Pollution Prevention in Waste Management

Pollution Prevention in
Waste Management
Vanna Liu
2013 Sustainability Intern
Solid and Hazardous Waste Education Center
University of Wisconsin Extension
The University of Wisconsin Extension’s Solid and Hazardous Waste Education Center (SHWEC) provided a student intern and staff assistance to identify useful changes that reduce waste, emissions and/or hazards, to increase efficiency at this host facility. However, the host facility decides whether to implement suggestions based, among other things, its own evaluation of the project, including its own evaluation of the work performed by the intern under the facility’s supervision. The host facility accepted the services “as is” and without warranty, including expressly without warrant of merchantability or warranty of fitness for a particular purpose.
NOT FOR DISTRIBUTION
Preface
This report will serve as a summary of my findings at Meriter Hospital as a 2013 Sustainability Intern with the Solid and Hazardous Waste Education Center. Pollution prevention was the main objective of this internship. While there are many paths to pollution prevention, my time at Meriter was spent in the waste management route.
I have had the pleasure of working with many professionals who have made this internship very worthwhile. First, I would like to thank Steve Brachman and Marlene Jaglinski, for making this internship a possibility and providing such a great service to the community. Secondly, I would like to thank my faculty advisors Barb Bickford and Joe Van Rossum, who I constantly sought advice from. Finally, a big thank you to all the folks at Meriter, especially to Kim Wilson and Kari Gust for all the time we spent auditing and tireless explanations of policies, to Alice Butler for all the guidance she has shown throughout the process, and to John Eisenhauer for my acceptance into this hospital and all the wisdom
I have gained from our talks.
2
Table of Contents
Preface…………………………………………………………………………………………………….……. 2
Table of Contents…………………………………………….………………………………………..…… 3
Background……………………………………………………………….…………………………..………. 4
Baselines Review…………………….…………………………………………….………………………. 5-6
Pharmaceutical Waste Audit…………………………………………….……………………………. 7-10
Blue Wrap Recycling..………………………………………….………………………………….…..… 11-12
Community Collection Program…………………………………………….……….……………… 13
Greenhouse Gas Reduction…….…………………………………………….……………………….. 14
Appendix….…………………………………………….……………………………………………………… 15-17
3
Background
Meriter Hospital is a 448 bed not-for-profit hospital located in Madison, WI. Five wings in the hospital house more than nineteen patient units, and are currently operating at an average 6200 patient days per month. The Hospital is the flagship facility of Meriter Health Group, which consists of Meriter
Laboratories, Home Health, Foundation and Clinics. For the purposes of this report, “Meriter” will refer to Meriter Hospital.
The principle “first do no harm” is adhered to readily at Meriter and their sustainability mission comes as a result. With ongoing renovations and new construction, Meriter constantly evaluates projects on environmental impact. The 2011 Eco-Efficiency Initiative of the Year award was given to the hospital by
INBusiness Magazine following projects on water conservation and energy reductions. In waste management, the hospital has implemented many industry Best Management Practices and go far beyond in some areas.
Contact Information:
Meriter Hospital
202 S. Park Street,
Madison, WI 53715 http://www.meriter.com/
(608)417-6000
4
Baseline Review
Purpose
A baseline review is generally the first step in waste reduction. It is necessary for a facility to quantify the amount of waste it generates in order to set reduction targets and determine where to start. While all waste streams were recorded in some form, there were many inconsistencies, like units of measure, which make it difficult to organize. The goal of this review was to create a single unified spreadsheet where all waste streams are measured under one metric.
Results
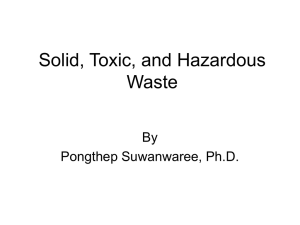
29 waste streams beginning January 1, 2012 have been quantified in pounds per month. All 29 waste streams are captured in Figure 1 in their respective categories, shown in Table 1.
Table 1. Categories of waste and their waste streams
Waste Category Waste Streams
Solid waste
C&D (bulk MSW)
General MSW
Construction-Trash
C&D (bulk recycling) Construction-Recycled
RMW Medical Waste, Pathological Waste
Hazardous waste
Pharmaceuticals
Recycling
Aerosols, Botox, Dual, RCRA Haz pharmaceuticals
Non-haz pharmaceuticals
Amalgam, Amalgam Separator, Appliances, Ballasts, Batteries, Bulbs, Cardboard,
Commingled, Electronic, Kitchen Grease, Mercury, Parts wash, Photo Fixer, Scrap metal, Shredded Paper, Surgical Equipment, Surgical Instruments, Toner Cartridges,
Used oil
Non-hazardous pharmaceuticals,
15.44, 1.31%
Hazardous waste;
3,75; 0,32%
RMW; 67,56; 5,73%
Recycling; 302,27;
25,65%
Solid waste, 636.85,
54.03%
C&D (bulk recycling); 109,38;
9,28%
C&D (bulk MSW);
43,35; 3,68%
Figure 1. Categorical pie chart of waste generated in tons for the year 2012 by Meriter Hospital
5
Based on the “Target-Setting Guidelines for Common Health Care Waste Categories” from the
Sustainability Roadmap for Hospitals, American Hospital Association (AHA), Meriter is performing
“basic” in solid waste, municipal solid waste (MSW) from construction and demotion (C&D), and recycling (Table 2). The hospital is “intermediate” in regulated medical waste (RMW) and “advanced” in
C&D recycling, hazardous waste and pharmaceutical waste. See Appendix for more figures.
Table 2. Classification of waste generation performance by Sustainability Roadmap for Hospitals, AHA
CATEGORY
Solid waste
C&D (bulk MSW)
C&D (bulk recycling)
Hazardous waste
Recycling
BASIC INTERMEDIATE ADVANCED MERITER CLASSIFICATION
57.% 51.4% 45.7% 54.03% BASIC
5%
0%
Regulated medical waste 13.5%
4%
Non-haz Pharmaceuticals 0.50%
20%
3%
2%
9%
3%
0.6%
30%
0%
5%
5%
2.5%
0.8%
40%
3.68% BASIC
9.28% ADVANCED
5.73% INTERMEDIATE
0.32% ADVANCED
1.31% ADVANCED
25.65% BASIC
Recommendations
Table 3 lists recommendations for long-term target percentages of waste. These are long term goals because while a 3.3% change in solid waste does not sound like much, it requires a diversion 39 tons or
78,000 pounds of waste if total waste remains constant. A 4.35% increase in recycling has been recommended to reach the “intermediate” performance benchmark. While 51 tons is a reach, there are items currently being disposed of as MSW with high recycling potential. At this point, it is not economical for some materials since technology is still in development (for example, organic food waste). It is expected that costs of recycling will decrease as newer and more cost effective options become available. Meriter is currently disposing of pharmaceuticals at a level higher than the
“advanced” benchmark. This was investigated in the Pharmaceutical Waste Audit (See next page).
Because contactors dispose of C&D waste, no target changes are listed for C&D MSW and C&D recycling.
Table 3. Target percentages of total waste and changes in tons to reach target
CATEGORY
Solid waste
C&D (bulk MSW)
C&D (bulk recycling)
RMW
Hazardous waste
Non-haz Pharmaceuticals
Recycling
MERITER
54.03%
3.68%
9.28%
5.73%
0.32%
1.31%
25.65%
TARGET
50.72%
No Change
No Change
5.00%
No Change
1.00%
30.00%
CHANGE IN TONS
-39.03
0.00
0.00
-8.63
0.00
-3.65
51.31
Limitations
Furniture recycling and donations have not been included in this study as weights diverted have not been recorded. Pharmaceutical returns were not captured because it is not waste by WDNR .
6
Pharmaceutical Waste Audit
Purpose
Non-hazardous pharmaceuticals represent 1.31% of Meriter’s total waste generated in 2012. Table 2 shows that a higher percentage of pharmaceutical waste is an indicator of more advanced performance.
The standard for “advanced” performance is 0.8%, which Meriter is higher than by 0.5%. This difference amounts to 6.01 tons or 12,022 pounds of non-hazardous pharmaceutical waste per year.
(1.31% − 0.8%) Nonhaz Pharm
⁄
Total Waste
∗ 1178.6 tons Total Waste = 6.01 tons Nonhaz Pharm
Generally, only 5% of all pharmaceutical waste is hazardous by Resource Conservation and Recovery Act
(RCRA), while 11% is recognized as BMP hazardous, and 84% non-hazardous. From the Baselines Review, it was determined that 20% of Meriter’s pharmaceutical waste stream was hazardous, 4% greater than the industry’s highest BMP standard. The difference between disposing a pharmaceutical as hazardous versus non-hazardous waste is $9.54 per pound, which using values from 2012, would equates to
$14,641.
(20% − 16%) Haz Pharm
⁄
Total Pharm
∗ 19.19 tons Total Pharm = 0.768 tons Haz Pharm
− $0.03 lb Nonhaz ) = $14,641
In the beginning, there were two main objectives of the pharmaceutical waste audit:
To determine whether items were being wasted in the non-hazardous pharmaceutical (bluewhite) containers that did not belong
To determine what areas required further education in proper pharmaceutical waste disposal
Results
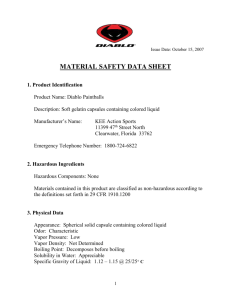
31 non-hazardous pharmaceutical waste containers were analyzed within a 4-week period, accounting for all units that Meriter Hospital manages waste for, which excludes UW labs and clinics.
Biohazardous,
31.3lbs,
10% Trash or Sewer,
74.3lbs
25%
Hazardous,
58.7lbs,
20%
Non-hazardous,
136.5lbs
45%
BMP
92%
RCRA
8%
Figure 2. Summary of results from audit of non-hazardous pharmaceutical waste containers (7/19-
8/7/13), shown in percentages of total weight at left and percentages of “Hazardous” items at right
7
25% by weight of all items found in the blue-white containers could have been drained in the sink or potentially trashed. Plain intravenous (IV) fluids such as sodium chloride, lactated ringers, calcium glutonate, etc. can be drained in a sink for treatment by the municipal wastewater treatment plant.
Empty containers and IV bags with protected health information (PHI) were considered potential trash because these items could be disposed of in general trash if PHI was removed. Other items found in the trash include: gloves, cups, wipes, and packaging.
10% of the weight measured was considered biohazardous under Meriter policy. It is estimated that at least 90% of the biohazardous material were syringes without needles. Furthermore, these were often empty syringes that once held plain fluids or non-hazardous pharmaceuticals.
45% by weight was correctly placed in this receptacle.
20% of the total weight was considered hazardous by Meriter practices, defined as RCRA hazardous,
BMP hazardous or an empty container of either. When looking at the itemized results, only 8% (32/380) of the hazardous material was actually RCRA regulated. The other 92% (348/380) were classified as BMP hazardous.
Utilizing waste data from 2012, the cost of correction under current Meriter policy is shown in Table 4.
Table 4. Cost of correction using equivalent weights from 2012 baseline
Disposal Method
Biohazardous
Hazardous
General MSW
Equivalent
Weight (lb)
3216
6027
7624
Recommendations
Cost/Pound
0.4
9.84
0.024
Cost
1286
59284
185
Difference from
Current Cost
-322
-57476
2102
Distribute educational material
25% of waste found in the non-hazardous pharmaceutical waste containers was divertible into sewer or MSW. This is equivalent to 7624 pounds of material incinerated per year and saving $2100 if all were disposed of in MSW and landfilled instead. Most of this weight can be attributed to plain intravenous fluids which can be drained. In addition, many empty containers that previously held nonhazardous medication were also found in these containers. By policy, these containers can go in MSW if
PHI was removed.
Educational material was created for each unit detailing what items found during the audit could be trashed.
Pictures taken during the audit process were used. Figure
3 is an example of the poster generated.
Black markers or dense black stamps should also be more
Figure 3. Example of educational material generated from audit data for each unit
8
conveniently available for nurses to use to render PHI illegible. A trash audit reveals that nurses may recognize that IV bags can be disposed of in general MSW. However, the extra step of PHI removal presents an inconvenience to the user. Further research is needed to determine which method of PHI removal is preferred and most cost effective.
Discontinue handling syringes without needles as sharps
WDNR regulations define sharps as “medical equipment that may cause punctures or cuts.” 1 Syringes without needles are dull and do not possess potential in puncturing, thus these items are not classified as sharps. Sharps are a type of biohazardous waste, which requires special handling and disposal. At
Meriter, biohazardous waste is sent to be shredded, microwaved then landfilled by a local vendor. Thus, this method of disposal is energy consuming and not cost effective for items not regulated as biohazardous waste.
By extrapolating data from audit and using 2012 values, 2894 pounds of syringes without needles were disposed of in non-hazardous pharmaceutical waste containers. This is using an estimate of 90% syringes without needles in the biohazardous waste found. Table 5 lists the costs associated with disposing syringes without needles found in the non-hazardous pharmaceutical container audit.
Table 5. Cost of various disposal methods for 2894 pounds of syringes without needles
Disposal Method
Biohazardous
Pharmaceutical
General MSW
Cost/Pound Cost
0.4 1157.70
0.3 868.28
0.024 70.06
The disposal of syringes without needles as sharps is an unnecessary expense by the hospital. If syringes without needles are handled as normal containers, they will be disposed of as pharmaceutical waste if containing medication or general MSW if empty. Both options are much more cost effective, as shown in table 5. These costs were calculated for the 2894 pounds of syringes without needles estimated that are currently disposed of in the non-hazardous pharmaceutical waste container. While it was not possible to audit sharps containers themselves, it is expected that many syringes without needles are disposed of in those red containers by Meriter policy. Therefore, savings are predicted to be much higher when taking into account the diversion of syringes without needles from sharps containers.
Currently, Meriter’s MSW vendor will not accept syringes of any kind on the basis that workers have a natural aversion to anything that appear medical and otherwise dangerous. Syringes diverted to MSW will be both empty and not attached to a needle. Because they are empty, no medication will leach out and contaminate the landfill or surrounding waste. Without a needle, the syringes are dull-ended and do not present a danger to workers. A way to compromise would be single-streaming the syringes and labeling the containers, which informs workers of the container’s contents. Otherwise, it may be advisable to search for another vendor that will take this stream, especially one capable of recycling syringes.
1 Wisconsin Department of Natural Resources, “PUB-WA 820 2007: Medical Waste: Definitions of Terms.” 2007.
Accessed 23 Aug 2013.
9
Dispose empty BMP hazardous containers in MSW
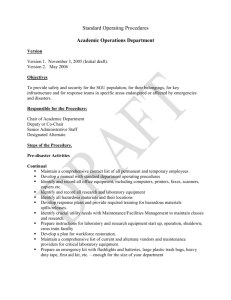
The only empty containers regulated by the EPA and WDNR are those of RCRA P-listed chemicals.
Among Meriter’s entire formulary, only 17 items out of 2474 are P-listed, with either nicotine or warfarin as active ingredient. 828 items are classified as BMP hazardous, excluding RCRA and P-listed.
Figure 4 shows the organization of pharmaceutical waste classification; BMP hazardous theoretically encompasses RCRA, which contains P-listed chemicals. Currently, all empty containers of BMP hazardous medications are disposed of in the hazardous pharmaceutical bin, for which is only required for P-listed pharmaceuticals.
Empty containers are costly to dispose of, especially for hazardous pharmaceuticals. Whereas all other disposal costs are dependent on weight,
“black” container disposal is charged per container, thus dependent on volume.
An 8 gallon “black” drum costs $149 to dispose of. (The average cost per pound is $9.84. A pound of general MSW costs
$0.02 to dispose of.) Empty containers take up a lot of space, which is of concern especially for this disposal
Figure 4. Organization of pharmaceutical waste classification scenario.
According to the audit, only 8%, 32/380, of the hazardous pharmaceuticals erroneously disposed of in the non-hazardous pharmaceutical waste receptacle were RCRA hazardous (Figure 2). 4/32 of these items are P-listed. The other 92% of hazardous waste were BMP hazardous excluding RCRA. Disposal of all 380 BMP hazardous items in
“black” is estimated at $60,000.
Because it was not possible to perform a RCRA hazardous waste audit, we do not know what percentage of “black” waste are empty BMP hazardous containers. However, all medication is contained in some sort of packaging, whether it be IV bags, bottles, syringes or foil wrappers. All this packaging of hazardous pharmaceutical under current policy is disposed of in “black.”
10
Blue Wrap Recycling
Purpose
A previous blue wrap recycling pilot a few years ago was unsuccessful due to conflicting compactor usage and transportation costs. The same compactor used for general MSW was used for compacting blue wrap. Large amounts would need to be collected and stored before clearing the compactor for blue wrap compacting. Kimberly-Clark, who initiated the program, also pulled their support from it.
Eventually, the transportation costs began to outweigh the benefits of recycling blue wrap.
Results
About 10,000 sheets of blue wrap are purchased monthly for use in the operating room (OR). This generates about 2,700 pounds of general MSW for the hospital.
Table 6. Average pounds of blue wrap purchased a month
Width (in) Length (in) Thickness (in) Sheets/month Volume/month (cf) Pounds/Month
54
45
54
36
18
30
24
48
Total
54
45
72
36
18
30
24
48
0.03
0.03
0.03
0.03
0.03
0.03
0.03
0.03
480
2064
648
936
864
2160
2400
384
9936
25
76
46
22
5
35
25
16
250
270
806.25
486
234
54
375
267
171
2663
Recommendations
After discussing blue wrap with several people in the sustainable healthcare community, it became evident that there were three options for reduction and recycling: purchase hard cases, pelletizing by a vendor and repurposing into totes. It is recommended that a combination of these methods are used.
Purchase hard cases
The OR and Supply, Processing and Distribution (SPD) unit estimate a 50% potential in reduction by purchasing hard cases, reducing 8 tons of blue wrap yearly. This process is already underway, with Phase
I complete.
Haul for pelletizing
A vendor in the area has offered to take our loose blue wrap at no cost to the hospital. The only condition was that the blue wrap has to be clean and uncontaminated. He also had another proposal for collection: purchase their manual baler for $1295 and receive $0.05 per pound of baled blue wrap. With half of blue wrap potentially eliminated by hard cases, collecting and baling the other 50% would yield a
20 month payback period.
÷ 2) ∗ $0.05 lb
11
However, this does not include labor costs and assumes 100% capture. Table 7 shows the payback period according to percent capture.
Table 7. Payback periods calculated by percent blue wrap captured out of total blue wrap purchased
Capture
70%
80%
90%
100%
Tons collected Payback Period
(months)
5.59
6.39
7.19
7.99
27.79
24.32
21.62
19.45
Repurpose into reusable totes
Two organizations are interested in sewing reusable totes with the blue wrap generated: Meriter volunteers and the Dane County Retired and Senior Volunteer Program. It is estimated that Meriter will be able to divert 5% to repurposing per month.
12
Community Collection Program
Purpose
This program would provide a “green” service for the wider Meriter community. There have been internal collection drives for cell phones in the past, but they were event-based. A collection program would have this recycling service available continually.
Recommendations
TerraCycle’s Brigade Program
TerraCycle has many different brigade programs collecting widely used items for recycling. Meriter has been signed up for two: the Cell Phone Brigade as well as the Writing Instruments Brigade. The hospital is able to monetarily benefit from TerraCycle’s program because of its not-for-profit status. Table 8 shows the return Meriter is able to receive for each item collected. TerraCycle repurposes these items into products they then sell through their website.
Table 8. TerraCycle’s Brigade Program
Item
Writing instrument
Standard Cell Phone
Smart Phone iPhone
Return
$0.02
$1.00
$7.50
$10.00
Lions International Eyeglass Recycling
Lions Madison is willing to collaborate with Meriter to collect used eyeglasses. They currently run a program with the Madison schools where every child needing glasses are provided a pair free of charge if unable to afford them.
13
Greenhouse Gas Reduction
The following values for metric tons of carbon dioxide equivalent (MTCO2E) reduced were calculated using the EPA’s Waste Reduction Model (WARM).
Baselines Review
Waste targets (diversion to recycling) – 137 MTCO2E
Pharmaceutical Waste Audit
Distribute educational material to remove trash – 5 MTCO2E
Discontinue handling syringes without needles as sharps – 2 MTCO2E
Dispose empty BMP hazardous containers in general MSW – 2 MTCO2E
Blue Wrap Recycling
Purchase hard cases – 13 MTCO2E
Haul for pelletizing – Recycling PP N/A on WARM
Repurpose into reusable totes – 0 MTCO2E
14
Appendix
Baseline Spreadsheet for Jan 2012-Dec 2012
Waste
Electronic
Surgical Instruments
Construction-Recycled
Construction-Trash
Toner Cartridges
Ballasts
Bulbs
Medical Waste
Pathological Waste
General
Shredded Paper
Commingled
Cardboard
Scrap metal
Appliances
Amalgum
Parts wash
Photo Fixer
Used oil
Kitchen Grease
Amalgum Separator
Batteries
Non-haz pharmaceuticals
RCRA Haz pharmaceuticals
Dual
Botox
Aerosols
Mercury
Surgical Equipment
Total Waste
Vendor
Cascade
Centurion
Findorff
Findorff
Kids for Cash
Lamp Recyclers
Lamp Recyclers
MERI
MERI
Pellitteri
Pellitteri
0
5.98
0
54.21
7.8
Pellitteri
Pellitteri
2.9
11.41
Pellitteri 1.13
Roxane Stillman's Salvage Recycling N/A
Safety Kleen 0
Jan-12
2.198
Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12
1.404
1.126
0 5.071
0.36
2.822
Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Total 2012
0 0.3085
3.3395
0 0.727
17.356
0.093753 0.093753 0.093753 0.093753 0.093753 0.093753 0.093753 0.093753 0.093753 0.093753 0.093753 0.093753
1.125036
45.22
20.26
0 0 0 0 0 0 15.29
17.87
7.55
3.19
109.38
15.81
0.049
0
6.36
0.19755
0.349
0
0.1342
0
0
0.1025
0.0625
0
0.15225
0.0535
0
0.1062
0
0
0.1333
0.146
0
0.14435
0
5.35
0.1862
0.09
7.26
0.1188
0
4.01
0.1568
0.193
4.56
0.1216
0
43.35
1.60275
0.894
0.13688
0
5.52
6.05
0.0135
0
49.01
58.82
8.1
2.9
11.34
1.65
N/A
0
8.02
2.9
12.43
1.02
N/A
0
0.134714 0.158299 0
5.02
5.57
5.48
0
49.04
7.05
2.9
9.94
0.31
N/A
0
0.0125
54.62
9.07
2.9
10.91
0.72
N/A
0
0
55.58
7.57
2.9
11.25
1
N/A
0
0.124502 0
5.37
6.40
0
53.73
7.72
2.9
10.22
0.9
N/A
0
0.0075
58.03
8.4
2.9
11.83
0.44
N/A
0
0.128093 0
5.10
0
47.56
7.72
2.9
10.44
0.08
N/A
0.0075
6.07
0
53.56
8.55
2.9
11.96
1.41
N/A
0
0.119054 0
5.55
5.42
0
52.02
7.57
2.9
11.08
0.77
N/A
0
0
50.67
6.15
2.9
10.75
0.3
N/A
0
0.80154139
67.529
0.0335
636.85
93.72
34.8
133.56
9.73
N/A
0.0075
Safety Kleen
Safety Kleen
Safety Kleen
Sani Max USA
Solmetex
Stericycle Specialty Waste
Stericycle Specialty Waste
Stericycle Specialty Waste
Stericycle Specialty Waste
Stericycle Specialty Waste
Stericycle Specialty Waste
Stericycle Specialty Waste
Stryker Surgical
0
0
0
0
0
0.175
0.0035
0
0.916
0.1975
0.0365
0
0
0
0
0.225
0
0
1.91
0.5025
0.18
0.0685
0
0
0.0025
0
0.009
0
0
0.375
0
0.2085
0.832
0.048
0
0.012
0.0025
0
0
0.15
0.0035
0
0.983
0.1605
0.035
0
0
0
0
0
0
0.2
0
0 0 0.2675
1.9725
0.9765
1.6395
0.4505
0.192
0.062
0
0.005
0
0
0
0.0025
0
0.01
0
0
0.034
0
0
0
0
0.25
0.0035
0.3045
0.049
0
0.0025
0
0
0
0
0.3625
0.125
0 0.0035
0.25
0
0 0.5955
0
0.9705
1.868
0.825
0.162
0.062
0
0
0
0
0.015
0
0.0025
0
0
0.3315
0.1395
0.1055
0.0255
0.0055
0
0
0
0
0
0
0.015
0
0.1225
0.0875
2.3225
0 0.004
0.018
0.239
1.556
0.3085
0.1695
3.0985
0.063
0
0
0
0
0
0
0
0.987
0.042
0
0
0
0.0075
0.049
0
1.3105
15.436
0.631
0.0055
0.0195
0.0025
0.413417 0.413417 0.413417 0.413417 0.413417 0.413417 0.413417 0.413417 0.413417 0.413417 0.413417 0.413417
4.961
148.55
110.45
92.67
76.40
92.44
85.97
87.09
90.22
98.71
114.79
94.73
86.58
1178.60083
Benchmarking
60,00%
50,00%
40,00%
30,00%
20,00%
10,00%
0,00%
BASIC
INTERMEDIATE
ADVANCED
MERITER
15
Pharmaceutical Waste Audit Spreadsheet
Drug
Acetaminophen/Codeine
Acyclovir
Adenosine
Advair discus
Aerosol Inhaler
Albumin
Albuterol sulfate
Alprazolam
Aluminum Can
Aminophylline
Amiodarone
Ampicillin
Atropine
Bacteriostatic
Beneprotein
Bicarbonate
Bismatrol
Bivalirudin
Bivalirudin
Bloody Gauze
Brevibolac
Brinzolamide
Bupivacaine
Buprenorphine
Caffeine
Calcium Chloride
Calcium Glutonate
Photos from Audit
Cefepime
Cefotetan
Ceftaroline
Ceftriaxone
Cefuroxine
Ciprofloxacin
Cleocin
Clindamycin
Culture vial
Cup
Cup-Pill
Cytomegalovirus immune
Daptomycin
Dexmedetomidine
Dextrose
Diatrizoate
Diatrizoate meglumine
1A-ED satellite1E-Soiled 1E-Med Room2E-Endoscopy3C-Pharmacy 3N-Inpatient Rehab 3T-Medical Imaging
1
1
5
7
1
1 1
1
2
5
1
1
1
6
1
1
1
1
4
12
2
1
2
2
1
4
1
2
3
15
5
2
2
16
Blue Wrap Bag
17