Participation Health Screening Questionnaire

Name:_____________________________ PeopleSoft #:________________ Date:__________ 1
UConn Student Health Services Activity Preparticipation Screening Questionnaire
Answer the following as honestly as possible:
Assess your Health Status by marking all true statements:
History: You have had:
Yes No a heart attack Yes No heart valve disease
Yes No heart surgery
Yes No cardiac catherization
Yes No coronary angioplasty (PTCA)
Yes No pacemaker/implantable cardiac defib/rhythm disturbance
Yes No heart failure
Yes No heart transplantation
Yes No congenital heart disease
Symptoms:
Yes No You experience chest discomfort with exertion
Yes No You experience unreasonable breathlessness
Yes No You experience dizziness, fainting, or blackouts
Yes No You experience ankle swelling
Yes No You experience unpleasant awareness of a forceful or rapid heart rate
Yes No You take heart medications
Other health issues:
Yes No You have diabetes
Yes No You have asthma or lung disease
Yes No You have burning or cramping sensation in your lower legs when walking short distances
Yes No You have musculoskeletal problems that limit your physical activity
Yes No You have concerns about the safety of exercise
Yes No You take prescription medications
Yes No You are pregnant
Comments:________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Name:_____________________________ PeopleSoft #:________________ Date:__________ 2
Cardiovascular risk factors
Yes No You are a man >45 years
Yes No You are a woman > 55 years
Yes No You smoke or quite smoking within the previous 6 months
Yes No Your blood pressure is > 140/90 mmHg OR You do not know your blood pressure OR You take blood pressure medication
Yes No Your blood cholesterol level is > 200 mg/dL (or LDL is > 130 mg/dL or HDL blood cholesterol is < 40 mg/dL) OR You do not know your cholesterol level
Yes No You have a close blood relative who died suddenly before the age of 50
Yes No You are physically inactive (i.e. you get < 30 min of moderate intensity physical activity on at least 3 days of week for past 3 months)[exercise at 40 – 60 % of your maximal intensity]
Yes No You have a body mass index > 30 kg/m 2
Yes No You have prediabetes (fasting blood glucose > 100 mg/dL on two different occasions) OR You do not know if you have prediabetes
Yes No Your HDL > 60 mg/dL (Subtract one risk factor)
Yes No Have you ever had an injury or pain that has interfered with your ability to exercise? Explain.
__________________________________________________________________________________________________
_________________________________________________________________________________________________
I have read, understood and completed this questionnaire as honestly as possible. Any questions I had were answered to my full satisfaction.
Date:________________________ Name:_______________________________________________
Signature:_____________________________________________
PAC Use Only
______
Total number of positive cardiovascular risk factors
PAC initials/date:
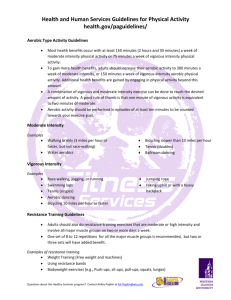
______ 0 - 1 indicates Low Risk: client can begin moderate or vigorous intensity exercise without consulting physician or other appropriate health care provider
______ > 2 indicates: Moderate Risk
______can begin low to moderate intensity exercise (40 – <60% VO
2
R; 3 - < 6 METs)
“An intensity that causes noticeable increases in HR and breathing.” i.e. walking at a moderate or brisk pace of 3 – 4.5 mph (15 – 20 minute/mile), level bicycling, yoga, weight training
______CANNOT begin vigorous intensity exercise (>60% VO
2
R; > 6 METs) without medical exam and clinician approval
“An intensity that causes substantial increases in HR and breathing” i.e. jogging or running, step aerobics, jumping rope, basketball game, soccer
* Modified from AHA/ACSM Health/Fitness Facility Preparticipation Screening Questionnaire. ACSM’s Guidelines for Exercise Testing
and Prescription , 9 th Edition, 2014. Lippincott Williams and Wilkins http://www.lww.com.
Name:_____________________________ PeopleSoft #:________________ Date:__________ 3
Physical Activity Questionnaire
1.
What physical activities do you engage in on a regular basis?
____________________________________________________________________________________
____________________________________________________________________________________
2.
If you walk, run or jog, what is the average number of miles you cover each workout? _________miles
3.
If you participate in resistance training, which type of exercises do you perform? (Check all that apply.)
Free weights
Machines
Therabands
Calisthenics (push-ups, pull-ups, etc.)
Core training
Please provide specifics (crunches, sit-ups, planks, etc. and repetitions/time performed):
______________________________________________________________________________
______________________________________________________________________________
4.
How many minutes, in average, is each or your exercise workouts?____________________minutes
5.
How many workouts do you participate in on average each week?____________________ workouts
6.
Check those activities that you would prefer in a regular exercise program for yourself:
Walking, running, jogging
Elliptical
Swimming
Handball, racquet ball, squash
Stationary cycling
Basketball
Bicycling
Spinning
Aerobic dance/zumba
Stairmaster
Resistance Training
Yoga/Pilates
Free weights
Other (Specify)_____________________________________
Stretching
Machines
7.
What are YOUR physical activity goals?
Improve Health
General Fitness
Lose weight
Build Muscle Mass
Aerobic Fitness
Tone
Strengthen Core
Improve Balance
Improve Flexibility
Improve fitness knowledge
Other (Specify)_______________________________________________
Improve Strength
8.
What are YOUR greatest obstacles to regular exercise?
Time
Motivation
Money
Enjoyment
Pain
Lack of knowledge
Other (Specify)________________________________________________