File - Melinda McMillen
advertisement

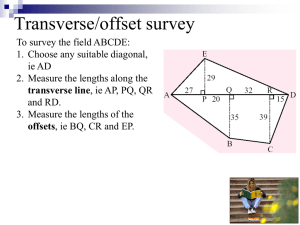
Radial Tunnel Syndrome at the Elbow Melinda McMillen: Jordan Utley & Jenn Ostrowski Section 1 Introduction to the Pathology Incidence of the Pathology Radial tunnel syndrome (RTS) is cause by pressure on the radial nerve either by repetitive motions of the wrist/elbow or by a direct blow to the elbow. Activities that may increase the risk for developing RTS are: Contact sports such as soccer, rugby or football Inadequate warm-up before practice or play Diabetes mellitus Hypothyroidism (underactive thyroid gland) Occupations, such as an assembly line, where the hands are used frequently to do fine movements (Radial Tunnel Syndrome (radial [posterior interosseous] nerve, 2010)). Etiology Radial tunnel syndrome can be causes by multiple factors. One of the more common mechanisms of injury is if the radial tunnel is too small for any reason and then the puts pressure on the nerve and it can become pinched and cause pain. Constant use of the arm and repetitive motion of the elbow and wrist such as twisting, gripping, pushing and pulling can stretch and irritate the nerve even more. Another common form of injury is from a direct blow to the lateral side of the arm/elbow (Klein). <Photo 1: Etiology> Section 2 Anatomy & Physiology of the injury Anatomy The radial nerve starts at the lateral side of the neck where the individual nerve roots from the brachial plexus exit the spine through the neural foramina. The radial nerve is one of three main nerves that run down the arm to the hand. The nerve travels down the posterior side of the upper arm and runs along the lateral side of the elbow this is where the nerve passes into the radial tunnel, formed by muscles and bone. Passing through the tunnel the radial nerve runs below the supinator muscle. This is where is splits off into the superficial and deep branches (Radial Tunnel Syndrome, 2006). <Photo 2: Anatomy> <Photo 3: nerve pathways> Physiology Radial tunnel syndrome can be causes by two different mechanisms: a specific, acute incident like a direct blow to the elbow or a more chronic onset brought about by repetitive motions. The radial nerve branches spread to the back of the forearm. RTS occurs when this nerve is compressed as it passes through the radial tunnel near the elbow. With repetitive motions the radial nerve can become stretched or irritated from overuse (Is It Tennis Elbow or Radial Tunnel?, 2011). “With humeral fractures, the radial nerve is damaged 12 percent of the time (Starkey, Brown, Ryan, 2010).” Section 3 Evaluation of the injury Signs and Symptoms Symptoms of radial tunnel syndrome are located distally on the forearm and may be reproduced with resisted supination of the hand and resisted extension of the middle finger (Starkey, Brown, Ryan, 2010). Patient reports of tenderness and pain over the radial tunnel and weakness in the muscles on the back of the forearm and wrist especially with gripping activities and pain with twisting motions of the hand (Radial Tunnel Syndrome (radial [posterior interosseous] nerve). 2010) Special Tests: Defining Practice Evaluation Radial tunnel syndrome can be evaluated through Tinnel’s Sign. This special test is performed by bending the elbow and tapping on the radial nerve between the olecranon and the lateral epicondyle. A positive sign will reproduce pain and/or results in a burning sensation in the hand (Starkey, Brown, Ryan, 2010). <Video 1: Tinnel Sign> Double Click to play Palpation tenderness over the wrist extensor is also indicative of RTS (Neal, Sara L., MD, MA, Fields, Karl B, MD,. 2010). <Photo 4: extensor muscles palpation> Section 4 Associated Differential Diagnoses Radial tunnel syndrome closely resembles lateral epicondylalgia also known as tennis elbow. Distinguishing between the two can be very difficult because physical examination maneuvers that aggravate RTS are usually also positive on a patient with lateral epicondylalgia. The most effective factor to differentiate between the two pathologies is the point of maximal tenderness. “ In radial tunnel syndrome, this point is over the anterior radial neck; in tennis elbow, it is at the origin of the extensor carpi radialis brevis muscle” (Neal, Sara L., MD, MA, Fields, Karl B, MD,. 2010). <Photo 5: differential diagnosis> Section 5 Prognosis & Recent Evidence Informing Best Clinical Care Prognosis If treated properly, then the symptoms of radial tunnel syndrome typically resolve and decrease over time. “It is hard to give a specific time period or percentage of outcomes due to variations in outcome measures, the severities of RTS and the inconsistencies in duration, type of intervention, and follow up time for interventions.” Rarely, surgery is necessary to free the compressed nerve (Standard of Care: Radial Tunnel Syndrome, 2007). Resent Research After modifying the activity of a patient presenting with RTS another form of management being recently utilized is injections. Typically used to relieve pain is a local anesthetic and a corticosteroid. “In 1 study of 25 patients with RTS, 18 patients (72%) had resolution of their symptoms with a single injection of 2 mL 1% lidocaine and 40 mg of triamcinolone in 1 mL of carrier at 6 weeks of follow-up and 16 patients continued to have long-term pain relief at greater than 2 years”. A point of controversy in management of RTS relief is the use of surgery to decompress the radial nerve; opinions differ from surgeon to surgeon. Although there are any reports and individual case studies supporting the efficacy of surgical intervention there has been no randomized controlled trial that compares surgical with non-surgical treatment or with a placebo. For more information of these above topics see article below. Dang, A.C., MD, Rodner, C.M., MD. (2009). Unusual Compression Neuropathies of the Forearm, Part I: Radial Nerve. Retrieved June 1, 2013, from http://musculoskeletalinstituteofnewengland.org/clinical_services/orthopaedic/han dwrist/pdfs/article_radialnerve.pdf REFERENCES Dang, A.C., MD, Rodner, C.M., MD. (2009). Unusual Compression Neuropathies of the Forearm, Part I: Radial Nerve. Retrieved June 1, 2013, from http://musculoskeletalinstituteofnewengland.org/clinical_services/orthopaedic/han dwrist/pdfs/article_radialnerve.pdf Is It Tennis Elbow or Radial Tunnel?. (2011). APEX Network Physical Therapy. Retrieved May 31, 2013, from http://www.apexnetworkpt.com/2011/08/it-tennis-elbow-or-radial-tunnel Klein, David M, MD. Kennedy-White Orthopaedic Center. Retrieved May 31, 2013 from, http://www.kwoc.net/radial%20tunnel%20syndrome.pdf Neal, Sara L., MD, MA, Fields, Karl B, MD,. (2010). Peripheral Nerve Entrapment and Injury in the Upper Extremity. American Family Physician 15;81(2):147-155. Retrieved from http://www.aafp.org/afp/2010/0115/p147.html Radial tunnel Syndrome. (2006). Orthogate. Retrieved June 1, 2013 from, http://www.orthogate.org/patient-education/elbow/radial-tunnel-syndrome.html Radial Tunnel Syndrome (radial [posterior interosseous] nerve). 2010. Washington Orthopeadics and Sports Medicine. Retrieved June 1, 2013 from, http://www.wosm.com/index.php/component/content/article/121-radial-tunnelsyndrome-radial-posterior-interosseous-nerve Standard of Care: Radial Tunnel Syndrome. (2007). The Brigham and Women’s Hospital, Department of Rehabilitation Services. Retrieved June 1, 2013, from http://www.brighamandwomens.org/Patients_Visitors/pcs/rehabilitationservices/P hysical%20Therapy%20Standards%20of%20Care%20and%20Protocols/ElbowRadial%20Tunnel%20Syndrome.pdf Starkey, C., Brown, S., Ryan, J. (2010). Examination of Orthopedic and Athletic Injuries (3rd ed.). Philidelphia, PA: F.A. Davis Company.