Grant Application final version
advertisement

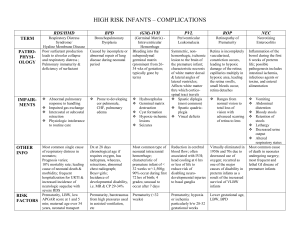
The Tulane Neonatal Outcomes Research Collaborative (TNORC) (A Pilot Grant Application) 1/11/2011 Submitted by Euming Chong MD, Robert Gordon MD, David Cupp MD, Jane Reynolds MD & Phillip Gordon MD, PhD (on behalf of the TNORC) TNORC co-directors: Phillip Gordon Euming Chong - (grant to be dispensed to Dr Chong if awarded) Members: Jane Reynolds Nancy Wood Julie Elzey Bill Gill Kathy Smith Angie Noya Betty Martinez Shelly Holcomb Affiliates / Collaborators: (co-authors italicized and current collaborators underlined) Robert Gordon (ophthalmology) & David Cupp (ophthalmology resident) - Tulane Tom Yeh (pediatric cardiac surgery) - Tulane Chi Dola (obstetrics) - Tulane Victor Lunyong (Ochsner) - LA Barry Bloom (Wesley Medical Center) - KS Karen Fairchild (University of Virginia) - VA Danny Benjamin (Duke University) - NC Reese Clark (Pediatrix Corp.) – SC Robert Christensen (Intermountain Health System) - UT Joshua Benjamin (pediatric resident) - Tulane ABSTRACT: THE TULANE NEONATAL OUTCOMES RESEARCH COLLABORATIVE Background: The Tulane Section of Neonatology has been steadily building local, regional and national collaborations in clinical research. This effort is now being formally designated as the Tulane Neonatal Outcomes Research Collaborative (TNORC). In 2011, we are moving from predominantly quality improvement-based projects, to a higher percentage of prospective trials and device-based investigations. TNORC has a firm commitment for a ten-fold increase in federal funding of NIH funded clinical research (including overhead) over the next year. We have ongoing projects matriculating that should quintuple the budget again within the next 5 years (with a planned follow up RO1 submission for the first neonatal multicenter randomized controlled trial ever based out of Tulane for $500,000 by 2012). Collaborators and parties of interest in the TNORC thus far include: neonatology (P Gordon, Chong & Reynolds), ophthalmology (R Gordon), maternal-fetal medicine (Dola), Ochsner neonatology (Lunyong), University of Virginia neonatology (Fairchild), The University of Kansas – Wesley Medical Center neonatology (Bloom), Intermountain Health System (Christensen), the NICHD fast start neonatal clinical trials program – based at Duke University (Benjamin), and pediatric cardiac surgery (Yeh). Objectives: The TNORC has four specific aims for 2011: 1) become a major site of enrollment for the NICHD acyclovir pharmacokinetics study in newborns (our 2nd participation in this rapid start study type). This study should bring in approximately $100,000 in NIH clinical study revenue. 2) Initiate our first device investigation of ophthalmic ultrasound as a means to measure opthalmic nerve sheath diameter (an indirect measure of intracranial pressure) in premature infants with and without intraventricular hemorrhage. This will be a real time study that documents the technology’s ability to quantify change in intracranial pressure without the use of MRI. It has limited corporate sponsorship. 3) Analyze, present and publish two recently completed multicenter studies that were both led by the TNORC (aminophyline as an adjunct to cooling therapy for hypoxic ischemic encephalopathy and zosyn versus ampicillin and gentimicin as first choice antibiotics in the NICU). The aminophylline study’s preliminary analysis looks promising as a roadmap for an RO1 submission to fund a multicenter randomized controlled trial. The zosyn study has not yet been analyzed but holds great promise for paradigm change. 4) Re-open our NICU follow up clinic (which has been closed since Katrina) as a resource for neurodevelopmental follow up in current and future studies. Plan: What the TNORC needs to be successful in 2011: The directors of the TNORC are requesting $35,000 during the year of 2011 to hire a mid level person as a part time study coordinator and data manager; plus $15,000 for equipment and supplies to help support data management; software for statistical analysis, matching and randomization; travel to meetings to present our studies (to help build support for our RO1 application); as well as developmental assessment tools necessary for the NICU follow up clinic (Bayley III & DPIII kits). Total request: $50,000. The current man power for the TNORC is being supplied 100% by physicians. We cannot continue to add studies to the TNORC roster without an expansion in dedicated personnel. We will not qualify for other studies if we do not have an active follow up clinic. Most importantly, the TNORC will not be able to participate in the National Children’s Study, without standardized developmental follow up. If the TNORC is to attract new (and support existing) external funding, it must develop rudimentary infrastructure and hire essential personnel. PROJECT DESCRIPTION: THE TULANE NEONATAL OUTCOMES RESEARCH COLLABORATIVE Introduction: TNORC has an ambitious agenda for 2011. Each of the four specific aims described in this proposal are designed to propel the collaborative forward as a research enterprise; building momentum, infrastructure, revenue and stature with each step of completion. Much like the PLAN->DO->STUDY->ACT cycles of quality improvement (PDSAs), TNORC is also planning and executing its own continual improvement. Our ultimate vision is to become a regional and national resource in neonatal clinical research. Specific Aim 1: To be one of only two sites in the “Open Label Study to Describe the Pharmacokinetics of Acyclovir in Infants” as summarized in the table below. Acyclovir is a commonly used medication in neonatology that, like many other drugs, has no pharmacokinetic data in newborns. The approximate reimbursement is $4000 per patient enrolled. The master grant for this study has more than 20 other target medications in the roster for similar analyses. Dr Danny Benjamin (the study co-PI), has offered us the opportunity to be one of these two sites. Dr Jane Reynolds would be the study coordinator. Phillip Gordon and Euming Chong will be the site Co-PIs. TNORC approved this protocol on 1/11/2011. Protocol Title An Open Label Study to Describe the Pharmacokinetics of Acyclovir in Infants IND Number: 106153 Product Acyclovir Objective: This study will evaluate the safety and pharmacokinetics of intravenous acyclovir in infants. Study Design: Single-center, open-label, pharmacokinetic study. Infants < 91 days postnatal age suspected to have a systemic infection. These participants will be divided into groups as determined by gestational and postnatal age: Group-1: 23-29 weeks gestational age, <14 days postnatal age Study Population: Group-2: ≥ 30 weeks gestational age, <14 days postnatal age Group-3: 23-29 weeks gestational age, 14-90 days postnatal age Group-4: ≥ 30 weeks gestational age, 14-90 days postnatal age Number of Participants: Approximately 24 participants with at least 3 PK samples Number of Sites: 2 centers Duration of Participation: Up to 13 days Dose Schedule: Estimated Start: Estimated Finish: 3 days of intravenous acyclovir will be administered as follows: 500 mg/m2 q 8 hours for 3 days March 2011 September 2011 Specific Aim 2: To initiate our first device study entitled, Optic Nerve Sheath Diameter Ultrasound as a Measure of Hydrocephalus. PI = Dr Robert Gordon Clinical background: Hydrocephalus is a condition characterized by increased intracranial pressure and the subsequent complications that result when the brain is deformed by that pressure. Congenital hydrocephalus occurs in 1/500 live births, making it more common than Trisomy 21 with potentially more devastating consequences, such as generalized cerebral hypoperfusion, mental retardation and death. The etiology of hydrocephalus can be varied, with over 180 different reasons for hydrocephalus to develop. Intraventricular hemorrhage (IVH) is the leading cause of congenital hydrocephalus. We will use the strong association between IVH and prematurity to screen this subgroup for development of elevated intracranial pressure. Current methods for assessing hydrocephalus include cranial ultrasound, CT, MRI and monitoring of head circumference. Each method has specific draw backs, including: cost, radiation exposure, cold stress, need for specialized technicians, and varied interpretations of imaging. If there were a simple inexpensive, noninvasive bedside tool that could assess elevated intracranial pressure, it would greatly improve the management of premature infants at risk for hydrocephalus. Device Background: Ultrasound (U/S) technology uses sound waves to penetrate a medium and then record the reflective signatures of that medium to reveal an image. Its excellent safety profile and relative ease of use has found it a role in medical diagnostics for the last 50 years. Ophthalmologists employ U/S routinely in their offices to assess retinal and other posterior ocular structures. Recently there has been interest in using U/S for a new role, measuring the optic nerve sheath diameter (ONSD). Geeraerts, T. et al 1 found that OSND on T2 MRI correlates with elevated intracranial pressure. Rajajee, V. et al 2 found that ultrasonically measured ONSD was highly sensitive and specific for identifying intracranial pressure>20 mmHg. Gravendeel, J. et al 3 was first to publish normative values for ONSD measured by ultrasound (values at birth, 4 and 8 months were 3.9, 5.5, and 5.8mm respectively). Objectives: To use ONSD measured by Accutome’s B-Scan Plus U/S to establish a growth curve for premature infants to be used for assessing likelihood of hydrocephalus development. Babies born at less than 36 weeks gestational age will be followed weekly in the NICU for changes in head circumference (HC), cranial ventricular width (VW), and ONSD. Upon discharge (typically at 1-3 months of age), the infants will be monitored in the outpatient setting every 3 months until one year of age. Our target recruitment of 60 premature babies is a starting point based on projected Tulane NICU patient volume and the cohort size in the Gravendell, J et al report . 3 Following longitudinal collection of data and appropriate statistical analysis, a growth curve will be plotted for the subgroup of patients who did not develop hydrocephalus. In the hydrocephalic group we will compare ONSD, VW and HC to determine if ONSD may be an earlier and more accurate marker for elevated intracranial pressure. 1. Geeraerts T, Newcombe VF, Coles JP, et al. Use of T2-weighted magnetic resonance imaging of the optic nerve sheath to detect raised intracranial pressure. Critical care (London, England). 2008;12(5):R114. 2. Rajajee V, Vanaman M, Fletcher J, Jacobs T. Optic nerve ultrasonography is an accurate non-invasive bedside tool to detect raised ICP in the neuroicu; Institutional validation of criteria may be required. Neurocritical Care. 2010;13:S161. 3.Gravendeel J, Rosendahl K. Cerebral biometry at birth and at 4 and 8 months of age. A prospective study using US. Pediatric Radiology. 2010;40(10):1651-1656. Specific Aim 3A: to analyze, present and publish the “Aminophylline use to prevent renal dysfunction in patients with birth asphyxia undergoing whole body cooling” study – a large case series and matched cohort comparison study performed by Tulane-Lakeside and Ochsner in collaboration with the University of Virginia to investigate the safety and efficacy of aminophylline as an adjunct therapy to cooling. Co-PIs = Dr Euming Chong and Phillip Gordon. IRB waiver granted. Study Description: 17 infants were consecutively treated with whole body cooling for hypoxic ischemic encephalopathy (HIE) based on predetermined, standardized criteria at the Tulane-Lakeside and Ochsner Main Campus NICUs from 2008-2010. All but one infant received aminophylline, a therapy known to improve renal function in HIE but not to have been paired with cooling before now. One infant died. Another infant remains ventilator dependent at transfer. All other infants were discharged home on full feeds by bottle. Sarnat scores of neurologic insult revealed a median score of moderate severity in our cohort with an average initial blood gas pH of 6.96 and an average base deficit of -18.96. Substantial improvements in renal function were noted (as shown below). PRELIMINARY PRIMARY OUTCOME DATA Severe Renal Dysfunction < 0.5 ml/kg/h Moderate Renal Dysfunction < 1 ml/kg/h Acute Renal Failure creatinine > 1.5 x 2 d theophylline (pooled data*) 21/101 (21%) N/A N/A aminophylline + cooled (our study) 2/17 (12%) 6/17 (35%) 2/17 (12%) cooled (pooled data*) 128/257 (50%) 204/234 (87%) N/A cooled control (pooled data*) 144/265 (54%) 204/226 (90%) N/A theophylline control (pooled data*) 53/96 (55%) N/A N/A * Pooled data derived from 8 randomized controlled trials with available data on renal function (4 from cooling and 4 from theophylline therapy studies). References available upon request. Data Analysis: We are collaborating with the University of Virginia (UVA), where a similar whole body cooling guideline (sans aminophylline) is in use. We will do a 2 to 1 matched cohort comparison study of renal function between aminophylline treated and non-treated infants, using the UVA patients as the non treated controls. There are more than 70 cooled patients in the UVA database, allowing us to match infants by Sarnat score and initial base deficit, thereby assuring similar severities of initial renal insult. Plan: An abstract has been submitted to the Pediatric Academic Societies meeting in May 2011. We intend to publish within weeks of that presentation and to use that meeting as a forum for organizing a randomized controlled trial. The publication will be submitted by May and, as we work towards its final publication, we will organize and write our first application for an RO1 to fund the trial, (with a submission goal for the fall cycle of the NICHD). The NICU follow up clinic will be imperative for this study. Specific Aim 3B: To analyze, present and publish the “Comparison between ampicillin and gentamicin vs. piperacillin/tazobactam use in the neonatal intensive care unit” study – a multicenter study performed at Tulane-Lakeside and Wesley Medical Center (Wichita, KA) to investigate the safety and efficacy of piperacillin/tazobactam as a first choice antibiotic in the NICU. Co-PIs = Dr Euming Chong and Phillip Gordon. IRB waiver submitted. Study Description: Tulane-Lakeside and Wesley Medical Center (KA) each entered into a PDSA cycle on Jan 2010 in which they switched from ampicillin and gentamicin to piperacillin/tazobactam as a first choice antibiotic for the newborn. There were a number of reasons for this quality improvement baseddecision including increased ampicillin resistance organisms, gentamicin dosing errors and associated blood draws, gentamicin ototoxicity, gentamicin renal toxicity, and recent data demonstrating that all members of the aminoglycoside family are potent vasodilators of the ductus arteriosus. This month (Jan 2011), an IRB waiver was submitted at Tulane (and one is pending at Wesley) to perform a review of piperacillin/tazobactam versus ampicillin and gentamicin for the safety and efficacy of piperacillin/tazobactam as a first choice antibiotic. Planned Analysis and Publication: Outcomes of interest will include treatment of a patent ductus, failed hearing screens, resistant organisms, failed antibiotic therapy events, mortality, ventilator associated pneumonias, necrotizing enterocolitis, number of transfusions and cost. The NICHD neonatal rapid start trial program recently performed a pharmacokinetic analysis on piperacillin/tazobactam, facilitating our initial PDSA. The final analysis of that study is due soon. Dr Benjamin (the PI of that study) has promised us that this data will be made available to us shortly after analysis and if that pK analysis suggests an alteration in dosing, we will consider that as a potential future PDSA intervention. This study will be submitted for publication in 2011. Specific Aim 4: to re-open the Tulane-Lakeside NICU Follow Up Clinic and maintain an internal NICU database using our existing electronic medical record system that includes neurodevelopmental assessments. Background: New Orleans has two other institutions that have level III regional NICUs. One does not have a designated NICU follow up clinic (Ochsner) but has a developmental pediatrician. The other, LSU Children’s Hospital, has never reported their outcomes nationally. It serves primarily as a means of helping their patients get additional services from their hospital. There is currently no institution in the Mississippi Delta region reporting neurodevelopmental outcomes on NICU graduates. This is unfortunate for two reasons: 1) before Hurricane Katrina, Louisiana had some of the worst NICU discharge outcomes in the country (based on Vermont Oxford data).2) post Katrina, Tulane and Ochsner have both made significant strides in the quality of their NICU care. However, the nation currently remembers us as the same pre-Katrina institutions. A NICU discharge clinic that includes neurodevelopmental assessments will allow TNORC to report our current outcomes, which we believe are exemplary. It will allow us to stand out as an institution regionally. Finally, and perhaps most importantly for this application, it will allow TNORC to access prospective studies and trials that require neurodevelopmental assessment as part of their study protocol (which is the most substantial limit facing the TNORC today). Action Plan: The TNORC directors met with HCA administrators on Jan. 6th and brokered a plan for opening a NICU follow up clinic at Lakeside Hospital in mid March. HCA will handle staffing needs. TNORC and Tulane pediatrics will handle physician staffing. Approximately $5000 is needed for developmental assessment equipment (Bayley III developmental assessment scales, DPIII developmental survey, two large crawl-around carpets and computerized data entry/processing of these scores). Conclusions: This proposal demonstrates the versatility of the TNORC as a clinical research enterprise. We started it as a quality improvement venture, focusing on PDSA cycles. Two such interventions (the addition of aminophylline to whole body cooling and the switch from ampicillin & gentamicin to piperacillin/tazobactam) resulted in our first two multicenter studies. Phase I at the TNORC (2010): PDSA cycles were used to create one year quality improvement projects. Based on available literature, two global changes were made to current clinical practice at the Tulane NICU: 1) Piperacillin/tazobactam was chosen as the first choice of antibiotic instead of ampicillin & gentamicin. 2) A single dose of aminophylline was administered prior to the initiation of whole body cooling for asphyxiated infants to prevent renal dysfunction. IRB waivers were applied for prior to analysis. From a practical point of view, neither of these studies generated immediate revenue. However, the aminophylline study appears to be so dramatic in its preliminary results that we believe the clinical concept is ripe for a randomized controlled trial. We will be well positioned to write that grant and lead the study if we have sufficient infrastructure in place (namely neurodevelopmental follow up). This past year, we also successfully completed our role as a site for the NICHD sponsored fluconazole prophylaxis study. This was a low enrollment, low revenue study. We agreed to be a part of it primarily because we wanted to develop expertise and infrastructure in prospective clinical trials. This led to the offer of the Acyclovir study in 2011, (a more lucrative study). Both studies will be of lasting value to the neonatal community and thus will improve our stature nationally. Phase II at TNORC (2011): a) Evolution - Dr Robert Gordon’s device study represents one new phase of our venture. Devices, especially those which can be used in observational studies are ideal for parallel studies because they have little likelihood of introducing extraneous bias to an existing medical study. Thus this represents an excellent opportunity for us to learn how to coordinate device studies with an ongoing prospective study (such as the acyclovir study). Both studies will improve our potential to generate revenue. b) Communication / publication / advancement - The aminophylline and piperacillin/tazobactam studies are both likely to have substantial impact upon the national neonatology community when they are presented and published. TNORC represents an important incubation chamber for our junior faculty and offers a clear mechanism by which they can begin to ascend the promotion ladder. These synergies also provide the motivation and energy for future clinical studies and grant applications. c) Remediation - The re-opening of our NICU follow up clinic is perhaps the most critical goal of all for the coming year. We hope to have it open by March. Without this, substantial future funding will be denied to us and we will not be on a level footing with similar neonatal research enterprises nationally. RELEVANCE OF PROJECT TO LONG RANGE GOALS: The budget requested in this application serves as seed / bridging money for TNORC. In our conclusions section of the project summary, we outlined the first two years of TNORC’s existence (2010 and 2011). We have demonstrated in these two years, a clear vision by which a new research enterprise can transition from principally performing unfunded quality improvement research, to attracting mid level NIH funding as a non-network clinical research site (as well as industry sponsorship), to ultimately developing TNORC into what most investigators would consider an optimal funding opportunity (the principal site for NIH grants). It is perhaps worth noting that no start up money has been spent on TNORC. All the effort spent upon it thus far is due to the vision and academic motivations of its directors and participants. Now the timing is critical. There is only so much time that each intensivist can give to contracted studies (as we are attracting now), because the revenue is not sufficient to create protected time. To reach the next level, we need a mid level person to help focus and coordinate TNORC. We need dedicated equipment (computers, software, a data backup system). These things are not expensive and our current projected revenue should put us past the breakeven scenario by 2012 (after overhead is taken). Most importantly, we anticipate that future funding should eventually be on par with other center-based research enterprises at the university. This grant would be the stimulus that TNORC needs to make all of this happen. BUDGET FOR TNORC (2011): Current funds: $5,000 (after overhead) Pilot Grant Request:$50,000 $ 35,0000 TNORC employee (part time) – patient enrollment, IRB liason, data management, research $4,500 Developmental assessment tools and equipment for the NICU follow up clinic $3,500 Software for statistics, patient randomization, patient matching, Access (for building templates and auto filling datasets) for data entry and management at Lakeside $2,500 computer and miniserver for de-identified data repository at Tulane $2,500 for miscellaneous supplies to support TNORC (including books, subscriptions, etc.) $ 3,000 to Dr Robert Gordon for miscellaneous supplies to support his ONSD study. $ 4,000 for travel to PAS and other meetings to present research Total: $55,000 TIMELINE FOR COMPLETION – All 4 specific aims in this proposal will be completed by Dec 2011. BIOGRAPHICAL SKETCH CURRENT AS OF 1/10/2010 Provide the following information for the key personnel in the order listed on Form Page 2. Photocopy this page or follow this format for each person. NAME POSITION TITLE Phillip V. Gordon MD PhD Professor of Pediatrics EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, and include postdoctoral training.) INSTITUTION AND LOCATION North Carolina State University Florida State University University of Florida DEGREE (if applicable) YEAR(s) B.A. Ph.D. M.D. 1986 1992 1995 FIELD OF STUDY Psychology Molecular Biology Medicine RESEARCH AND PROFESSIONAL EXPERIENCE: Concluding with present position, list, in chronological order, previous employment, experience, and honors. Include present membership on any Federal Government public advisory committee. List, in chronological order, the titles, all authors, and complete references to all publications during the past three years and to representative earlier publications pertinent to this application. If the list of publications in the last three years exceeds two pages, select the most pertinent publications. Selected Professional Experience 2009-present Professor, Chief & Elsie Shaeffer Chair of Neonatology, Assistant Chair of Pediatrics, Tulane School of Medicine, New Orleans, LA 2009-present Associate Editor, Journal of Perinatology 2007-2009 Section Head of Neonatology, Ochsner Health System, New Orleans LA 2006-2007 Associate Professor of Neonatology, University of Virginia Health Sciences, Charlottesville VA 2004-2007 Neonatal Fellowship Director, University of Virginia Health Sciences, Charlottesville VA 2000-2006 Assistant Professor of Neonatology, University of Virginia Health Sciences, Charlottesville VA 2002-2007 Recipient NIDDK 1KO8DK/HD61553-0 Paracrine regulation of IGF-I in the developing gut 2001-2003 Recipient NIH CHRCDA HD01421The role of IGF-I in developing gut Publications by Dr Gordon in Clinical, Translation & Basic Science Research: 1. Gordon P, Rutledge J, Sawin R, Thomas S, and Woodrum D. Early postnatal dexamethasone increases the risk of focal small bowel perforation in extremely low birth weight infants. Journal of Perinatology 19: 573-577, 1999. 2. Gordon PV, Price WA, Stiles AD. Dexamethasone administration to newborn mice alters mucosal and muscular morphology in the ileum and modulates IGF-I localization. Pediatric Research 49: 93-99, 2001. 3. Gordon PV, Young ML, Marshall DD. Focal small bowel perforation: an adverse effect of early postnatal dexamethasone therapy in extremely low birth weight infants. Journal of Perinatology 21: 1-5, 2001. 4. Gordon PV, Marshall DD, Stiles AD, Price WA. The clinical, morphologic, and molecular changes in the ileum associated with early postnatal dexamethasone administration: from the baby’s bowel to the researcher’s bench. Molecular Genetics and Metabolism 72: 91-103 (and cover photo), 2001. 5. Gordon PV, Stiles AD, Price WA, Rutledge J. Early postnatal dexamethasone diminishes transforming growth factor alpha localization within the ileal muscularis externa of newborn mice and extremely low birth weight infants. Pediatric and Developmental Pathology 4: 532-537, 2001. 6. Gordon PV, Moats-Staats B, Stiles AD, Price WA. Dexamethasone changes the composition of insulin-like growth factor-binding proteins in the newborn mouse ileum. Journal of Pediatric Gastroenterology and Nutrition 35(4):532-8, 2002. 7. Guthrie SO, Gordon PV, Thomas V, Thorp JA, Peabody J, Clark RH. Necrotizing Enterocolitis in a National Neonatal Data Set. Journal of Perinatology 23(4): 278-85, 2003. 8. Gordon PV, Paxton JB, Herman A, Carlisle E, Fox NS. IGF-I accelerates ileal epithelial cell migration in culture and newborn mice and may be a mediator of steroid-induced maturation. Pediatric Research 54(5); 2004. 9. Herman A, Carlilse E, Paxton JB, Gordon PV. Insulin-like growth factor (IGF-I) regulates submucosal growth and thickness within the newborn mouse ileum. Pediatric Research 55(3); 507-13, 2004. 10. Gordon PV, Paxton JB, Kuemmerle J, Fox NS. A 14 kD cathepsin L-derived-carboxylIGFBP-2 fragment is sequestered by cultured rat ileal crypt cells. American Journal of Physiology: Gastroenterology and Liver Physiology, 2005 (Epub ahead of print). 11. Effird MM, Heerens AT, Gordon PV, Bose CL, Young D. Randomized controlled trial of hydrocortisone for prevention of hypotension in extremely low birth weight infants. Journal of Perinatology 25(2); 119-24, 2005. 12. Gordon PV, Paxton JB, Fox NS. A methodology for distinguishing divergent cell fates within a common progenitor population: adenoma- and neuroendocrine-like cells are confounders of rat ileal epithelial cell (IEC-18) culture. BMC Cell Biology 6(1):2, 2005. 13. Gordon PV, Paxton JB, Fox NS. CREG mediates glucocorticoid-induced loss of the type-2 IGF receptor in ileal epithelial cells. Journal of Endocrinology 185(2), 2005 (Epub ahead of print). 14. Gordon PV, Herman AC, Marcinkiewicz M, Gaston BM, Laubach VE, Aschner JL A neonatal mouse model of intestinal perforation: Investigating the harmful synergism between glucocorticoids and indomethacin, Journal of Pediatric Gastroenterology and Nutrition, 2007 Nov;45(5):509-19. 15. Gordon PV, Swanson JR, Attridge JT, Clark R. Emerging trends in acquired neonatal intestinal disease: is it time to abandon Bell's criteria? J Perinatol. 2007 Nov;27(11):66171. 16. Marcinkiewicz M, Gordon PV. A role for plasmin in platelet aggregation: differential regulation of IGF release from IGF-IGFBP complexes? Growth Horm IGF Res. 2008 Aug;18(4):325-34. 17. Gordon PV, Marcinkiewicz M. An analysis of IGFBP evolution.Growth Horm IGF Res. 2008 Aug;18(4):284-90. 18. Stout G, Lambert DK, Baer VL, Gordon PV, Henry E, Wiedmeier SE, Stoddard RA, Miner CA, Schmutz N, Burnett J, Christensen RD. Necrotizing enterocolitis during the first week of life: a multicentered case-control and cohort comparison study. J Perinatol. 2008 Aug;28(8):556-60. 19. Gordon PV. Understanding intestinal vulnerability to perforation in the extremely low birth weight infant. Pediatr Res. 2009 Feb;65(2):138-44. BIOGRAPHICAL SKETCH CURRENT AS OF 1/10/2010 Provide the following information for the key personnel in the order listed on Form Page 2. Photocopy this page or follow this format for each person. NAME POSITION TITLE Euming Chong, MD Assistant Professor of Pediatrics EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, and include postdoctoral training.) INSTITUTION AND LOCATION University of Western Ontario, Canada Wayne State University, Michigan Thomas Jefferson University Hospital DEGREE (if applicable) MD YEAR(s) 2002 2002-2005 2005-2008 FIELD OF STUDY Medicine Pediatrics Neonatology RESEARCH AND PROFESSIONAL EXPERIENCE: Concluding with present position, list, in chronological order, previous employment, experience, and honors. Include present membership on any Federal Government public advisory committee. List, in chronological order, the titles, all authors, and complete references to all publications during the past three years and to representative earlier publications pertinent to this application. If the list of publications in the last three years exceeds two pages, select the most pertinent publications. Selected Professional Experience 2008 – present Assistant Professor of Pediatrics, Tulane University Academic & Clinical Educator/Attending for the Pediatric Residency Tulane University 07/2006 – 06/2008 Thomas Jefferson University Hospital, Philadelphia, PA Neonatal-Perinatal Chief Fellow 07/2005 – 06/2008 Thomas Jefferson University Hospital, Philadelphia, PA Neonatal-Perinatal Fellowship Program 07/2002 – 06/2005 Children’s Hospital of Michigan, Detroit, MI Pediatric Residency Program 04/2000 – 05/2002 University of Western Ontario Faculty of Medicine, London, ON Doctor of Medicine 04/1997 – 09/1999 International Medical University, Kuala Lumpur, Malaysia Diploma of Advanced Medical Science Pre-clinical years prior to transfer to University of Western Ontario Publications by Dr. Chong in Clinical, Translation & Basic Science Research: 1. Chong E, Greenspan J, Kirkby S, Culhane J, Dysart K. Changing Use of Surfactant Over 6 Years and Its Relationship to Chronic Lung Disease. Pediatrics 2008; 122(4):e917-21 2. Chong E, Locke R, Dysart K, Chidekel A, Shaffer T, Miller T. Heat Shock Protein 70 Secretion by Tracheal Tissue during Mechanical Ventilation: Association with Indices of Tissue Functioning and Modeling. Pediatric Research 2009; 65(4):387-91 3. Dola C, Tran T, Linhuber AM, Cierny J, Denicola N, Chong E, Bhuiyan A. Preterm Birth After Mature Fetal Lung Indices: Is There Any Neonatal Morbidity? Journal of Maternal –Fetal and Neonatal Medicine 2010; May Early Online e1-6 PMID: 20459338 BIOGRAPHICAL SKETCH CURRENT AS OF 1/9/2010 Provide the following information for the key personnel in the order listed on Form Page 2. Photocopy this page or follow this format for each person. NAME POSITION TITLE Jane E. Reynolds , MD Associate Professor of Pediatrics EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, and include postdoctoral training.) DEGREE INSTITUTION AND LOCATION YEAR(s) FIELD OF STUDY (if applicable) Hunter College in the Bronx, City University of NY BA 1964-1968 Women’s Medical College of PA MD 1968-1972 Albert Einstein Medical Center, Philadelphia, PA 1972-1973 Thomas Jefferson University Hospital, Philadelphia, PA 1973-1975 Medicine Pediatrics RESEARCH AND PROFESSIONAL EXPERIENCE: Concluding with present position, list, in chronological order, previous Hospital of the Albert Einstein College of Medicine/ 1975-1977 Neonatology employment, experience, and honors. Include present membership on any Federal Government public advisory committee. List, in chronological order, the titles, all NY authors, and complete references to all publications during the past three years and to Bronx Municipal Hospital, representative earlier publications pertinent to this application. If the list of publications in the last three years exceeds two pages, select the most pertinent publications. Selected Professional Experience 1978-1984 Assistant Professor of Pediatrics 1984-Present Associate Professor of Pediatrics Tulane University School of Medicine (LA) 1984-2010 Neonatal Attending MCLNO-University Hospital (LA) 1978-1993 Neonatal Attending Charity Hospital of Louisiana 1985-1997 Consulting Neonatologist Slidell Memorial Hospital (LA) 1977-1978 Clinical Instructor & Neonatal Attending Hospital of the Albert Einstein College of Medicine (NY) 1977-1978 Consulting Neonatologist New Rochelle Hospital and Medical Center (NY) Publications by Dr. Reynolds in Clinical Research: 1. Hot Topics 2000 In Neonatology, December 2000, “Early Postnatal Dexamethasone Therapy for the Prevention of Chronic Lung Disease” for the Vermont Oxford Steroid Study Group, Roger F. Soll, MD, Pediatrics, 2001 Sept;108(3):741-8. 2. Hot Topics 2000 In Neonatology, December 2000, “Neonatal Skin Care Study: The Effect of Aquaphor Original Emollient Ointment on Nosocomial Sepsis Rates and Skin Integrity in Infants of Birth Weight 501 to 1000 Grams” for the Vermont Oxford Group. (In Press) 3. Eidelman, AI and Reynolds, J: Gentamycin Resistant Klebsiella Infections in a Neonatal Intensive Care Unit. Am Jour Dis Chil 4:132, April, 1978. 4. Dunn, DW and Reynolds, J: Neonatal Withdrawal Symptoms Associated with “T’s and Blues” (Pentazocine and Triplennamine). Am Jour Dis Chil, 136:644-645, July, 1992. 5. Contributions to Practical manual of Pediatrics, 2nd edition. Waring, WW, Jeansonne, LO, et al. CV Mosby Co., 1992. 6. Reynolds, JE, Pernoll, ML, Gill, WL, Nadell, J, Frost, A, Mabie, W: Hydrocephalus: A Case of Ventricular-Amniotic Shunting. Southern Med J 78(2):203, Feb, 1985. 7. Reynolds, JE, Pernoll, ML, Mabie, W, Nadell, J, Gill, WL: Direct Fetal Therapy: The Multidisciplinary Team Concept, Southern Med J 78(6):661-664, June, 1985. 8. Cryotherapy for Retinopathy of Prematurity Cooperative Group: Multicenter Trial of Cryotherapy for Retinopathy of Prematurity. Pediatrics 81:679-706, 1988. BIOGRAPHICAL SKETCH Provide the following information for the Senior/key personnel and other significant contributors. Follow this format for each person. DO NOT EXCEED FOUR PAGES. NAME POSITION TITLE Gordon, Robert Allen Associate Professor of Clinical Ophthalmology and Pediatrics eRA COMMONS USER NAME (credential, e.g., agency login) rgordon EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, include postdoctoral training and residency training if applicable.) DEGREE INSTITUTION AND LOCATION MM/YY FIELD OF STUDY (if applicable) Tulane University(New Orleans, La) Tulane Medical School (New Orleans, La) Baylor University Medical School (Houston, Tx) Tulane University Medical Center (New Orleans, La) Indiana University Medical Center (Indianapolis, Ind) B.S. M.D. Internship 1965 1969 1970 Residency 1970-1973 Fellowship 1976 Chemistry Medicine Rotating internship Ophthalmology Pediatric Ophthalmology Please refer to the application instructions in order to complete sections A, B, C, and D of the Biographical Sketch. A. Personal Statement Optic nerve sheath diameter (ONSD) has been shown to directly correlate with the level of ICP. Since there are only a few reported studies on ONSD measurements in babies, and none on preemies, the main goal of this study is to develop a normative database of ONSD in premature babies as measured by noninvasive ophthalmic ultrasound. A secondary goal is to measure ONSD in preemies who develop hydrocephalus before and after ventriculoperitoneal shunts.Since joining the faculty in 1973, my interest in ophthalmic signs and symptoms of pediatric systemic diseases, including prematurity, has exponentially expanded during my role as Director of the Tulane Pediatric Ophthalmology and Strabismus service. Although my research interests have mainly focused on preventing lifetime blindness from Retinopathy of Prematurity (25 years as principal investigator for NIH sponsored clinical trials), I have frequently struggled to help my pediatric colleagues diagnose increased intracranial pressure (IICP) or hydrocephalus in infants and children. In older children and adults, IICP is classically reflected on ocular fundus examination by noting papilledema of the optic nerve head. Unfortunately, in infants and very young children papilledema is usually not present or too difficult to confirm as an outpatient due to poor patient cooperation. Specifically, since premature infants, babies and children less than 2-3 years of age do not manifest papilledema when they develop IICP, clearly new noninvasive diagnostic techniques in addition to measuring head circumferences and performing brain ultrasound should be explored to improve early detection of hydrocephalus in this fragile population. B. Selected Positions and Honors Positions and Employment 1975-present Director, Pediatric Ophthalmology and Strabismus, Tulane University Health Sciences Center Other Experience and Professional Memberships 1990-present Member, American Association Pediatric Ophthalmology & Strabismus, 1976-present Fellow, American Academy of Ophthalmology Honors and Awards 2005-2010 “Best Doctors in New Orleans”-Pediatric Ophthalmology 2006 National Eye Institute-NIH, ETROP Inspiration Award 1994-1996 Pediatric Consultant, Ophthalmic Device Section, (Intraocular Lenses), Federal Drug Administration Honor Award,American Academy of Ophthalmology “Composite Drawing of Retinopathy of Prematurity Stages & Zones”, Published in Neonatal Ophthalmology Slide Set, Produced & distributed by Wyeth International Laboratories, Copyright 1992 C. Selected Peer-reviewed Publications Publications Most Relevant to the Current Application Additional Recent Publications of Importance to the Field 1. *The Early Treatment for Retinopathy of Prematurity Cooperative Group. Authors/Group Information: The members of the writing Committee and the Early Treatment for Retinopathy of Prematurity (ETROP) Study Investigators are listed on pages E7 and E8. Gordon RA (Page 7), “Final Visual Acuity Results in the Early Treatment for Retinopathy of Prematurity Study,” Arch Ophthalmol. 2010; 128(6) (doi:10.1001/archophthalmol.2010.72). 2. Systematic Review of Digital Imaging Screening Strategies for Retinopathy of Prematurity. Robert A. Gordon, et al. Letter to Editor, Pediatrics 2009; 123(2) pp. e360-3361, (doi: 10.1542/peds.2008-3579). 3. VanderVeen DK, Coats DK, Dobson V, Fredrick D, Gordon RA, et al. Prevalence and course of strabismus in the first year of life for infants with prethreshold retinopathy of prematurity: findings from the Early Treatment for Retinopathy of Prematurity study. Arch Ophthalmol 2006 Jun; 124(6):766-73 4. Early Treatment of ROP Cooperative Group, “Revised Indications for the Treatment of Retinopathy of Prematurity: Results of the Early Treatment for Retinopathy of Prematurity Randomized Trial,” Archives of Ophthalmology; 12/2003, 121 1684-1696. 5. Cryotherapy for ROP Cooperative Group”, Multicenter Trial of Cryotherapy for ROP: Natural History ROP: Ocular Outcome of 5 ½ years in Premature Infants with Birth Weight Less Than 1251g”, Archives of Ophthalmology; 5/2002, 120(5)595-599. Gordon RA, Principal Investigator, Tulane CRYO-ROP Center) D. Selected Research Support Recently Completed Research Support Principal Investigator, NIH-sponsored ROP clinical trials: 2002-2009 Principal Investigator, Phase II ETROP Follow-up study, NEI 2000-2005 Principal Investigator, CRYO-ROP Follow-up study, NEI 2000-2005 Principal Investigator, "Early Treatment Study for ROP (ETROP)”, NEI Participating Center 2000-2001 Principal Investigator, "Phase III CRYO-ROP Outcome Study Center.” 1994-1998 Principal Investigator, "Phase III CRYO-ROP Outcome Study Center”, National Eye Institute Grant # 2U10 EY06358 08 1993-1999 Principal Investigator, "STOP-ROP" (Supplemental Oxygen for Pre-threshold ROP) NEI/NIH Center 1989-1994 Principal Investigator, “Phase II CRYO-ROP Outcome Study Center,” National Eye Institute Grant # 2401EY06358-05 1985-1989 “A Multicenter Trial of Cryoablation for Retinopathy of Prematurity”, Gordon RA, Principal Investigator for Participating Center, NEI Grant # 1U01EY06358-01 ($372,000) BIOGRAPHICAL SKETCH as of 1/12/2011 Provide the following information for the Senior/key personnel and other significant contributors. Follow this format for each person. DO NOT EXCEED FOUR PAGES. POSITION TITLE NAME David G. Cupp, MD Ophthalmology Resident (PGY3) EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, include postdoctoral training and residency training if applicable.) DEGREE INSTITUTION AND LOCATION YEAR(s) FIELD OF STUDY (if applicable) University of California San Diego (La Jolla, CA) Penn State College of Medicine (Hershey, PA) Wilson Medical Center (Johnson City, NY) Tulane University (New Orleans, LA) B.S. M.D. Intern Resident 1997-2001 2008 2008-2009 2009-present Physics-Biophysics/PreMed Medicine Transitional Year Ophthalmology Selected Professional Experience 2001-2004 2005-2007 Biophysics Researcher. Torrey Pines Institute of Molecular Science (San Diego, CA). Research Assistant. Retina Research Group-Penn State College of Medicine (Hershey, PA). Peer Reviewed Publications and Poster 1. Cupp, DG. Kampf, PJ. Kleinfeld, AM. Fatty Acid-Albumin Complexes and the Determination of the Transport of Long Chain Free Fatty Acids across Membranes. Biochemistry, 4473-4481, 2004. 2. Kampf, PJ. Cupp, DG. Kleinfeld, AM. Different mechanisms of free fatty acid flip-flop and dissociation revealed by temperature and molecular species dependence of transport across lipid vesicles. J. Biol. Chemistry, 21566-21574, 2006. 3. Alan M. Kleinfeld, David Cupp, J. Patrick Kampf. Flip-flop is Rate Limiting for Transport of Long Chain Free Fatty Acids across Small and Large Unilamellar Lipid Vesicles. Poster presented at 48th Annual Biophysical Socitey Meeting; Baltimore, MD, 2004.