=time; state is drug concentration (c,p1,p2) as function of t
with(as.list(c(state,parameter)),{#now define some auxiliary fctns, then number (3) of ODE & of unknown functions.
WT = unname(weight[toString(GA)])
CL=thetaCL*(WT^0.75)*(1+thetaGACL*(GA-GAmed))*(1+((t/24)^thetaPNACL)) #allometric clearance; theta indicates a covariate.
VC = thetaVC*WT*(1+GAVc*(GA-GAmed)) #volume VC of central compartment depends on GA; see Nielsen et al
dose = parameter['doses']$doses; time = parameter['times']$times
concs=with(as.list(parameters),dose/(thetaVC*(1+GAVc*(GA-GAmed))))
val = 0
for (ii in 1:length(dose)){
val = val + concs[ii]*(time[ii]< t & t < time[ii]+delta)
}
val = val/delta
dp1 <- Q1*c/VC - Q1*p1/V1 #dp1, dp2, dc= time derivatives; Q1,Q2=wash rates; V1,2=volume of peripheral cmpt. 1,2.
dp2 <- Q2*c/VC - Q2*p2/V2 #time rate of change of concentration in peripheral compartment 2.
dc <- - Q1*c/VC + Q1*p1/V1 - Q2*c/VC + Q2*p2/V2 -CL*c/VC + val #rate of change of concentration in central cpt.
list(c(dp1,dp2,dc)) #output of the function concentration; defines the 3-compartment model
})
}
parameters <-c(thetaVC = 0.406,V1=0.305, V2=4.55, thetaCL =0.01, Q1 = 0.0930 , Q2 = 0.0155,# Table III "combined dataset" in Nielsen et al.
GAmed= 28.9,thetaGACL = 0.0871, #making thetaGACL larger, e.g. thetaGACL= 0.12,
#would give bacterial count curves closer to those of Mohamed et al. but would be ad hoc.
GAVc= -0.0114, thetaPNACL=0.517, Kgrowth= 2,Kdeath=0.179, Bmax=8.26e8, BP =2.09e6, gamma = 1,
Emax0= 51,EC500= 9.85, AR50= 0.113,Kon=0.0426,Koff=0.0139, doses = list(dose), times = list(time), delta = 0.08)
#central values used, not "population" PK/PD. Koff=0.0139 (-->half-life=50 h), fixed by Mohamed, may be unrealistically small.
#Emax0= 51,EC500= 9.85, AR50= 0.113,Kon=0.0426,Koff=0.0278, doses = list(dose), times = list(time), delta = 0.08)
#PK model for getting concentration from all doses. The above concentration function is only for one dose.
#This new function will help superimpose concentration from different doses by looping through intervals
conccurve = function(dose, interval,GA){
out2<-ode(y=c(p1=0,p2=0,c=0),times=times,func=concentration,parms=parameters)#events = list(data = eventdat))
return(out2)
}
out = conccurve(dose,interval,GA) #output of above
conc = out[1:nrow(out),4] #nrow=1+sum(interval)/step; 4=concentration in vc (1=time (h), 2 & 3= conc. in v1 & v2)
conc = conc[-1] #remove the first component (which is 0)
#Now predict CFU number as a function of time. CFU are bacteria that are cycling
#and also not "adaptively" drug resistant.
#Some of the calculations are similar to those used in Mohamed et al. The main method will be
# solving a system of non-linear first order ODE for deterministic and stochastic models.
#conc is now a vector with, for example, 7601 components
countfunc <- function(conc){
concfunc <-splinefun(conc) # temporarily make concentration into a function
state <-c(s=4.83e5, r=0,m=1,corr=0, ARoff = 1, ARon = 0) #initial (t=0) values for 6 ODE in 6 unknowns
#s=bacteria per mL; r quiescent (for us usually remains 0); m and corr (same as PHI) auxiliary functions (see text);
#AR is adaptive resistance; ARon, ARoff are fractions with and without adaptive resistance
withdrug<-function(t,state,parameters){ #model for number of CFU taking into account drug effects
with(as.list(c(state,parameters)),{#following lines give the derivatives in the ODE and some auxiliary quantities
C = concfunc(SPH*t) #get concentration from spline
EC50 = EC500 #not EC500*(1 -exp(-10*Cr*t)); the optional extra factor of the references is never used in our calculations
dARoff <- Koff*ARon-Kon*ARoff*C #the ODE for no adaptive resistance; d=time derivative
dARon <- Kon*ARoff*C - Koff*ARon #time derivative of the fraction of CFU that have acquired adaptive resistance
Emax <- Emax0*(1-ARon/(ARon+AR50)) #Emax model
DRUG <- (Emax*C^gamma)/(EC50^gamma+C^gamma) #The drug effect on bacterial killing
ksr<-(Kgrowth-Kdeath)*(s+r)/Bmax #ksr is transfer rate constant from cycling to quiescent bacteria; in our
#calculation the number of quiescent bacteria remains 0 until CFU numbers become so large stochastics no longer matter
if(s<BP) ksr = 0 #ksr with cutoff; for calculating eradication probability E(t) gives same results as no cutoff
ds<-Kgrowth*s-(Kdeath +DRUG)*s-ksr*s #growth and death equation for cycling bacteria
dr<-ksr*s-Kdeath*r # r is # quiescent bacteria, not susceptible to the drug even for AR off. Set=0 when calculating E(t)
dm<-(Kgrowth-Kdeath-DRUG)*m #m*4.83e5 approximates s if ksr is small;
dcorr<-Kgrowth+(Kgrowth-Kdeath-DRUG)*corr #corr is a stochastic correction used in stochastic models.
list(c(ds,dr,dm,dcorr,dARoff,dARon)) #output of the function withdrug
})
}
count<-ode(y=state, times=times,func=withdrug,parms=parameters) #output from the withdrug function showing
#the number of CFU and of other relevant quantities at time t
return(count)
}
count = countfunc(conc)
dtrmn<-count[ ,'s']/4.83e5 # Deterministic S/S(0), where s is number in central compartment
on<-count[,"ARon"]# the fraction of bacteria that have adaptive resistance at time t
####### Collect results needed to plot figures ######################################
thetaCL = 0.01
WT = unname(weight[toString(GA)]) #weird way to get weight
GAmed= 28.9 #Median for many observations, see Nielsen et al.
thetaGACL = 0.0871 #helps calculate correction of clearance for GA different from median.
thetaPNACL=0.517 #another covariate
t= seq(0,sum(interval),by=step) #for example t= 0, .01, .02, ..., 75.99, 76 in some cases.
a = round(t/24)*24 # using a instead of t in the following line gives step functions as in Nielsen et al. smooth is preferred here
CL=thetaCL*(WT^0.75)*(1+thetaGACL*(GA-GAmed))*(1+((t/24)^thetaPNACL))# gives smooth function; more plausible mechanistically
GAVc= -0.0114
factor<-.406*WT*4.83e8*(1+GAVc*(GA-GAmed)) #initial average number of CFU PER BABY NOT PER mL; vc = thvc*WT*(1+GAVc*(GAGAmed))
print(min(factor*dtrmn))
nonzero<-count[ ,"m"]/(1+count[,"corr"]) #stochastic estimate for prob 1 lineage has not gone extinct (ksr=0 approximation)
finalnz<-nonzero[(sum(interval)-1)*SPH]
cure<-exp(-factor*nonzero) #probability every lineage has gone extinct, E(t) in text.
print(cure[(sum(interval)-1)*SPH])#approximates long time limit E_F of E(t)
########## To make various figures, uncomment the following lines######
# # Check that figures are similar to those in Nielsen et al. and Mohamed et al. Add stochastic extinction plot
par(fin=c(4,5),ann=FALSE, mai=rep(.1,4),xaxp=c(0,sum(interval[-length(interval)]),1))# parameters specifying layout
plot(out[ ,"time"],out[ ,"c"],ylim=c(0,17),xlim=c(-1,sum(interval)),yaxp=c(0,16,4),type='l') # concentration as a function of time
abline(h=c(0,2,8,10,12,14,16),lty=2)
ex<-cumsum(interval)+1
points(ex,conc[SPH*ex],pch=8) # points one hour after each dose fraction shown as asterisks
legend(20,9,legend=c(dose,GA), cex=.5)
title(paste0("Doses=",paste(dose,collapse=","),"; GA=",GA))
plot(times,factor*dtrmn,log='y',ylim=c(.1,1e15),xlim=c(step, sum(interval)), type='l') #plot the number of CFU versus time
abline(h=c(1,100,1e8), lty=2) #horizontal lines as in Mohamed Figs 4, 5, 6 bottom row.
legend(x=5,y=1e11, c(dose,GA),cex=.65)
lines(times,factor*count[ ,"m"], lty=3) #deterministic ksr=0 approximation
plot(on, ylim=c(0,1),type="l") #fraction of CFU that have acquired adaptive resistance
lines(CL,type='l', lty=2) #Clearance for central compartment increases as baby ages
legend(20*SPH,.6,c(dose,interval[2], GA),cex=.75)
plot(cure, type="l",ylim=c(0,1)) #extinction probability E(t)
abline(h=cure[length(cure)])
#round(conc[c(10,1198,1210,2398,2410,3598,3610,4798,4810,5998,6010,7198,7210)],2)#used for Table III of paper.
As an over-all check of the script, we simulated a hypothetical neonate with a very mild infection, so mild the
initial number of CFU was ~50 instead of ~109. We considered just one dose at birth so small that the
eradication probability E(75) was ~50%. Then we were able to check the results of PKPD.R with a Monte Carlo
simulation so different that any errors would presumably have shown up.
S3.3 Other scripts
We also streamlined the script of section S3.2 to give E(75) and deterministically calculated free drug
concentrations putatively relevant to effectiveness and toxicity for a list of different dosing regimens. The
script, MultiregimenPKPD.R and a sample input file are available as described in S3.1. The output was the
following Table. The “Doses” column of the table gives 72 hour (h) dosing protocols followed by a 4 h
recovery period; the interval between doses is 36 h if three doses are listed, 24 h if 4 doses are listed. The
remaining column headings in the table are, for GA =25 weeks and then GA=40 weeks, the extinction
probability EF estimated from E(75) and then free drug concentrations (mg/mL) in the central compartment at
0.1, 23.99, 24.1, 35.99… hours. For example the first infusion lasts from 0 h to 0.08 h so we look at 0.1 h.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
Doses
2.5,7,0,0
3,6,0,0
4,0,0,0
4,4,4
4,7,7
4,4,0,0
4,4,4,0
4,4,4,7
4,4,5,4
4,4,7,4
4,5,4,4
4,6,4,4
4,7,0,0
4,7,4,4
4.5x4
5,0,0,0
5,6,6
5,4,0,0
5,4,4,4
5,5,5,5
6,0,0,0
6,4,4
6,6,6
6,3,0,0
6,4,0,0
6,4,4,0
6,4,4,4
7,0,0,0
7,4,0
7,4,0,0
7,4,4,0
7,4,4,4
E25
0.00
0.00
0.01
0.01
0.01
0.01
0.01
0.01
0.01
0.01
0.01
0.03
0.04
0.79
0.05
0.16
0.16
0.17
0.17
0.67
0.53
0.53
0.53
0.56
0.66
0.70
0.70
0.83
0.83
0.97
0.99
0.99
0.1
5.82
6.98
9.30
9.30
9.30
9.30
9.30
9.30
9.30
9.30
9.30
9.30
9.30
9.30
10.47
11.63
11.63
11.63
11.63
11.63
13.96
13.96
13.96
13.96
13.96
13.96
13.96
16.28
16.28
16.28
16.28
16.28
23.99
1.17
1.41
1.87
1.87
1.87
1.87
1.87
1.87
1.87
1.87
1.87
1.87
1.87
1.87
2.11
2.34
2.34
2.34
2.34
2.34
2.81
2.81
2.81
2.81
2.81
2.81
2.81
3.28
3.28
3.28
3.28
3.28
24.1
17.44
15.35
1.87
1.87
1.87
11.17
11.17
11.17
11.17
11.17
13.49
15.82
18.14
18.14
12.56
2.34
2.34
11.63
11.63
13.96
2.80
2.80
2.80
9.78
12.10
12.10
12.10
3.27
3.27
12.57
12.57
12.57
35.99
5.43
4.92
1.22
1.22
1.22
3.89
3.89
3.89
3.89
3.89
4.56
5.22
5.89
5.89
4.37
1.53
1.53
4.19
4.19
4.86
1.83
1.83
1.83
3.83
4.50
4.50
4.50
2.14
2.14
4.81
4.81
4.81
36.1
5.41
4.90
1.22
10.52
17.49
3.88
3.88
3.88
3.88
3.88
4.54
5.20
5.87
5.87
4.36
1.52
15.47
4.18
4.18
4.84
1.83
11.12
15.77
3.82
4.48
4.48
4.48
2.13
11.43
4.79
4.79
4.79
47.99
3.42
3.10
0.81
3.41
5.36
2.47
2.47
2.47
2.47
2.47
2.89
3.31
3.72
3.72
2.78
1.01
4.91
2.68
2.68
3.09
1.22
3.82
5.12
2.46
2.88
2.88
2.88
1.42
4.02
3.08
3.08
3.08
48.1
3.41
3.09
0.81
3.40
5.34
2.47
11.76
11.76
14.09
18.73
12.18
12.59
3.71
13.01
13.23
1.01
4.90
2.67
11.96
14.70
1.21
3.80
5.10
2.46
2.87
12.17
12.17
1.42
4.01
3.07
12.37
12.37
71.99
1.44
1.32
0.40
1.40
2.14
1.08
2.62
2.62
3.01
3.78
2.79
2.96
1.59
3.13
2.95
0.50
2.00
1.18
2.72
3.28
0.60
1.60
2.10
1.11
1.28
2.82
2.82
0.70
1.70
1.39
2.92
2.92
72.1
1.44
1.32
0.40
10.69
18.40
1.08
2.61
18.88
12.29
13.06
12.08
12.25
1.59
12.42
13.40
0.50
15.93
1.18
12.01
14.88
0.60
10.89
16.03
1.11
1.28
2.81
12.11
0.70
1.69
1.38
2.92
12.21
E40
0.06
0.27
0.60
0.60
0.60
0.68
0.68
0.68
0.69
0.91
0.92
1.00
1.00
1.00
0.97
0.92
0.92
0.99
0.99
1.00
0.99
0.99
0.99
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
0,1
7.01
8.42
11.22
11.22
11.22
11.22
11.22
11.22
11.22
11.22
11.22
11.22
11.22
11.22
12.62
14.03
14.03
14.03
14.03
14.03
16.83
16.83
16.83
16.83
16.83
16.83
16.83
19.64
19.64
19.64
19.64
19.64
23.99
1.21
1.45
1.93
1.93
1.93
1.93
1.93
1.93
1.93
1.93
1.93
1.93
1.93
1.93
2.17
2.41
2.41
2.41
2.41
2.41
2.89
2.89
2.89
2.89
2.89
2.89
2.89
3.38
3.38
3.38
3.38
3.38
24.1
20.81
18.24
1.92
1.92
1.92
13.12
13.12
13.12
13.12
13.12
15.92
18.72
21.52
21.52
14.76
2.40
2.40
13.60
13.60
16.40
2.88
2.88
2.88
11.28
14.08
14.08
14.08
3.35
3.35
14.56
14.56
14.56
35.99
6.26
5.54
0.81
0.81
0.81
4.10
4.10
4.10
4.10
4.10
4.92
5.74
6.56
6.56
4.61
1.02
1.02
4.30
4.30
5.12
1.22
1.22
1.22
3.69
4.51
4.51
4.51
1.42
1.42
4.71
4.71
4.71
36.1
6.21
5.50
0.81
12.01
20.41
4.07
4.07
4.07
4.07
4.07
4.89
5.70
6.52
6.52
4.58
1.01
17.81
4.27
4.27
5.09
1.21
12.41
18.01
3.66
4.48
4.48
4.48
1.41
12.61
4.68
4.68
4.68
47.99
2.41
2.14
0.34
3.35
5.61
1.59
1.59
1.59
1.59
1.59
1.91
2.22
2.53
2.53
1.79
0.42
4.94
1.68
1.68
1.99
0.51
3.52
5.02
1.45
1.76
1.76
1.76
0.59
3.60
1.85
1.85
1.85
48.1
2.39
2.12
0.34
3.32
5.57
1.58
12.78
12.78
15.58
21.17
13.09
13.40
2.51
13.71
14.37
0.42
4.90
1.67
12.86
15.97
0.50
3.49
4.99
1.44
1.75
12.95
12.95
0.59
3.58
1.83
13.03
13.03
71.99
0.36
0.33
0.08
0.46
0.75
0.26
1.21
1.21
1.45
1.92
1.25
1.30
0.39
1.34
1.36
0.10
0.68
0.28
1.23
1.51
0.12
0.50
0.69
0.25
0.30
1.25
1.25
0.14
0.52
0.32
1.27
1.27
72.1
0.36
0.33
0.08
11.65
20.33
0.26
1.20
20.78
12.63
13.10
12.44
12.48
0.39
12.52
13.94
0.10
17.46
0.28
12.41
15.49
0.12
11.69
17.48
0.25
0.30
1.24
12.43
0.14
0.52
0.31
1.26
12.45
Tables I and II of the paper consist of selected excerpts from the table. Excel (.xlsx) versions of the table can be
obtained from running MultiregimenPKPD.R at http://epbi-radivot.cwru.edu/gentaPKPD/ or by email from the
corresponding author. An R script for statistics (Fig. 6 of the paper) is available similarly. In the statistical
calculations we used 5 decimal place accuracy for the E(75) values in order to prevent ties.
Robustness of the results relative to changes in the parameter Koff, the rate constant that resting bacteria
return to the cycling state, was analyzed. The table above is for half-life 50 h. Results for half-life 25 hours are
in the next table, They predict larger values of E(t) and for most daily dosing regimens a bigger influence of the
day 3 and 4 doses on E(75).
Doses
2.5,7,0,0
3,6,0,0
4,0,0,0
4,4,4
4,7,7
4,4,0,0
4,4,4,0
4,4,4,7
4,4,5,4
4,4,7,4
4,5,4,4
4,6,4,4
4,7,0,0
4,7,4,4
4x4.5
5,0,0,0
5,6,6
5,4,0,0
5,4,4,4
5,5,5,5
6,0,0,0
6,4,4
6,6,6
6,3,0,0
6,4,0,0
6,4,4,0
6,4,4,4
7,0,0,0
7,4,0
7,4,0,0
7,4,4,0
7,4,4,4
E25
0.00
0.00
0.03
0.03
0.03
0.03
0.03
0.03
0.04
0.77
0.15
0.94
0.79
1.00
0.57
0.35
0.35
0.45
0.57
1.00
0.73
0.73
0.74
0.83
0.95
0.99
0.99
0.93
0.93
1.00
1.00
1.00
t=0.1
5.82
6.98
9.30
9.30
9.30
9.30
9.30
9.30
9.30
9.30
9.30
9.30
9.30
9.30
10.47
11.63
11.63
11.63
11.63
11.63
13.96
13.96
13.96
13.96
13.96
13.96
13.96
16.28
16.28
16.28
16.28
16.28
23.99
1.17
1.41
1.87
1.87
1.87
1.87
1.87
1.87
1.87
1.87
1.87
1.87
1.87
1.87
2.11
2.34
2.34
2.34
2.34
2.34
2.81
2.81
2.81
2.81
2.81
2.81
2.81
3.28
3.28
3.28
3.28
3.28
24.1
17.44
15.35
1.87
1.87
1.87
11.17
11.17
11.17
11.17
11.17
13.49
15.82
18.14
18.14
12.56
2.34
2.34
11.63
11.63
13.96
2.80
2.80
2.80
9.78
12.10
12.10
12.10
3.27
3.27
12.57
12.57
12.57
35.99
5.43
4.92
1.22
1.22
1.22
3.89
3.89
3.89
3.89
3.89
4.56
5.22
5.89
5.89
4.37
1.53
1.53
4.19
4.19
4.86
1.83
1.83
1.83
3.83
4.50
4.50
4.50
2.14
2.14
4.81
4.81
4.81
36.1
5.41
4.90
1.22
10.52
17.49
3.88
3.88
3.88
3.88
3.88
4.54
5.20
5.87
5.87
4.36
1.52
15.47
4.18
4.18
4.84
1.83
11.12
15.77
3.82
4.48
4.48
4.48
2.13
11.43
4.79
4.79
4.79
47.99
3.42
3.10
0.81
3.41
5.36
2.47
2.47
2.47
2.47
2.47
2.89
3.31
3.72
3.72
2.78
1.01
4.91
2.68
2.68
3.09
1.22
3.82
5.12
2.46
2.88
2.88
2.88
1.42
4.02
3.08
3.08
3.08
48.1
3.41
3.09
0.81
3.40
5.34
2.47
11.76
11.76
14.09
18.73
12.18
12.59
3.71
13.01
13.23
1.01
4.90
2.67
11.96
14.70
1.21
3.80
5.10
2.46
2.87
12.17
12.17
1.42
4.01
3.07
12.37
12.37
71.99
1.44
1.32
0.40
1.40
2.14
1.08
2.62
2.62
3.01
3.78
2.79
2.96
1.59
3.13
2.95
0.50
2.00
1.18
2.72
3.28
0.60
1.60
2.10
1.11
1.28
2.82
2.82
0.70
1.70
1.39
2.92
2.92
72.1
1.44
1.32
0.40
10.69
18.40
1.08
2.61
18.88
12.29
13.06
12.08
12.25
1.59
12.42
13.40
0.50
15.93
1.18
12.01
14.88
0.60
10.89
16.03
1.11
1.28
2.81
12.11
0.70
1.69
1.38
2.92
12.21
E40
0.82
0.90
0.77
0.77
0.77
0.93
0.94
0.94
0.97
1.00
1.00
1.00
1.00
1.00
1.00
0.97
0.97
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
0.1
7.01
8.42
11.22
11.22
11.22
11.22
11.22
11.22
11.22
11.22
11.22
11.22
11.22
11.22
12.62
14.03
14.03
14.03
14.03
14.03
16.83
16.83
16.83
16.83
16.83
16.83
16.83
19.64
19.64
19.64
19.64
19.64
23.99
1.21
1.45
1.93
1.93
1.93
1.93
1.93
1.93
1.93
1.93
1.93
1.93
1.93
1.93
2.17
2.41
2.41
2.41
2.41
2.41
2.89
2.89
2.89
2.89
2.89
2.89
2.89
3.38
3.38
3.38
3.38
3.38
24.1
20.81
18.24
1.92
1.92
1.92
13.12
13.12
13.12
13.12
13.12
15.92
18.72
21.52
21.52
14.76
2.40
2.40
13.60
13.60
16.40
2.88
2.88
2.88
11.28
14.08
14.08
14.08
3.35
3.35
14.56
14.56
14.56
35.99
6.26
5.54
0.81
0.81
0.81
4.10
4.10
4.10
4.10
4.10
4.92
5.74
6.56
6.56
4.61
1.02
1.02
4.30
4.30
5.12
1.22
1.22
1.22
3.69
4.51
4.51
4.51
1.42
1.42
4.71
4.71
4.71
36.1
6.21
5.50
0.81
12.01
20.41
4.07
4.07
4.07
4.07
4.07
4.89
5.70
6.52
6.52
4.58
1.01
17.81
4.27
4.27
5.09
1.21
12.41
18.01
3.66
4.48
4.48
4.48
1.41
12.61
4.68
4.68
4.68
47.99
2.41
2.14
0.34
3.35
5.61
1.59
1.59
1.59
1.59
1.59
1.91
2.22
2.53
2.53
1.79
0.42
4.94
1.68
1.68
1.99
0.51
3.52
5.02
1.45
1.76
1.76
1.76
0.59
3.60
1.85
1.85
1.85
48.1
2.39
2.12
0.34
3.32
5.57
1.58
12.78
12.78
15.58
21.17
13.09
13.40
2.51
13.71
14.37
0.42
4.90
1.67
12.86
15.97
0.50
3.49
4.99
1.44
1.75
12.95
12.95
0.59
3.58
1.83
13.03
13.03
71.99
0.36
0.33
0.08
0.46
0.75
0.26
1.21
1.21
1.45
1.92
1.25
1.30
0.39
1.34
1.36
0.10
0.68
0.28
1.23
1.51
0.12
0.50
0.69
0.25
0.30
1.25
1.25
0.14
0.52
0.32
1.27
1.27
72.1
0.36
0.33
0.08
11.65
20.33
0.26
1.20
20.78
12.63
13.10
12.44
12.48
0.39
12.52
13.94
0.10
17.46
0.28
12.41
15.49
0.12
11.69
17.48
0.25
0.30
1.24
12.43
0.14
0.52
0.31
1.26
12.45
S4 A Front Boosting Theorem
This section generalizes a mathematical theorem known from radiotherapy treatment planning (Sachs et al.
1996, Fakir et al. 2013).
S4.1 Stochastic process theory in radiation biology and tumor radiotherapy treatment planning.
The main radiobiological counterpart of PK is the study of the stochastic energy deposition tracks produced
by high energy charged particles passing through biological matter. For example in typical x-ray therapy
incident photons produce electron tracks that kill tumor cells, mainly by damaging their DNA. For well over 65
years a gradually increasing research effort has been devoted to developing Monte Carlo software simulating
stochastic energy deposition tracks of electrons and other particles. Powerful new packages have been
developed in the last few years; one is conveniently available to all researchers (http://www.geant4.org/geant4/
accessed April 16 2014). They are computationally more intensive than PK software, but the results have fewer
uncertainties due to comparatively greater reliance on physics and radiochemistry vs. biology. They are being
mined for biological implications [e.g. (Friedland and Kundrat 2013, Girdhani et al. 2013)].
Among radiobiological counterparts to PD is a stochastic process formalism first applied to tumor control
probability estimates around 1990 [e.g. (Tucker et al. 1990, Hanin et al. 1994);Sachs, 1996 #19] and since
extended. As recently used in treatment planning for individualized, conformal, boosted, fractionated x-ray
tumor therapy (Fakir et al. 2013), the formalism analyzed deterministic models, e.g. exponential or S-shaped
logistic, of CFU growth between radiation dose fractions, the relevant CFU being stem-like cancer cells. It
compared each deterministic model with a stochastic process counterpart. As often in tumor treatment modeling
(Hanin and Zaider 2014), the effectiveness index was the predicted probability of eradicating all CFU. The
calculations showed that deterministic models usually underestimate the usefulness of front dose boosting
compared to back boosting.
S4.2 Notation and assumptions
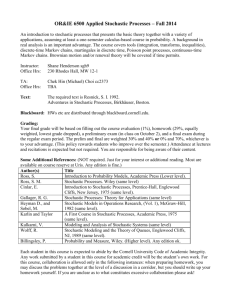
Fig. S1 indicates some of the main notation. All the regimens considered will consist of a single cycle
Figure S1 An example of a dosing regimen. Shown is a hypothetical regimen
consisting of one cycle of one bolus each weekday. Two dose fractions, given on Monday
of weeks 2 and 3, are twice as large as the others. The total number of dose fractions is
denoted by K (15 in this example). The time of the kth fraction is denoted by Tk
(k=1,…,K).
The time for the first dose is chosen as t=0. During a recovery period (RP) the drug clears and short-term
patient toxicity effects ameliorate. Here the recovery period is shown as 4 days and the final time F is thus 22
days. We will always assume a regimen includes a RP so long that drug concentration at time F and the
difference E(F)-EF are both negligible
One major difference between radiotherapy treatment planning and PK/PD for anti-bacterial drugs is that in
radiotherapy an acute dose can often be approximated as acting instantaneously whereas a drug bolus typically
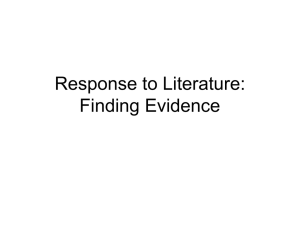
elevates free drug concentration c(t) for an extended period. To take this difference into account let us introduce
a continuous, nowhere-negative shape function S(t) with support in [0,RP] and unit area (Fig. S2).
Figure S2. Concentration shape
Suppose that we have time translation invariance (“autonomy”) in the
sense that the free drug concentration cj(t) due to dose fraction dj depends
only on the time difference t-Tj. Specifically, assume cj=f(dj)S(t-Tj) where
f(u) is a monotonic increasing function of u and f(0)=0. Thus
c( t ) k 1 f ( dk )S( t Tk )
K
( S 5.1.1 )
An example where such autonomy does not hold is given by our
gentamicin analyses, due to modulating factors (Fig. 5 of the paper) such as the time-dependent ratio of neonate
weight to volume.
Suppose also that CFU PD is a Feller-Arley-Kendall process with per-CFU death rate d(t)=de(t)+αc(t),
where de(t) is the endogenous per-CFU death rate and α is a constant. Such linearity in concentration does not
hold in our gentamicin analysis either, because of the development of CFU adaptive resistance at a CFUnumber dependent rate. However, the above assumptions are good approximations for some clinical situations
(e.g. brachytherapy with repeated rapidly decaying implants) and also supply instructive examples, applicable to
any dosing cycle, of the influence of stochastic fluctuations on PD predictions about dose boosting.
S4.3 Results
To see the implications of these assumptions, we may as well, in view of the IID nature of Feller-Arley-Kendall
processes, focus on lineages. Specifically, since Eq. (2.4.1) gives the E(t) (the eradication probability for the
whole CFU population) directly as a monotonically decreasing function of ε(t) (the non-extinction probability
for a single lineage), we will focus on Eq. (S2.2.3), i.e. ε=m/(1+ Φ), for the stochastic corrections Φ to the nonextinction probability ε for one lineage.
The deterministic equation (S2.2.1B) for average CFU number m(F) at the final time F (see Fig. S1) gives,
since m(0)=1 for lineages and Eq. (S4.1.1) is here assumed, the following result.
F
K
(A) m(F) me (F)exp k 1 f ( d k ) ; where ( B ) me (F) exp b( ) d e ( ) d .
0
( S 4.2.1)
Here me(F) is just the final average CFU number if no treatment is given; (A) shows that this average is
K
multiplied by an exponential killing factor exp k 1 f ( dk ) due to the drug treatment. The fact that the
killing factor depends only on the sum of the f(dk) (Jusko 1971) means that the order in which the doses are
given does not matter to the deterministic estimate of final average CFU number. For example the deterministic
calculation asserts, under our assumptions, that the idea of first decreasing average CFU number by repeated
equal doses and then giving a boosted dose to finish off the CFU population is simply wrong: exactly the same
final average would be predicted by the deterministic calculation if the boosted dose were first instead of last.
However analyzing the stochastic correction factor Φ in ε=m/(1+ Φ) uncovers a systematic preference for
front boosting. Suppose we have two dose fractions with dj > dj* and with j>j* so that Tj > Tj*, i.e. the bigger
dose comes later. Let us compare this regimen to the dosing regimen where the two doses are switched, so the
bigger dose comes earlier. Write the integral in Eq. (S2.2) for Φ(F) in the following form:
(F) dt b(t)exp [ b( ) de ( )]d h( t ), where h exp d k 1 f ( d k )S( Tk ) . ( S 4.2.2 )
0
t
t
F
F
F
K
Here the function of t in the curly brackets is, for all t, the same for both dosing regimens and is greater than
zero. For h(t) our assumptions on f(u) and S(u) imply the following comparisons: (1) For t<Tj*, h(t) is the same
for both regimens; (2) for Tj* < t <(Tj+RP), h(t) is smaller for the back boosted regimen; (3) for Tj +RP< t, h(t)
is again the same; here if j*=1 or j=K respectively then (1) or (3) respectively is to be regarded as an empty t
interval. These properties of h(t) imply that overall Φ(F) is always strictly larger for the front-boosted regimen,
which implies, since m(F) is the same for both regimens that ε(t) is smaller for the front-boosted regimen, which
in turn implies that EF is larger for the front boosted regimen.
The advantage of having a mathematical theorem is that it covers all possible dosing regimens, so lengthy
Tables like I and II are not needed. However, the restrictions for the theorem’s validity exclude non-linear
effects of free drug concentration on CFU death rate, and exclude CFU adaptive resistance. So the theorem
cannot be applied directly to neonatal gentamicin treatment calculations, serving only to help explain the
results. The intuitive reason for the greater effectiveness (as judged by EF) of front-boosting is, very roughly,
the following: once a CFU population is eradicated by chance fluctuations, then any extra future growth
promised by b(t) is simply wasted, since there are no CFU left to grow. Thus, it is best to bring population
numbers close to zero as early as possible, so that the amount of time spent near zero, where 0 can be reached
by chance, is a great as possible. This intuitive reason applies to many processes less special than the FellerArley-Kendall process, so the possibility of deterministic calculations under-estimating the effectiveness of
front loading should, we would argue, always be kept in mind. Of course front loading has long been considered
in many treatment protocols for many other reasons.
S5. Supplement Bibliography
1. Campillo, F., M. Joannides and I. Larramendy-Valverde (2013) "Estimation of the parameters of a stochastic
logistic growth model." arXiv.org; http://arxiv.org/abs/1307.2217.
2. Fakir, H., L. Hlatky, H. Li and R. K. Sachs (2013). "Repopulation of interacting tumor cells during
fractionated radiotherapy: Stochastic modeling of the tumor control probability (editor's pick)." Medical Physics
40: 121716.
3. Friedland, W. and P. Kundrat (2013). "Track structure based modelling of chromosome aberrations after
photon and alpha-particle irradiation." Mutat Res 756(1-2): 213-223.
4. Girdhani, S., R. Sachs and L. Hlatky (2013). "Biological effects of proton radiation: what we know and don't
know." Radiat Res 179(3): 257-272.
5. Grimmett, G. and D. Stirzaker (2001). Probability and random processes. Oxford, Oxford University Press.
6. Hanin, L., L. Pavlova and A. Yakovlev (1994). Biomathematical problems in optimization of cancer
radiotherapy. Boca Raton, FL, CRC Press.
7. Hanin, L. and M. Zaider (2014). "Optimal schedules of fractionated radiation therapy by way of the greedy
principle: biologically-based adaptive boosting." Phys Med Biol 59(15): 4085-4098.
8. Hanin, L. G. (2004). "A stochastic model of tumor response to fractionated radiation: limit theorems and rate
of convergence." Math Biosci 191(1): 1-17.
9. Jacquet, P. and W. Szpankowski (1998). "Analytical depoissonization and its applications." Theoretical
Computer Science 201(1): 1-62.
10. Jusko, W. J. (1971). "Pharmacodynamics of chemotherapeutic effects: dose-time-response relationships for
phase-nonspecific agents." J Pharm Sci 60(6): 892-895.
11. Kendall, D. G. (1948). "On the generalized birth and death process." Ann. Math. Stat. 19: 101-117.
12. Kimmel, M. and D. E. Axelrod (2002). Branching Processes in Biology. New York, NY Springer.
13. Michor, F., T. P. Hughes, Y. Iwasa, S. Branford, N. P. Shah, C. L. Sawyers and M. A. Nowak (2005).
"Dynamics of chronic myeloid leukaemia." Nature 435(7046): 1267-1270.
14. Mohamed, A. F., E. I. Nielsen, O. Cars and L. E. Friberg (2012). "Pharmacokinetic-pharmacodynamic
model for gentamicin and its adaptive resistance with predictions of dosing schedules in newborn infants."
Antimicrob Agents Chemother 56(1): 179-188.
15. Nielsen, E. I. and L. E. Friberg (2013). "Pharmacokinetic-pharmacodynamic modeling of antibacterial
drugs." Pharmacol Rev 65(3): 1053-1090.
16. Nielsen, E. I., M. Sandstrom, P. H. Honore, U. Ewald and L. E. Friberg (2009). "Developmental
pharmacokinetics of gentamicin in preterm and term neonates: population modelling of a prospective study."
Clin Pharmacokinet 48(4): 253-263.
17. Ovaskainen, O. and B. Meerson (2010). "Stochastic models of population extinction." Trends Ecol Evol
25(11): 643-652.
18. Sachs, R. K., W. F. Heidenreich and D. J. Brenner (1996). "Dose timing in tumor radiotherapy:
considerations of cell number stochasticity." Mathematical Biosciences 138(2): 131-146.
19. Tan, W. (2002). Stochastic models with applications to genetics, cancers, AIDS, and other biomedical
systems. London, World Scientific.
20. Tucker, S. L., H. D. Thames and J. M. Taylor (1990). "How well is the probability of tumor cure after
fractionated irradiation described by Poisson statistics?" Radiat Res 124(3): 273-282.