The Subliminal Therapy Flow Charts
advertisement

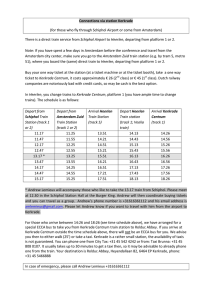
Subliminal Therapy: The New Paradigm for Psychotherapy Syllabus 19th International Conference Association of Psychology and Psychiatry for Adults and Children Subliminal Therapy Institute, Inc. www.stii.us Copyright 2014 2 Table of Contents Page Course Schedule . . . . . . . . . . . . . . 3 The Guiding Rule . . . . . . . . . . . . . . 4 The Concept of Subliminal Therapy . . . . . . . . 4 The Origin of Subliminal Therapy . . . . . . . . . 4 Treating Addictions With Subliminal Therapy . . . . . 5 Treating Depression With Subliminal Therapy . . . . . 7 Treating Chronic Pain . . . . . . . . . . . . . 9 Treating Chronic Pain Using Subliminal Therapy . . . . 14 Clinical Success Rates of Subliminal Therapy . . . . . 16 Certification in Subliminal Therapy . . . . . . . . 16 Yager Subjective Effects Inventory (YSEI) . . . . . . 19 The Subliminal Therapy Flow Charts . . . . . . . . 20 Verbal content for the Steps of the Flow Chart . . . . 23 Website Links . . . . . . . . . . . . . . . . 29 3 Course Schedule 1500 – 1630 Personal Introduction The Concept of Subliminal Therapy Demonstration of the Use of Subliminal Therapy Discussion of the Demonstration 1645 – 1800 Relationship Between Hypnosis and Subliminal Therapy Theory and Assumptions of Subliminal Therapy The ST Model of the Mind Introducing Centrum Establishing Communications With Centrum Validating that Communication Demonstration of Subliminal Therapy Discussion of the Demonstration 1830 – 1945 Applying Subliminal Therapy Subliminal Therapy protocol Setting the Stage to Use Subliminal Therapy Defining and Refining the Goal of Therapy Uncovering the Subconscious Cause/Roots Reframing the Uncovered Information Test Completion of the Work When Possible Demonstration of Subliminal Therapy Discussion of the Demonstration 2000 – 2100 Areas of application of Subliminal Therapy Treating psychological/emotional problems Treating psychogenic physical disorders Effectiveness Research Data Collection and Processing Results and Conclusions Certification The Subliminal Therapy Institute, Inc. 4 The following items are not included in any particular order; they are complementary to the textbook, Subliminal Therapy: Using the Mind to Heal. The Guiding Rule Anytime I preface a question with the name “Centrum” the nest words you speak to me will be the words Centrum has written on your chalkboard. The Concept of Subliminal Therapy Subliminal Therapy is a generalized, psychodynamic-based approach to treating mental disorders, as well as psychogenic physical illness. It is psychotherapy in which the patient is guided to employ mental abilities that are universal to everyone, but commonly unrecognized. In application, the patient is guided to engage their own mental abilities to achieve desired change. Subliminal Therapy was conceived by Edwin K. Yager, Ph.D. and has evolved into a structured, cogent protocol during the past 35 years of use in clinical practice. During the past three years, Dr. Yager has collected data on the success rates of ST in the form of inventories completed by the patients before and after treatment, and again at follow-up. The inventory assesses areas of life in which the presenting problem has negatively impacted the patient, together with the degree to which that impact is present at the time the inventory is completed. The results of this research are updated as additional data become available and published on the website of The Subliminal Therapy Institute, Inc., (www.stii.us.). Data available before 2011are also published in Dr. Yager’s textbook on ST (Yager 2011). The Origin of Subliminal Therapy I am often asked about how ST originated, and my answer is seldom adequate. It has been about 40 years since that occurred, and allowing for a degree of memory impairment, I can best respond in terms of the circumstances at the time. My first copyrighted paper on ST is dated in 1975, following a period of speculation and discussion with my engineering colleagues who shared my curiosity about mental functioning. Conception must therefore have occurred in about 1974 when I began transitioning from my career in engineering into the field of mental health. I had begun to seriously study and teach clinical hypnosis; however, I had not yet begun my formal training in psychology. I had no knowledge of current treatment protocols and theory. There is a common belief that nothing is truly new, that knowledge evolves from earlier knowledge. It’s a well-founded argument that I generally endorse, but it doesn’t fit in this situation; I had no knowledge of psychology from which ST could have evolved. I was an engineer. My way of thinking about the world was (and still is) pragmatic, and thoughts about psychic issues had only recently begun to occur, largely in reaction to my studies of hypnosis. I began to wonder about how we function mentally, about how to explain the frequent presence of contradictions between conscious desire and conscious experience. I concluded we must have an unconscious level of superior 5 intelligence, a level having abilities not available to consciousness. I could not explain our functioning in life without that assumption. With the aid of hypnotic trance, I was able to establish meaningful communication with that domain in the minds of my patients and ST evolved as I explored and tested possibilities of the pragmatic use of the abilities of that domain. Out of my personal experience, and in contradiction to my earlier convictions about life that derived from my training as an engineer, I am compelled to acknowledge the reality of true inspiration, inspiration that defies reasoned explanation. Treating Addictions with Subliminal Therapy People speak of being addicted to street drugs and cigarettes, and express concern about becoming addicted to medications. People also speak of being addicted to a behavior such as gambling, and of being addicted to another person. These all accurately define “addiction” in that they refer to compulsions over which there is little or no conscious control. I propose an unconventional theory of addiction and I will propose an unconventional treatment protocol as well. The theory I propose evolved in the course of applying Subliminal Therapy (ST) in many cases of addiction - both drug and non-drug addictions - during the past 35 years. Sadly, in the early years I did so without documenting the results of my work. While I am subjectively confident the success rate in eliminating the addictions was uniquely high, I lack evidence to support that opinion. In recent years, however, I have documented the success rates of my work, and this data confirms the high success rates I expected. Nevertheless, since there are too few cases to declare validation of the theory, what I propose here is still “theory.” The theory is quite simple: “All addictions are essentially mental disorders; therefore, elimination of the addiction will require psychological intervention, not just medical management.” “Perhaps, but…” is a frequent rejoinder to that statement. It might seem I have ignored the profound influence of withdrawal in motivating the continued use of a drug. My response is to point out that, in the case of drug addiction, while withdrawal is a physiological process, it is mentally perceived. Without perception, there would be no awareness of withdrawal; therefore, even this aspect of addiction is essentially mental, and is clearly a disorder. Moreover, since perception can be altered by hypnotic technique, the distress of withdrawal can thus be eased during the treatment of the essential cause of the addiction. Drug Addiction With respect to withdrawal, assuming abstinence from a drug, its chemical influence yields its power over time as the chemical is metabolized by the body; the trauma of withdrawal fades with time. In illustration, in the case of tobacco smoke, the chemical elements are metabolized in about a week; in the case of heroin, months-to-years may be required. Psychological compulsion is the primary force that propels addiction beyond the distress of withdrawal, and this force can last for a lifetime. Compulsions are unconsciously rooted in classic conditioned response, in seeking pleasure, avoidance of pain or, in the case of drug addiction, may be rooted in fear of the consequence of not using the drug. In all events, compulsions are “learned,” 6 they are the consequence of conditioning from life experiences. That being true, “re-conditioning” becomes the cure for addiction. And since re-conditioning is the essence of ST, ST is the preferred treatment for addiction. A review of the cases I have treated affirms that the major component of drug addiction is the compulsion to abuse, and therefore psychological intervention – not just medical treatment – is essential if the addiction is to be successfully eliminated. This compulsive component was “the elephant in the room” in all of the cases reviewed. Meanwhile, in support of the psychotherapy, withdrawal was mitigated by other means, and in each case the compulsion was found to be the consequence of conditioning, conditioning that occurred during the course of life-experiences. This pattern is identical in sequence to the etiology of almost all other problems I have successfully treated using ST. Non-Chemical Addiction Addictions to behaviors, people, gambling, exercise, etc., share the element compulsion with drug additions; they are not able to not experience the drive again and again and again. They are not able to not think about the experience; an obsessive element has crept in. Another truth held in common with drug additions is that the person who is non-chemically addicted does not know the actual psychological cause/s of their addiction. Our innate need for explanations for things that happen can prompt the person to rationalize explanations for being addicted, and such explanations are plentifully offered in my practice, but they are not found to be accurate when adequately explored. Once the actual cause is uncovered, patients are consistently surprised to learn what it is. Treatment As in treating all psychogenic disorders, the conscious belief in a fabricated cause of the addiction must be discounted. In using ST, it must be ignored. Conscious opinion of the cause must be set aside to permit the protocol to flow as it should. The greatest single challenge in employing ST lies in differentiating between expressed conscious opinion and the information communicated from the unconscious domain of the person. When treating someone who is immersed in the distress of withdrawal, that distress must be relieved before psychological intervention is possible. At least to some extent, the distress will fade with abstinence; however, relief can be accelerated by medication and/or by hypnotic techniques. Nevertheless, relief must be achieved to the extent that the person can function intellectually. Once the mind is clear, assuming the person is consciously motivated to eliminate the addiction, the protocol for treating addiction by ST is the same as for treating other psychogenic disorders. A highly important aspect of treatment of drug addictions is to follow the patient for at least the duration of the metabolism of the addicting chemical. Failure to do so invites relapse as related issues surface, issues that can also be resolved with ST as they arise. 7 Treating Depression With Subliminal Therapy Depression is not a disorder in and of itself; it is a reaction to other problems. Successful treatment of depression requires resolution or reframing of those problems. As viewed by the medical model, depression is a consequence of chemical imbalance within the brain. As viewed by the model of Subliminal Therapy (ST), depression is the cause of the chemical imbalance. If the ST model is accurate, psychological treatment is clearly indicated; if the medical model is accurate, psychological treatment can be effective only to the extent that it can directly impact the chemical imbalance. The current standard of treatment protocols embrace a combination of psychotherapy and medication. In this article, I will first address Depression; I will then speak to Bi-Polar Disorder as they relate to the use of Subliminal Therapy. Depression manifests in many ways, not all of which are obvious. The symptoms may be physiological: disturbed sleep, loss of appetite or libido. Gastrointestinal distress or loss of energy may be present. Immune function may be impaired, leading to physical illness. The first symptoms may be irritability, malaise or even manic behavior. Also, absent significant correction of the life situation or proactive intervention, symptoms are apt to gain intensity over time, and possibly multiply as well. A diagnosis of depression is made when a combination of predefined symptoms are present, and there are no guides or limits to the selection from the list of possible symptoms. Unlike anxiety, obsessions, phobias etc. - that have clearly defined and required patterns of symptoms - depression is a “catch all” diagnosis that has no rigid definition. For example, if a person is conditioned to be anxious by one experience, conditioned to have insomnia a year later in another experience, and conditioned to feel malaise in a third experience, that combination of entirely separately created symptoms could be diagnosed as depression. And this could be true even though no other symptoms of depression were present during any of the conditioning experiences. The Beck Depression Inventory is a frequently used measure of the level of depression, and is simply a listing of possible symptoms with levels of significance in each case. The final score on the Beck is a total of these scores without regard to any specific pattern or selection of the symptoms. Treatment of depression by ST involves addressing the specific causes underlying the diagnosis of depression, rather than addressing “depression” as an entity. In the protocol of ST, when the apparent causes have been individually resolved, an inner search is conducted to identify any remaining, unrecognized yet contributing influences, which are then also resolved. When all contributing causes have been resolved, the depression is no longer apparent. Sad things happen to all people. That’s part of the game of life. Among other causes of depression, there is a natural reaction to sad experiences, which normally recedes with time and adaptation. Clinical depression happens when it doesn’t recede, when the sad condition continues, possibly exacerbated by other sad things that happen. Depression compromises reason and perspective, and can also compound the depression itself by unrealistically sensitizing the sufferer to minor sad things that otherwise would not be perceived. 8 Insidiously, this happens without conscious awareness that it is happening, precluding conscious defense, and precluding conscious repair of the essential cause because the cause is not known. Actually, the cure for depression is quite simple; eliminate its cause, or change the person’s perspective of the cause, thereby eliminating the effect of the cause. Of course, in either case, one must know what the cause is, and therein lies the problem. In almost all cases, the patient has not recognized all causes at a conscious level, and so is unable to address it. The patient may have conscious knowledge of some aspect of the cause, which may be seen as the cause, without fully understanding it. Even the knowledge that is conscious has probably never been subjected to rational evaluation, which would relieve the depression to some extent. In short, barring identification of the true cause/s, the patient is trapped and can only mask the depression with medication or hypnotic techniques. In either case only temporary relief is likely; continuing, repeated reinforcement is required, and tolerance becomes a factor. Eliminating depression by eliminating the cause is a far better road to travel. This road is the road of Subliminal Therapy. If the assumption of psychogenesis of depression is accurate – that the depression is the consequence of conditioning from life experiences – reconditioning must be possible. This is true because we are intelligent creatures, capable of learning. Conditioning comes from learning, and we are capable of relearning. Given new information, we are capable of understanding, in a different way, what we once understood on the basis of more limited information. It is by this means that we grow intellectually. It is also by this means that using ST provides the opportunity for reconditioning. As new information is uncovered and considered in the light of current knowledge, understanding changes, resulting in a different consequence. As previously unrecognized influences from past experiences are uncovered and reframed in the light of objective reason, the depression lifts. Considering the option of changing the person's attitude toward the cause: Just as in the first solution (eliminating the cause), the true cause must be uncovered and its influence resolved. Nevertheless, in some cases at least some causes are known. It might be the loss of a loved one or other obvious event that has resulted in exaggerated and/or prolonged distress, or guilt for an omission, or an act related to that loss, that is regretted. The person may recognize that the depression is dysfunctional and without purpose, yet not be cognizant of the reason it is as it is. Straightforward, rational reframing of known information may suffice to resolve the depression if the causes are accurately known; however, it is wise to probe for influence that has not been recognized, preferably by Subliminal Therapy. In some cases, depression can be so severe that psychological treatment is not possible. In severe depression, rational thought may not be possible, rendering psychotherapy impossible. In these cases, reducing the intensity of the depression is mandated if psychotherapy is to take place, and reduction may only be accomplished by medication, or in the extreme by electroconvulsive treatment. Hypnotic reduction of this depression is compromised by the person’s inability to think clearly. Bi-Polar Disorder (BP) is characterized by alternating cycles of depression and mania. There is compelling evidence of familial correlation and common belief that it is a genetic malady. There are devastating consequences and its incidence is on the order of 4%, fairly consistent in all cultures. The actual etiology of BP is not yet understood; however, there are not many arguments favoring psychogenesis, the presence of at least genetic predisposition to BP is strongly apparent. One plausible 9 theory holds that the depressive component is a psychogenic consequence of the trauma of the mania (which is not psychogenic) and must therefore be amenable to psychotherapy. Regardless of theory, the depressive component of the BP cycle can at least be moderated by psychotherapy, especially by ST, and in many cases the manic episodes can be moderated by direct hypnotic suggestion. Meanwhile, there are at least modestly effective medications for the management of BP symptoms, albeit with unfortunate side effects. Treating Chronic Pain Introductory Concepts One’s values, beliefs, responses, behaviors and reaction to stimuli all develop as a consequence of conditioning from life experiences and chronic pain can represent such a conditioned response. The concept of chronic pain developed here is psychological in nature and not supportive of current pain theory, which cannot fully explain either the cause or elimination of physical pain. The conclusions reached here are contrary to conventional theory; still, they attempt to explain experience, rather than relying on textbook physiology. Much of the basis for this concept of chronic pain derives from the author’s success in treating pain following his discovery and development of the psychodynamic psychotherapy, Subliminal Therapy. Our mental capacities include the ability to perceive pain and to not perceive it; that is, to be consciously unaware of a stimulus that would be expected to cause pain. Given that everyone has the mental capacity to not perceive pain, why not engage it to avoid pain in all situations? The answer lies in the certainty that pain is needed for survival. In one respect or another, pain serves a purpose. It can be protective, stimulating the person to seek needed medical attention or prompting avoidance of risky behavior. And yet, pain may be present in other situations in which it does not have apparent purpose or identifiable cause. Patients may not recognize hidden benefits of pain, and the consequence in some situations may be a chronic, persistent state of pain, leading to suffering and disability. Pain is often considered to be an exclusively biological process; however, theories of pain based on physiology are not adequate to explain phantom limb pain, the elimination of pain by hypnotic suggestion, or the fact that surgical severing of nerves does not necessarily relieve pain. Pain may continue to be experienced long after an injury, without evident purpose or cause. Moreover, pain may be felt at an elevated level of intensity that is inconsistent with the severity of the physical stimulus. Treating chronic pain psychologically requires a means to go beyond the patient’s limited conscious understanding of its cause; subconscious influence must be identified. Insight regarding the cause may serve that purpose, and yet insight alone is not sufficient; the insight must be integrated and resolved within the subconscious domain of the patient’s mind for protracted relief to occur. Instances of chronic pain that is falsely claimed for economic gain, or for other consciously known reasons, are not addressed here. Perception of Pain Humans “perceive” things through the senses, and at least to some extent the option exists to consciously pay attention - or not - to perceptions. War stories are replete with examples of acts of heroism in the presence of serious injury; in entertainment hypnosis subjects may be guided to perceive 10 a chicken on their head, or perceive the audience to be absent. Clinically, hypnotically guided absence of perception of pain is also possible; childbirth and surgery with hypnosis as the sole anesthetic are common examples. Conscious perception can be dramatically altered by hypnotic suggestion, as well as by emotion. Perception varies over time, circumstance and with emotion, sometimes modified by factors that seem unrelated to the stimulus. Persistent pain, stimulated by influence from past experience, may persist without conscious awareness of its actual cause, with only the effect – the pain – consciously perceived. Possible Genesis of Chronic Pain According to the International Association for the Study of Pain: Pain Definitions (2011), "Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage." Although adequate as a definition of acute pain, this widely embraced definition does not explain many chronic pain situations. Migraine headaches, for example, do not involve tissue damage, nor do many other manifestations of pain. An adequate definition must embrace the existence of psychogenic pain. Chronic Pain Initiated by Physical Trauma Physical injury causes pain, stimulating a response. Its purpose is clear; it motivates us to do whatever is necessary to relieve the pain. Acute pain is adequately explained by conventional pain theory until/unless it reaches chronicity. In that event, where the initial stimulus is not recurring and no physical cause is evident, the sustaining stimulus must be psychological. Moreover, it is likely that the patient is not consciously aware of the unconscious, psychological rationale supporting the stimulus. Trauma causes the production of adrenalin and, for reasons not clearly understood, adrenalin cements memories and their effects (Ewin, 2009, p101). In illustration, in a time of trauma and under the influence of adrenalin, a person might learn to associate pain with knowing he is alive. That association might have the consequence of causing pain in present life as a means of “knowing I’m alive.” The blatant irrationality of that learned response is not recognized subconsciously, where the continuing pain is being inspired; only the initial association matters there, and this essential factor may provide general explanation for the presence of much enduring, “chronic” pain. Chronic Pain in Consequence of Psychological Trauma or Subconscious Need Psychological factors can be the initial cause of pain, be a compounding influence, or may cause the continuation of pain that was initially inspired physically. As examples, guilt for overreacting in a situation or for mistakes of judgment, particularly if leading to a bad outcome, may have the consequence of self-punishment by means of pain; fear may cause muscle contraction that exacerbates low back pain, and learned associations may promote continuation of physically inspired pain. Psychogenic Causes of Chronic Pain Patients have uncovered the following listed causes of psychogenic pain during the course of treatment employing Subliminal Therapy. Without exception, the patients did not initially recognize these causes at a conscious level. In some cases the patient was initially so preoccupied with awareness of pain itself that other perceptions were excluded. In most cases there were expressed, inaccurate reasons or justification for their pain, and in all cases the patients expressed surprise upon learning the actual reason. There was an element of “irrational rationality” in each instance. Viewed in retrospect, the initial stimulus of chronic pain consistently has an element of rationality that does not apply in current life. 11 To get attention To relieve emotional pain To know I’m alive To avoid remembering To punish myself I’m being punished So I can make her feel guilty So I can void thinking about something So I can stay awake So I will continue physical therapy It is always there when ______ It is my destiny It is inevitable It is unavoidable Psychological Purpose of Chronic Pain Although acute pain is essentially a protective mechanism (Mannion, et.al., 2000), chronic pain can sometimes serve irrational purposes such as getting attention from others, self-punishment or distraction from unpleasant thoughts. Pain may subconsciously satisfy many possible needs. Pain exists because we perceive it. When pain persists unnecessarily, it is because we have been conditioned to continue to perceive it. If the person has learned (at a subconscious level) to expect pain to continue, or has subconsciously become aware that the pain has value in some way, that conditioned response will likely persist, causing continued pain in opposition to conscious desire, will and logic. Unfortunately, in the case of chronic pain the purpose is rarely known consciously; therefore, lasting relief will probably not be possible by direct, conscious intervention. By one means or another, the subconscious purpose must be uncovered and resolved for extended relief. As shown above, many possible psychological bases for chronic pain have been revealed. Regardless of the reason for continuing pain – the reason learned in the initial sensitizing situation – that reason always had legitimate importance in the initial situation, even though problematic in later situations. Phantom limb pain is a clear demonstration of the ability of the mind to create pain and it appears that migraine headaches may be another. The mechanism of the creation of psychogenic chronic pain may also be through the action of smooth muscle, muscle that is controlled at a subconscious level in reaction to earlier experience. In illustration, it is speculated that headaches are caused by smooth muscle action, generating cranial pressure while being controlled at that subconscious level in response to past experience. As another illustration, the action of the smooth muscles of the glands may generate antibodies that in turn create the pain of psoriasis. Still, in all cases the pain is psychogenic. Psychological Treatment of Chronic Pain Although episodes of chronic pain may appear to correlate with consciously identifiable, non-physical factors such as, “Its worse when I am stressed, when I go to bed / wake up / sit down / when my husband is in the room,” the correlation may not be consistent across or within patients; chronic pain also occurs at other times and for unimagined reasons. Unless the various factors associated with psychogenic, chronic pain are understood, resolution is not possible. Therefore, effective, clinical elimination of psychogenic chronic pain requires the identification of underlying psychological causes, followed by resolution of those causes. When causes are resolved, pain ceases to exist. Essential, Clinical Requirements for Treating Chronic Pain Psychologically Both ethical and pragmatic necessity requires clinicians to rule out physical causes of pain. Nevertheless, in some 12 instances there are clear indications that the presenting pain is psychogenic and, arguably, psychological treatment might precede medical treatment and perhaps make it unnecessary. Uncover the subconscious, psychological reasons for the presence of pain. Hypnotic trance can facilitate this step by utilizing age-regression techniques or ideo-motor inquiry. Ego State Therapy has demonstrated fair effectiveness in doing so, and even free association in trance can be effective to some degree). With Subliminal Therapy, the presence or absence of causal, subconscious influences is determined by rationally utilizing extra-conscious mental abilities that all humans have. Resolve the uncovered influences at the subconscious level. Once identified, resolution of the cause of chronic pain is usually accomplished by reframing the uncovered insight in the light of more mature understanding. For example, a memory of an event that was understood in one way at the time can be understood differently from the perspective of maturity, and this change in understanding changes its effect in present life. Treating Chronic Pain Using Subliminal Therapy If chronic pain is a conditioned experience, reconditioning to be without pain should also be possible. This is the intent and focus of the protocol of Subliminal Therapy in treating pain. Effectiveness has been remarkable (See success rate data page ) and the intervention is time-efficient as well. The underlying theory of Subliminal Therapy assumes that people are conditioned by their experiences in life, usually without conscious recognition when it is happening, and that such conditioning can result in both physical and mental disorders. Thus, the use of Subliminal Therapy is indicated when the pain is the consequence of experiences, the on-going influence of which is stored in the patient’s mind below conscious awareness. Chronic pain, hay fever, bronchial asthma, PTSD, anxiety, addictions, compulsions, obsessions and many sexual problems are all examples of such psychogenic disorders. In applying Subliminal Therapy, an assumed “higher level” of the patient’s mental functioning is identified and guided by the clinician to do the work of therapy. The existence of this “extra-conscious” ability is first established by rational discussion with the patient in which commonplace evidence of its influence and abilities are pointed out. The patient is then guided to subjective awareness of that level of mental functioning by establishing direct, rational communication with that domain. The clinician then guides the process of Subliminal Therapy with the patient consciously passive, even though consciously aware of the process. During the process of Subliminal Therapy, the patient’s conscious involvement is limited to one role: providing communication between his or her extra-conscious domain and the clinician, with the patient cognitively aware of the proceedings. By engaging extra-conscious abilities, Subliminal Therapy enables a patient to identify and resolve the actual subconscious cause of the pain – as opposed to what the patient might initially believe to be the cause. Tapping into this higher level of mental abilities facilitates both the identification of the cause and its resolution. Communications from that domain are consciously perceived by the patient and then verbally relayed to the therapist. Problem resolution takes place as the clinician poses a logical sequence 13 of questions and requests addressed directly to that extra-conscious level of functioning, receiving responses from that level via the patient’s conscious mind. This feature bypasses the limits and rationalizations of consciousness by rationally engaging this “higher level” ability to do the work of therapy. It is a feature unique to Subliminal Therapy. As Subliminal Therapy is employed, the mechanism of change is re-conditioning, the difference being that it takes place at a subconscious level. Previously held, dysfunctional, subconscious beliefs and values are revised. False understandings and convictions are exposed and corrected by exposure to the patient’s more mature knowledge and judgment. Once the true cause(s) of a problem have been identified, final resolution can be accomplished with the patient consciously involved in the process itself; however, resolution is often accomplished without conscious involvement. Almost without exception, the rationale and concepts of Subliminal Therapy are readily embraced by patients. It makes sense to them and offers new hope for desired change. Chronic conditions are commonly resolved within two-to-five sessions, leaving both the patient, and sometimes the clinician, pleasantly surprised. The following table presents the success rates of employing Subliminal Therapy to treat chronic pain in the private practice of the author. The data was collected during the past five years using the patientcompleted inventory, Yager Subjective Effects Inventory, (Yager, 2007), at the beginning of treatment, post-treatment and where possible at follow-up. All cases of chronic pain treated during the past five yeas are included in this data if the course of treatment was completed. 14 Success Rate Table Average Treatment Hours Addiction 2.1 Chemical Smoking Other 2.5 2.0 2.0 Anxiety General Anxiety OCD Panic D Phobic D Mood Anger Depression Guilt 4.2 2.1 2.8 1.5 .026 .028 .036 .039 3.0 2.0 2.8 4.4 2.9 Asthma GI Pain Weight Other 2.0 4.7 2.5 3.2 1.9 Performance Vaginismus 1.15 0.93 1.06 3.2 Physical Sexual Effect Size Cohen’s d 0.37 0.71 0.43 1.57 0.25 0.33 0.55 0.86 7.8 Average Improvement n Number Of Cases n > 80% 94% 10 9 98% 99% 84% 3 4 3 3 4 2 80% 57 39 87% 61% 85% 82% 24 17 12 10 19 5 9 6 82% 25 15 83% 79% 74% 12 4 8 7 3 4 68% 31 19 84% 75% 75% 57% 87% 2 3 14 3 9 1 1 9 0 6 97% 4 4 21 5.0 1.84 2.00 93% 100% 2 2 2 2 Sleep D 2.9 0.49 82% 8 4 Other 2.9 0.27 86% 19 16 15 Success Rates of Subliminal Therapy Success Rates – All Cases Combined All Cases Subjective Relief n Mean Standard Deviation Cohen’s d Effect Size r Average Treatment Time PostTreatment 79% 202 5.46 2.02 2.21 0.74 2.8 hours Follow Up > 3 months 71% 48 1.7 2.3 1.95 0.70 16 Success Rates of Treatment of Chronic Pain by Subliminal Therapy Structural Pain Migraine Headache d = 1.69, r = 0.65, T = 4.31 66% (33) <13> 35% (3) <9> 84% (10) <5> 77% (39) <3> d = 5.28, r = 0.94, T = 7.61 GI Pain d = 1.70, r = 0.65, T = 1.72 Other Pain d = 1.14, r = 0.50, T = 1.57 Totals d = 1.24, r = 0.50, T = 5.30 0% 20% () <> d r T 69% (54) <4> 44% (42) <4> 40% 66% (42) <29> 60% 80% 100% Mean Percent Improvement at End of Treatment Mean Percent Improvement at Follow Up Standard Deviation Number of Subjects Cohen’s d Effect Size Students T-Test Certification in Subliminal Therapy Clinicians may be Certified in Subliminal Therapy only by the Subliminal Therapy Institute, Inc. The qualifications and training for this Certification, as well as its responsibilities and privileges, are as follows: Qualifications: If a citizen of the United States, Applicant must be licensed as a health care clinician in the state of his or her practice. If not a citizen of the United States, Applicant must be established as a clinician in the health professions of his or her country. If a United States citizen, Applicant must hold membership in a professional organization commensurate with license. If not a citizen of the United Sates, Applicant must hold membership in a professional organization commensurate with his or her professional status. Training Requirements: 17 A minimum of six-hours of formal training in Subliminal Therapy is required for Certification. Formal training may be completed in the facilities of STI, Inc., or elsewhere under the supervision of a clinician who has been Certified by STI, Inc. A Certificate of Completion, or written certification of completion of such formal training by a clinician who is Certified in Subliminal Therapy, will satisfy the training requirement to qualify to take the Certification Examination. In addition to the textbook on Subliminal Therapy, Subliminal Therapy: Using the Mind to Heal, training material will be provided for the Applicant on the website of the Institute, www.stii.us. Following formal training, the Applicant must have observed a minimum of 15 hours of the clinical application of Subliminal Therapy, accomplished by a Certified clinician, either in person or by observing video recordings, prior to taking the Certification Examination. Certification Examination: The Certification Examination consists of a combination of 100 multiple choice and true-false questions, randomly selected from a battery of greater than 100 questions. The answers to the multiple choice questions are randomly positioned for each examination. This examination must be completed on-line. Individual, affirmative statements of all of the questions in the battery of questions will be available on the website of the Institute as an aid to studying for the examination. Specific questions and concerns may be posed via email to the Institute at info@stii.us. Applicant must pass the Certification Examination with a minimum score of 95%. A fee of $50 will be charged for each administration of the examination and the applicant will be permitted to re-take the examination as frequently as described. Proof of Competency: After passing the Certification Examination, Applicant must demonstrate proficiency in using Subliminal Therapy by applying Subliminal Therapy in real-life situations for a minimum of six hours under the direct supervision of a Certified clinician. The supervising clinician must certify in written form that the applicant has satisfactorily demonstrated proficiency. This demonstration of proficiency may be accomplished in a person-to-person setting or may be accomplished by means of a series of exchanged video-recordings in which the applicant is afforded critique of her or his performance. Application Procedure: Formal, written application for Certification is made after completion and verification of the requirements for Certification. The application is to be submitted in the form of a letter from the 18 Applicant, addressed to the President of the Institute. This letter must include details of qualifications, documentation of Training, verification of observations and Proof of Competency as described above. Qualifications must be affirmed by a detailed statement from the Applicant and documented by appropriate copies of licensure or other certificates of status. Training must be affirmed by a detailed statement from the Applicant. Proof of passing the Certification Examination will be satisfied by passing the examination in the facilities of STI, Inc., or via the internet. Proof of Competency with respect to performance will be satisfied by a Certification of Competency signed by the Certified supervising clinician. Final Approval of Certification: Final approval for the Applicant to be Certified may be granted by the President of STI, Inc. or by action of the Board of Directors of the Institute. After review of the application, additional information and/or documentation may be required, and the Applicant will be promptly notified of such requirement. Obligations of Certification: It is an obligation of a Certified person to encourage the use of Subliminal Therapy in those applications where its use is appropriate. It is an obligation of a Certified person to train other clinicians who are interested in using Subliminal Therapy. It is an obligation of a Certified person to maintain the standards for Certification as detailed here. Privileges of Certification: Your name, links and related data will be posted on the website of the Institute. You will be eligible for referrals from the Institute. You will have authorization to publicize your Certification in any responsible way. You will have access to consultants associated with STI, Inc. You will have access to restricted information on the website of the Institute. As opportunity and your availability coincide, you will have authority to train others in the use of Subliminal Therapy. 19 Yager Subjective Effects Inventory (YSEI) _____________________________________________________________ Patient name _____________________________________________________________ Presenting problem _________________________ Date For each question, please circle the number that provides your best answer. If an item does not apply, skip that item. During the past day – week – month (Please circle one): Not at all Severe To what extent are the symptoms present in your life? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem interfered with your social life? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem interfered with your family life? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem interfered with your sexual life? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem interfered with your spiritual life? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem interfered with your memory? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem interfered with your sleep? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem interfered with your appetite? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem interfered with your work life? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem interfered with concentration? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem been a cause of personal distress? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem caused you to feel depressed? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem caused you to feel anxious? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem caused physical problems? 0 1 2 3 4 5 6 7 8 9 10 To what extent has the above problem caused any other problem/s? If your response is affirmative, what is that problem? 0 1 2 3 4 5 6 7 8 9 10 If the treatment has been completed, were you satisfied with the results? No Yes 0 1 2 3 4 5 6 7 8 9 10 20 The Subliminal Therapy Flow Charts Introduction to the Flow Charts These flow charts are intended as aids in learning to apply Subliminal Therapy. The suggested accompanying words are presented and are also available on the website of the Subliminal Therapy Institute, www.stii.us. The steps presented are the steps I typically take, based on over thirty-five years of experience with Subliminal Therapy. These steps are not necessarily the best selection in terms of content, or in terms of order of presentation; they are, rather, my personal, biased view of the preferred path to take. Yours may be better, yet I suggest you begin learning Subliminal Therapy with mine. Following the flow charts, I offer suggested words for use in the steps of the flow charts. As the clinician, you will ultimately employ phrasing and expressions that are personally comfortable and natural for you to use. It is the meaning and flow that must be communicated. This is as it should be. Some clinicians will adhere to my words, and that’s okay too, as they are good words and have proven to be effective. Moreover, not all possible paths of treatment are covered by the flow charts, yet they will prove sufficient in most cases. Your knowledge and skills as a clinician will be required to devise alternate paths in other cases. Instructions for Using the Flow Charts These charts are intended for instructional purposes; they do not cover all possible courses treatment might take. They are adequate for many cases, but as many more will deviate to the extent of requiring innovation and creative thought on your part as the clinician. As you learn to use ST, you may find better sequences to use, and you are encouraged to use what works for you; nevertheless, the sequence provided is a tool to use in developing your skills. Practice is of course essential. Read the content until you know what the next words are apt to be. If you comprehend the logic of the flow of the process, you will find that it flows for you. Your patient will likely slip into trance during the instructions and establishing communications with Centrum. Therefore, you will not be observed as you read the content suggested for the flow charts. It will be important that you read in your own, natural voice, rather than a voice that reveals you are reading; this is easily achieved through minimal practice. Trust that the patient is involved in his or her own thoughts and experiences and will not be paying critical attention to your performance. Speak clearly and with confidence; all else will follow as you would wish. 21 Basic Flow Chart 100 NO 200 NO 201 NO 202 FAIL 203 NO 204 NO 205 YES 106 111 112 113 114 NO 206 115 YES FAIL 207 > ONE 208 116 COMPLETE 108 ONE FAIL 211 NO 212 YES 213 FAIL 214 NO 215 COMPLETE YES 107 210 NO YES 105 NO YES COMPLETE 104 110 COMPLETE YES 103 209 YES YES 102 NO YES YES 101 109 117 22 Extended Flow Chart 205 NO 209 105 NO 311 YES YES 302 303 NO 305 YES 211 NO 304 101 YES 306 111 NO 304 YES 110 212 NO 209 YES 110 214 NO 308 YES YES 310 309 NO 408 23 Verbal Content for the Steps on the Flow Charts Note that the flow is addressed to the problem of asthma for convenience in presentation. 100 Having “set the stage” to begin the process of Subliminal Therapy, you will now begin to follow the Flow Charts. Since you are advised to avoid assumptions, ensure that Centrum is aware of the conscious goal by asking. Do not assume Centrum is aware. Request that Centrum respond by writing the answer on the chalkboard. Asking Centrum to indicate completion by writing the work “complete” following the first half-dozen steps of the process may make it unnecessary to repeatedly ask for the chalkboard response at the end of succeeding steps; the responses will come without the request. Y - 101 N - 200 Centrum, are you aware of your conscious desire/concern regarding the asthma? Please respond by writing your answer on the chalkboard. 101 It is wise to ensure that Centrum is willing to be involved in the process. And if there is a negative response, it will be necessary to persuade Centrum to be involved. Here, your talents as a clinician come into play; however, it is rare that Centrum is not cooperative. Y – 102 N - 201 Centrum, are you willing to cooperate in this effort, to do some work as I guide you and teach you how, to accomplish your conscious goal? 102 Ask Centrum to complete the investigation as comprehensively as possible with the objective of Centrum achieving as complete an understanding as is possible at this time, and to indicate completion of the task by writing the work “complete” on the chalkboard. Y – 103 N - 202 Centrum, please investigate this issue. Review memories of events that may have had something to do with it and communicate with those parts that are involved. The objective, Centrum, is for you to understand how asthma became part of your life. Centrum, is my request clear to you? 103 Centrum, please complete that task as comprehensively as is possible at this time and let me know when you have done so, to the limit of your ability, by writing the word “Complete” on the chalkboard. 104 Again, make no assumptions. Ask Centrum if the investigation produced understanding of the cause of the problem. If not, you must approach the process in a way that will ensure the development of Centrum’s understanding. Centrum, do you now understand the cause of the asthma, how it came to be a part of your life and why it has continued? C - 104 F – 203 Y – 105 N - 204 24 105 Ask Centrum if the asthma is being caused by one or more parts of the mind. If more than one, you must guide Centrum to interact with each part independently, one-at-atime, through step 109 of the sequence. Y – 106 N - 205 Centrum, is asthma being caused by the action of one or more parts of your mind? 106 Centrum, I will now ask that you identify the part, or parts if there are more than one, of your mind that are actively causing the asthma so that you will be able to communicate with them. Centrum, is that purpose clear to you? Y – 107 N - 206 107 Centrum, please identify the part, or parts, and let me know when you have completed the task by writing the word “Complete” on the chalkboard. C – 108 F - 207 108 Ask Centrum how many parts are actively involved in causing the asthma to occur, or in interfering or preventing the goal from being accomplished. Centrum, how many such parts are actively causing the asthma? 109 Centrum may or may not be in communication with this particular part. You must ask. Centrum, are you in communication with that part? 110 111 Then, Centrum, please accomplish that task to the limit of your ability and let me know when you have done so by writing the word “Complete” on the chalkboard. 112 Avoid assuming success. Ask! Centrum, did you succeed in that task? Y – 111 N - 210 C – 112 F – 211 Y – 113 N - 212 It is possible that Centrum accomplished more than you requested, or may have identified other active parts. Centrum, please search to identify any remaining part of your mind that may still be in a position to cause the asthma to continue. Is one or more parts of you mind still active in any way, for any reason, that might cause the asthma to recur in your life? 114 Y – 110 N – 209 Explain to Centrum that the part is “stuck” in time, aware only of the information available at the time it was formed, and that it is in ignorance of present reality. Explain Centrum’s job as being that of educating the part about present reality, thereby becoming aware of present life situation, values, needs, etc. Centrum, please communicate with that part in the following way; First, please listen to the part. Find out what the part believes and why it believes what it believes. Then, Centrum, communicate to that part information about present reality. Centrum, that part is stuck in time at that time when it came into being, knowing only what it knew then, in ignorance of your life as it is now. Educate that part, Centrum, about present needs, values and life situation. Persuade that part to your way of thinking. Centrum, is my request clear to you? 113 1 – 109 >1 -208 The patient may strongly desire conscious awareness of the work just completed, may N – 114 Y - 109 25 be indifferent, or may not want to be aware. Nevertheless, conscious awareness does seem to afford value to the process and, unless there is an expression of conscious opposition, request that Centrum reveal that information to consciousness. Centrum, please elevate to consciousness the memories of those experiences in which you learned to experience asthma, as well as understanding of the work you just completed. Please do so by writing on the chalkboard, by an inner voice, memory, insight or any other means. Please write the word “Complete” when you have done so. 115 116 117 Inquire if the patient is satisfied with the information received. Ask if it all makes sense and if the patient could, if requested, describe the process by which the asthma became a part of his life. If satisfied, go to 116. If not satisfied, go back to 114 and persuade Centrum to reveal the information, or determine if one or more parts are preventing conscious awareness. In the latter case, guide Centrum to communicate with those parts, persuading them to permit conscious awareness. Express to the patient the fact that the real test of completeness of this work is in the real world, yet there is value in finding a way to test it here and now, so that if not complete, we can continue the process now. Ask the patient to use his or her imagination to project into the future, into a situation in which an asthma attack would be expected to occur. If the patient has difficulty imagining that situation, the work is not complete and Centrum should be asked to identify the part. Other tests may occur to you. Use them as necessary as an aid in decisions of the moment. C – 115 F - 214 S 116 N 114 F 216 S 117 The task of change is now complete insofar as it is possible to test at this point. Explain to the patient that, although it appears to be complete, the real test is in the real world, and that some additional part might have escaped detection and still be active causing the asthma. Assure the patient that if there is a continuation of the asthma, it simply means that the work is not yet complete and that taking succeeding steps will be even more efficiently accomplished, now that Centrum knows how to do the work more efficiently. To not provide the assurance that the work can be finally completed – even if the asthma should recur – is to risk premature withdrawal from treatment. Point out that recurrence would simply mean the work is not complete; it does not mean failure of the person or of the treatment. Excellent work, Centrum. Thank you. 200 SERIES 200 201 It may seem incongruous that Centrum is not aware of what is happening in the patient’s life, yet that sometimes occurs, and the patient is usually dysfunctional because of it. Your task is to make Centrum aware of the issue and one way is to ask the patient to verbalize the problem, in simple yet comprehensive terms, after requesting that Centrum listen. At this point in the process, you are dependent upon Centrum. It is necessary that Centrum develop understanding of causal factors and it is your job to facilitate this. It might be that Centrum simply does not understand what is expected, or that Centrum is unable to overcome 100 101 26 the blocking of some resistant part, or other issue. By appropriate questions to Centrum, based on your professional sense of the situation, clarify the problem and persuade Centrum to continue with the work. 202 Your request may not clear for a number of reasons; however, it is probably due to your not having phrased the request in terms Centrum could follow. Rephrase it as required, perhaps including a review of the concepts of Subliminal Therapy, and repeat the question. Centrum, please investigate this issue. Review memories of events that may have had something to do with it and communicate with those parts that are involved. The objective, Centrum, is for you to understand how asthma became part of your life. Centrum, is my request clear to you? 203 If you have requested that Centrum indicate when the task is complete by writing “complete” on the chalkboard, and there has been no response, it may be that you (or the patient) are being impatient and Centrum simply needs more time. Ask Centrum if that is the case. Centrum, are you involved in the process and need more time? If the answer is “Yes”: Okay, we will be patient, just let us know by the word “complete” when you have completed the task. 204 205 Re-phrase your request to Centrum. You must depend upon Centrum’s ability to access memories, etc., and perhaps Centrum did not understand your request as you intended it to be. Ensure that you speak of Centrum using the abilities of memory access, communication with other parts, etc., to uncover the needed information. 206 Repeat your request using different words and include elaboration and explanation as you sense is necessary. 207 Although usually not a problem, this question may not be understood by Centrum. Explain that it will be necessary for Centrum to communicate with the identified parts and that this step is necessary to set the stage for that to happen. 209 You may, or you may not, know how many parts are actually involved causing the presenting problem; you only know there are more than one. Ask Centrum to select one of the parts and to proceed with the protocol. When Centrum has cleared that part, ask Centrum to select another, and then another, until all have been cleared. 104 N 105 Y 302 106 107 109 Your task is that of establishing communication between Centrum and the identified part. While the part may not be willing to communicate, it us usually willing to consider new information if doing so does not require self-disclosure. Centrum, are you willing to communicate with the part? 210 C 104 It is possible that Centrum is actively causing the problem that is the focus of treatment. Centrum may disagree with the conscious opinion of the patient. Centrum, are you, you Centrum, are you causing (problem)? 208 Y– 103 N - 202 Somehow there has been a lack of clear communications to Centrum. Perhaps it had to do with Y 303 N 310 27 phrasing, or even with content. Repeat the instructions of 110 in different words, checking incrementally with Centrum to ensure understanding. 211 You have requested that Centrum indicate completeness by writing the word “complete” and no response has been forthcoming. Ask Centrum if more time is needed. If no, ask if Centrum is willing to do the work. 110 Y 111 N 101 Centrum, are you willing to establish communication and do the work as requested? 212 Centrum, did you succeed in establishing communication with the part, as I requested? 214 Unconscious entities may deny conscious awareness for reasons of protection or for other reasons that are considered valid. On the other hand, it may be that conscious awareness is not necessary to accomplish the goal. You won’t know unless you ask. Centrum, will conscious awareness be necessary to accomplish the goal? 216 Y 110 N 209 Y 114 N 308 Inability to imagine the desired situation without difficulty is clear indication that the work is not complete. Centrum, the work is apparently not complete. I therefore ask that you re-investigate the beginning of the asthma and learn what remains to be accomplished. Identify the part/s that continue to be active in causing the asthma. C 104 300 SERIES 302 You need to know Centrum’s reason for causing the asthma, since this is the root of the barrier to the consciously desired change. So, ask. Ask Centrum to write that reason, or to express by an inner voice, or by other means. When the reason is expressed, guide the patient to offer countering views – back and forth – until agreement is reached, then proceed on that agreement. 303 In this step, you are seeking a way to engineer communications between the part and Centrum. A fair assumption is that the part is fearful of exposure and the following approach has been highly effective in resolving the barrier. Centrum, is the part willing to consider information with the provision that it need not expose itself, that it is only required to listen? A “no” or “no response” to this question will challenge your professional ability to devise an approach that will overcome the barrier. One possible approach is to temporarily abandon Subliminal Therapy, perhaps using age-regression techniques to resolve the immediate aspect, then return to working with Subliminal Therapy. Perhaps request Centrum to select a different part to work with, then come back to this part after requesting the part to listen to the process. 304 Centrum, please communicate with the part. Inform the part about present life conditions, Y 305 N 304 28 needs, values and desires. Ensure that the part understands the negative consequences of its influence and persuade the part to support your conscious goals. 305 Here, the best bet is to assume that the part is, in fact, listening and to ask Centrum to communicate as though that is true. Assume the part is well-intended and appeal to that good intention C 110 Centrum, please communicate information to this part, information about present life conditions, etc. Be supportive of that part, Centrum, appeal to its good intentions. 306 307 308 The part agreed to listen, and apparently has listened to the appeal from Centrum. The next step is to engineer bi-lateral communications between the part and Centrum so that full, mutual understanding can be reached between them. Centrum, is the part now willing to communicate fully with you in an exchange of positions and opinions? Y 304 N 110 Centrum, please communicate further information to the part. This time, Centrum, appeal to the positive intention of the part, offer any information you believe may persuade the part to communicate with you. C 110 Make it clear that you are asking for the conscious opinion of the patient, ask if it is important to him or her to know, at a conscious level, about the work just completed. Some will insist on knowing, others will not want to know. -- Patient --, do you want to know, to understand consciously, what Centrum just accomplished? 309 The patient wants to know, and there is value in having that knowledge, therefore, this becomes the focus of therapy. With this goal in mind, guide Centrum to eliminate the barrier, perhaps by following the basic protocol of Subliminal Therapy. 310 There are many conceivable reasons why Centrum might be unwilling to continue. You might be able to anticipate the reason and respond effectively, or you might not know the reason. Ask if Centrum is willing to reveal the reason for the refusal and use this response (if provided) to persuade Centrum. Your talents as a clinician will be tested at this juncture. Be inventive, knowing that unless Centrum can be persuaded, you must shift to another mode pf treatment. - 400 SERIES 408 In some instances, patients are just curious about what is going on, in other cases they may strongly desire to know, and other cases they may not want to know. As the clinician, you are obligated to conform to the patient’s wishes insofar as you are able to do so; after all, it is the patient’s life. It might be that the prospect of “knowing” what actually happened is so overwhelming that the patient is unwilling to continue therapy; it is seen as a threat that must Y 309 N 408 29 not be accommodated. Pay attention to your instincts. Links American Society of Clinical Hypnosis Hypnotherapy Training Ltd www.asch.net http://advhyp.com Edwin K. Yager, Ph.D. www.docyager.com Subliminal Therapy Institute www.stii.us