Consultation-Draft-National-Patient-Contact-Protocol-for
advertisement

DRAFT National patient contact protocol for patients with Implanted Medical
Devices subject to Hazard Alerts
Version 1.0
i
Contents
PURPOSE OF THIS PROTOCOL ................................................................................................................. 1
PART 1 – PRELIMINARY ISSUES ............................................................................................................... 2
A.
Introduction ........................................................................................................... 2
B.
Hazard Alerts ......................................................................................................... 4
C.
Scope of the Protocol ............................................................................................ 6
D.
Stages of the Protocol ........................................................................................... 7
E.
The role of State/Territory Recall Co-ordinators................................................... 8
PART 2 – PREPARATION .......................................................................................................................... 9
F.
Adopting a Hazard Alert Management Policy ....................................................... 9
G.
Appointing persons responsible ............................................................................ 9
H.
Establishing a Hazard Alert Committee ............................................................... 10
I.
Managing implanted device data ........................................................................ 10
Collecting implanted device data ........................................................................ 10
Documenting and testing data retrieval processes ............................................. 12
J.
Registering with Health Professional Online Services ......................................... 12
K.
Identifying Hazard Alerts ..................................................................................... 12
PART 3 – RESPONSE .............................................................................................................................. 13
L.
Managing a Hazard Alert ..................................................................................... 13
Initiating the Healthcare Organisation’s response .............................................. 13
Planning for patient contact ................................................................................ 13
Identifying affected patients ............................................................................... 14
Contacting patients ............................................................................................. 15
Following up patients unable to be contacted .................................................... 15
Responding to inquiries ....................................................................................... 16
Maintaining appropriate records ........................................................................ 16
PART 4 – RECOVERY .............................................................................................................................. 17
M.
Evaluating and reporting management and outcomes ....................................... 17
N.
Supporting system level accountability............................................................... 18
DICTIONARY .......................................................................................................................................... 19
ii
COMMISSION SPONSOR
Professor Debora Picone AM
PROGRAM DIRECTOR
Mr Neville Board, Director, Information Strategy and Safety in eHealth
AUTHOR
Dr Heather Wellington, DLA Piper
Version control (Document Revision History)
Version
Date
Comment
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
1.0
18 December 2013
20 December 2013
23 December 2013
28 January 2014
9 April 2014
5 May 2014
21 May 2014
10 June 2014
30 June 2014
Dr Wellington
Comments N.Wilcox, T.Snioch
Revisions incorporated
Revisions incorporated
Jurisdictional, Executive and private hospital sector feedback
Minor revisions
Revised following Recall Co-ordinator workshop 16 May 2014
Revised following proof of concept
Revised following DOH comments
Distribution
Date Issued
Issued To
0.1 – 18 December 2013
0.3 – 23 December 2013
0.4 – 28 January 2014
0.5 – 10 April 2014
0.6 – 7 May 2014
0.6 – 9 May 2014
1.0 23 June May 2014
1.0 10 July 2014
1.0 24 July 2014
Project group
DRAFT submitted to Dept of Health
ACSQHC Inter-Jurisdictional Committee
Commission Executive review
Hospitals participating in the Proof of concept phase
Jurisdictional Recall Co-ordinators, , Dept of Health
Commission Executive
ACSQHC Inter-Jurisdictional Committee
ACSQHC Board
This is a managed document. For identification of amendments each page contains a version number
and a page number. Changes will only be issued as complete replacements covered by a release
notice. This document has not been released for use until authorised by the last signatory.
Authorised for release:
…………………………………………………………………………………………. (___/___/___)
Professor Debora Picone, AM
iii
PURPOSE OF THIS PROTOCOL
The purpose of the National patient contact protocol for patients with Implanted Medical Devices
subject to Hazard Alerts ('Protocol') is to enhance the ability of healthcare providers to quickly
contact patients in the event of serious safety concerns about Implanted Medical Devices. The
Protocol was endorsed by Health Minsters in [month] 2014 for use in all public and private settings
in the Australian health care system in which medical devices are implanted in patients, including
hospitals, day procedure centres and professional consulting suites.
This Protocol defines the procedures that should be implemented when Implanted Medical Devices
are subject to Class I or Class II Hazard Alerts.
The Protocol is supported by a Guide to implementing the National Patient Contact Protocol.
1
PART 1 – PRELIMINARY ISSUES
A.
Introduction
The Australian Government, through the Department of Health and in consultation with State and
Territory health authorities and the private healthcare sector, has developed this Protocol for
application by Healthcare Organisations when Implanted Medical Devices are subject to Hazard
Alerts.
The Protocol applies to all public and private settings in the Australian health care system in which
Medical Devices are implanted in patients, including hospitals, day procedure centres and
professional consulting suites.
The Uniform Recall Procedure for Therapeutic Goods (‘URPTG’), which is the result of an agreement
between the therapeutic goods industry and the Commonwealth and State/Territory health
authorities, defines the actions to be taken by health authorities and sponsors when therapeutic
goods for use in humans, for reasons relating to their quality, safety or efficacy, are to be removed
from supply or use, or subject to corrective action. The URPTG does not, however, specify how
patients with Implanted Medical Devices should be contacted when those devices are subject to
Hazard Alerts.
In its reports: The Regulatory Standards for Approval of Medical Devices in Australia1 and The Role of
the Therapeutic Goods Administration Regarding Medical Devices, Particularly Poly Implant
Prostheses (‘PIP’) Implants2, the Senate Community Affairs Reference Committee noted significant
deficiencies in arrangements for contacting patients in these circumstances.
This Protocol defines the procedures that should be implemented in all public and private hospitals,
day procedure centres and professional consulting suites in the Australian health care system when
Medical Devices that have been implanted in patients in those settings are subject to Class I or Class
II Hazard Alerts3.
The Protocol is based on the following principle:
Contacting individuals with Implanted Medical Devices that are subject to Hazard Alerts, and
providing them with appropriate information and access to necessary services is:
a.
b.
c.
d.
a patient and consumer right;
a core responsibility of the healthcare system;
a normal part of an episode of care should the unexpected occur; and
a critical element of clinical communications.
1
The Senate Community Affairs Reference Committee. The regulatory standards for the approval of medical
devices in Australia. November 2011.
2
The Senate Community Affairs Reference Committee. The role of the Therapeutic Goods Administration
regarding medical devices, particularly Poly Implant Prostheses (PIP) Implants. May 2012.
3
Class I Hazard Alerts are issued when product defects are potentially life-threatening or could cause a serious
risk to health. Class II Hazard Alerts are issued when product defects could cause an illness or mistreatment.
2
The Protocol:
complements the URPTG;
has a consumer focus;
will support reliable, sensitive and timely contact with patients with Implanted Medical
Devices that are subject to Hazard Alerts;
reflects opinions as to ‘best practice’ expressed by stakeholders who participated in a
consultation process; and
supports good governance at an organisational and system level.
The Protocol defines management and governance responsibilities for Healthcare Organisations
consistent with those defined in standard 1 of the National Safety and Quality Health Service
(‘NSQHS’) Standards. The primary aims of the NSQHS Standards are to protect the public from harm
and to improve the quality of health service provision. Standard 1 requires Healthcare Organisations
to implement integrated systems of governance to actively manage patient safety and quality risks.
The Protocol is accompanied by an implementation guide: Guide to implementing the National
Patient Contact Protocol.
Important notice
This Protocol does not limit, affect or alter the obligations or duties in respect of Implantable
Medical Devices imposed on any person by or under any contract, common law or legislation.
To the extent that this Protocol is or may be inconsistent with anything in the URPTG or the
Australian Regulatory Guidelines for Medical Devices, the URPTG and those Regulatory Guidelines
shall take precedence.
3
B.
Hazard Alerts
Therapeutic goods including Implantable Medical Devices may be recalled when, for reasons relating
to their quality4, safety or efficacy, they are to be removed from supply or use, or subject to
corrective action. Recalls of therapeutic goods are governed by Section 23 of the Australian
Regulatory Guidelines for Medical Devices and are implemented in accordance with the URPTG. A
Hazard Alert, which is a type of Recall subject to the URPTG, is the issuing of precautionary
information about an Implanted Medical Device. Problems with device safety that lead to Hazard
Alerts are initially identified by reports referred to sponsors and/or the Therapeutic Goods
Administration ('TGA') from a variety of sources including patients, clinicians, Healthcare
Organisations, clinical quality registers, device manufacturers, Commonwealth and State/Territory
testing laboratories and other bodies.
Recalls (including Hazard Alerts) are defined according to the following European classification
system:
a.
b.
c.
Class I Recalls occur when products are potentially life-threatening or could cause a
serious risk to health.
Class II Recalls occur when product defects could cause illness or mistreatment, but are
not Class I.
Class III Recalls occur when product defects may not pose a significant hazard to health,
but withdrawal may be initiated for other reasons.
The level to which a Recall (including a Hazard Alert) action is undertaken is based on the
significance of the risk and the channels through which the goods have been distributed. The Recall
levels are:
a.
b.
c.
d.
Wholesale - includes wholesalers and state/territory purchasing authorities.
Hospital - includes nursing homes and institutions, hospital pharmacists, ambulance
services, blood and tissue banks and laboratories as well as wholesale as appropriate.
Retail - includes retail pharmacists, medical, dental and other healthcare professionals as
well as wholesale and hospital as appropriate.
Consumer - includes patients and consumers, as well as wholesale, hospital and retail
levels as appropriate.
Device Sponsors are primarily responsible for implementing Recalls (including Hazard Alerts). Most
Recalls are initiated by Sponsors in consultation with the TGA. Overall responsibility for coordinating
Recalls lies with the Australian (Commonwealth) Recall Co-ordinator, who is an officer of the TGA.
The agreement of the Australian Recall Co-ordinator is required before Sponsors implement any
recall strategies. Each State and Territory health authority also nominates an officer, and some also
nominate a deputy, through whom information relating to Recalls is channelled and coordinated.
Once a Hazard Alert has been initiated, the TGA notifies a number of key stakeholders including
State and Territory health authorities. The TGA has a standard operating procedure to alert the
Commonwealth Chief Medical Officer (‘CMO’), State and Territory Chief Health Officers (‘CHOs’) and
professional organisations (as appropriate) of certain Recall actions.
4
That is, compliance with statutory or agreed standards.
4
The URPTG requires Sponsors to notify defined individuals and organisations about Hazard Alerts in
an agreed written format, but does not define a specific requirement for Sponsors, Healthcare
Organisations or clinicians to ensure patients with Implanted Medical Devices are contacted
regarding Hazard Alerts. Nor does it provide for verification of the success of efforts to contact
patients. If the depth of a device Recall is to consumer level and consumers cannot be identified,
Sponsors are required to insert advertisements in the daily print media of each State/Territory in
which distribution has possibly taken place.
Following receipt of a Hazard Alert, public hospitals currently assume responsibility for contacting
patients with the relevant Implanted Medical Devices, but some have reported considerable
difficulty retrieving the necessary patient identification and contact information.
Co-ordinating and accounting for patient contact has also been challenging in some circumstances.
In the private sector practices vary. Some private Healthcare Organisations assume responsibility for
identifying patients in whom devices subject to a Hazard Alert have been implanted, but many rely
on the visiting medical officers who implanted the relevant devices in their private patients to
identify and contact those patients. Across both the public and private sectors, governance
arrangements and the effectiveness of patient contact efforts vary considerably.
This Protocol defines the procedures that should be implemented to ensure reliable, sensitive and
timely patient contact and to establish appropriate organisational governance of Hazard Alerts.
5
C.
Scope of the Protocol
The Protocol defines ‘best practice’ arrangements for the management and governance of Class I
and Class II Hazard Alerts, for implementation in all public and private settings in the Australian
healthcare system in which Medical Devices are implanted in patients, including hospitals, day
procedure centres and professional consulting suites.
Specifically, the Protocol defines arrangements for:
collecting and storing information necessary for the future identification of patients who
undergo implantation of medical devices;
retrieving information necessary to identify and contact patients with relevant Implanted
Medical Devices when Hazard Alerts are issued;
contacting and advising patients (both public or private) with Implanted Medical Devices
that are subject to Hazard Alerts;
evaluating the outcomes of patient identification and contact efforts; and
reporting to State/Territory Recall Co-ordinators.
The Protocol notes the role of State/Territory Recall Co-ordinators in supporting the management of
Hazard Alerts and assumes that State/Territory Recall Co-ordinators and/or CHOs may provide
Healthcare Organisations in their jurisdictions with nationally consistent information about the
appropriate timelines for patient contact, together with template information that they can provide
to patients. The Protocol does not, however, address the processes for producing such information
or communicating it to Healthcare Organisations. The Protocol also does not address:
responsibility for provision of and/or payment for healthcare services required by patients
with Implanted Medical Devices that are subject to Hazard Alerts; or
ownership and/or disposition of Implanted Medical Devices following their explantation.
6
D.
Stages of the Protocol
The Protocol complements the URPTG. The URPTG is divided into seven stages and the Protocol is
divided into four parts – preliminary issues, preparation, response and recovery (Figure 1).
Figure 1: Stages of URPTG and Patient Contact Protocol
URPTG
recall
stage
Protocol
part /
stage
Procedure
Responsibility
Protocol
section
1
Notification to the Co-ordinator Crisis Management
Sponsor
N/A
2
Information required to assess Recall
Sponsor
N/A
3
Assessment of Recall
Sponsor and Australian
Recall Co-ordinator
N/A
4
Recall
Sponsor
N/A
Sponsor
N/A
May include recall letters, paid advertisements in the
daily print media and media releases as approved by
the TGA
5
Notification to the Federal Minister responsible for
Consumer Affairs
PART 1 - PRELIMINARY ISSUES
1
Introduction
N/A
A
2
Hazard Alerts
N/A
B
3
Scope of the Protocol
N/A
C
4
Stages of the Protocol
N/A
D
5
The role of State/Territory Recall Co-ordinators
State/Territory health
authorities
E
PART 2 – PREPARATION
6
Adopting a Hazard Alert management policy
Healthcare Organisation
F
7
Appointing persons responsible
Healthcare Organisation
G
8
Establishing a Hazard Alert Committee
Healthcare Organisation
H
9
Managing implanted device data
Healthcare Organisation
I
10
Identifying Hazard Alerts
Healthcare Organisation,
clinicians and others
J
Healthcare Organisation
and relevant clinicians
K
PART 3 – RESPONSE
11
Implementing the Hazard Alert management
system
PART 4 – RECOVERY
12
Evaluating and reporting outcomes
Healthcare Organisation
and relevant clinicians
L
13
Supporting system level accountability
Healthcare Organisation
M
Sponsor
N/A
Australian Recall Coordinator
N/A
6
Progress of Recall and report
7
Follow-up action
7
E.
The role of State/Territory Recall Co-ordinators
The URPTG defines three specific responsibilities for State/Territory Recall Co-ordinators, as follows:
1.
Passing on product problem reports and recall action information to the Australian Recall
Co-ordinator.
a.
Any problem which has been reported to a State/Territory Recall Co-ordinator is
to be notified to the Australian Recall Co-ordinator without delay. Advice from
sponsors should be referred to the Australian Recall Co-ordinator.
b.
Failures of goods found by State/Territory health authorities in testing for State
Government tenders are to be notified to the Australian Recall Co-ordinator.
c.
State/Territory Recall Co-ordinators are to provide details of recalls to other
relevant organisations in the State/Territory.
Maintaining a current Rapid Alert System to communicate in an emergency, urgent safety
related information to all public and private hospitals.
Assisting in the timely provision of critical recalls information to pharmacists and other
professional groups.
2.
3.
This Protocol does not create new responsibilities for State/Territory Recall Co-ordinators. It
recognises, however, that subject to local arrangements each State and Territory Recall Co-ordinator
may assume, in addition to the responsibilities defined in the URPTG and listed above, co-ordinating
and/or governance responsibilities, which may include:
maintaining an up-to-date contact lists of Hazard Alert Co-ordinators in their jurisdiction;
ensuring the TGA has access to that list;
when a Hazard Alert is issued:
o contacting Hazard Alert Co-ordinators in their jurisdiction to determine the number
of patients potentially affected;
o supporting Hazard Alert Co-ordinators to access up-to-date information from the
TGA, the Supplier, the CMO, the CHO and other relevant sources;
o ensuring Hazard Alert Co-ordinators have access to agreed national advice on:
the information that should be provided to patients;
the timeframes within which patients should be contacted;
o monitoring the effectiveness of management of the Hazard Alert;
o creating a central point in the jurisdiction for communication about management of
the Hazard Alert;
o reporting outcomes of management of the Hazard Alert locally and nationally in
accordance with agreed protocols; and
supporting Healthcare Organisations and Hazard Alert Co-ordinators to take a continuous
quality improvement approach to the management of Hazard Alerts.
8
PART 2 – PREPARATION
F.
Adopting a Hazard Alert Management Policy
1.
The Healthcare Organisation should issue a policy (‘Hazard Alert Management Policy’)
confirming its intent to adopt this Protocol and its approach to implementation.
G.
Appointing persons responsible
2.
The Healthcare Organisation should:
a.
nominate a position or individual with responsibility for co-ordinating the
management of Hazard Alerts (the Hazard Alert Co-ordinator) in each
Healthcare Facility, and ensure they have appropriate delegated authority to
undertake the responsibilities detailed in this Protocol;
b.
nominate an alternative position or individual to assume responsibility for
co-ordinating the management of Hazard Alerts in the event the Hazard Alert
Co-ordinator is unavailable;
c.
define and promulgate the role and responsibilities of the Hazard Alert
Co-ordinator; and
d.
nominate the position or individual who is responsible for generating a patient
contact list in the event of a Hazard Alert, and a second position or individual to
assume delegated responsibility for list generation in the event that the
responsible person is unavailable.
The Hazard Alert Co-ordinator and their alternative should be:
a.
senior medical, nursing or allied health professionals; or
b.
senior managers with appropriate access to relevant clinical advice.
Depending on local arrangements, the persons nominated as responsible for generating
patient contact lists in accordance with clause 2.d. may but will not necessarily be the
Hazard Alert Co-ordinator and their alternative.
In accordance with jurisdictional protocols, the Healthcare Organisation should notify its
relevant jurisdictional contacts and/or State/Territory Recall Co-ordinators of:
a.
the names and contact details of nominated Hazard Alert Co-ordinators and
their alternatives; and
b.
any changes to those details immediately they occur.
3.
4.
5.
9
H.
Establishing a Hazard Alert Committee
6.
The Healthcare Organisation should establish a committee (‘Hazard Alert Committee’) to
advise the Hazard Alert Co-ordinator on the management of Hazard Alerts.
The chairperson of the Hazard Alert Committee should be a member of the Healthcare
Organisation’s senior management team.
7.
I.
Managing implanted device data
Collecting implanted device data
8.
9.
10.
11.
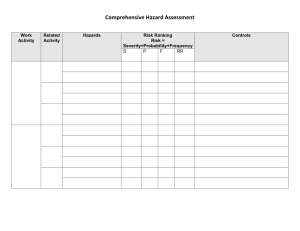
The Healthcare Organisation, with the support of clinicians, should:
a.
develop and implement procedures to ensure the data described in Table 1 are
collected and accurately recorded in patient medical records for all episodes of
care in which an Implantable Medical Device is implanted or explanted;
b.
make all reasonable efforts to:
i.
record standardised data, as described in Table 1, in searchable
electronic systems (e.g. patient administration/management system,
theatre management system or other searchable database); and
ii.
maintain the currency of those data over time;
c.
in accordance with its obligations under privacy law, inform patients, when the
relevant data are collected, that they may be stored, used or disclosed for the
purpose of effecting patient contact in the event of a Hazard Alert;
d.
advise patients with Implanted Medical Devices that they should always inform
the Healthcare Organisation and Medicare Australia, in writing and in a timely
manner, of any changes to their permanent contact details; and
e.
include device-identifying data in patient-held discharge summaries and
discharge information sent to patients’ general practitioners and, if applicable,
other referring clinicians.
For additional patient contact options, the Healthcare Organisation may choose to collect
the email addresses and mobile telephone numbers, where available, of each patient in
whom an Implantable Medical Device has been implanted.
The Healthcare Organisation should retain the data described in Table 1 in an accessible
format and location for all patients with Implanted Medical Devices for the minimum
statutory retention period following device explantation or patient death, but should
thereafter destroy or permanently de-identify data if no longer required for any purpose.
If data referred to in Table 1 are recorded in patients’ medical records and/or other
location(s) but are not stored in a searchable format, the Healthcare Organisation may
establish a systematic process to retrieve those data and record them in a searchable
format.
10
Table 1: Data items to be held by Healthcare Organisations
Data item
Fields and format(s)
Person identifier (NHDD5)
Name
First name – alphanumeric (an)
Family name – (an)
Middle name – (an)
Medicare number + individual reference number
Numeric (10)
Individual reference No (1)
Healthcare Facility medical or unit record number
Numeric
Patient date of birth
DD/MM/YYYY
Gender
M or F
Patient address at the date and time of implant (updated as
relevant during subsequent contacts with the Healthcare
Organisation)
Address details
Where the patient is a child or an incompetent adult, the
name and address of the patient’s substitute decision-maker.
Address details
(Street/unit number, Street,
Suburb/town, State, Postcode)
(Street/unit number, Street,
Suburb/town, State, Postcode)
Device identifier information6
Device identifier
Numeric - 8,12,13 or 14 Digits
(Global Trade Item Number (Bar Code Number))
Production identifier
Alpha numeric
(Batch number, serial number or ‘use by’ date)
Provider identifier
Establishment or clinician identifier
Date of admission for implantation, revision or explantation
procedure(s)
Alpha numeric
DD/MM/YYYY
5
NHDD: National Health Data Dictionary, version 16 see http://www.aihw.gov.au/publicationdetail/?id=10737422826.
6
International Medical Device Regulators Forum (IMDRF), UDI Guidance: Unique Device Identification (UDI) of
Medical Devices, see: http://www.imdrf.org/docs/imdrf/final/technical/imdrf-tech-131209-udi-guidance.pdf
11
Documenting and testing data retrieval processes
12.
The Healthcare Organisation should:
a.
document a procedure that will enable timely and reliable retrieval of patient-,
device- and provider-identifying data for all Implanted Medical Devices; and
b.
undertake a practical test, and periodically review the effectiveness, of the data
retrieval procedure.
Note: Notwithstanding clause 8.b8.b.i, arrangements to store, search and retrieve data
necessary to identify patients with specific Implanted Medical Devices may vary between
Healthcare Organisations and/or Facilities. For example, some Healthcare Organisations
may collect relevant data in searchable electronic patient records, while others may rely
on extracting inventory and/or procedure data from searchable electronic systems
supported by manual searches of patient records.
Procedures for generating patient contact lists may vary, therefore, between Healthcare
Organisations and Facilities, but should be documented in accordance with local
arrangements and tested periodically.
J.
Registering with Health Professional Online Services
13.
The Healthcare Organisation should register with Medicare’s Health Professional Online
Services (‘HPOS’) to enable future access to patient contact information held by
Medicare7.
K.
Identifying Hazard Alerts
14.
The Hazard Alert Co-ordinator should regularly monitor the TGA website for new Hazard
Alerts.
The Healthcare Organisation should establish a procedure for staff and visiting medical
officers to inform the Hazard Alert Co-ordinator if they are notified of a relevant Hazard
Alert.
15.
7
More information about HPOS is provided in the Guide to implementing the National Patient Contact
Protocol.
12
PART 3 – RESPONSE
L.
Managing a Hazard Alert
Initiating the Healthcare Organisation’s response
16.
When a Hazard Alert is received, the Hazard Alert Co-ordinator should:
a.
immediately ensure all Implantable Medical Devices subject to the Hazard Alert
that remain in stock are quarantined;
b.
report the receipt of the Hazard Alert to the relevant Healthcare Organisation
quality, clinical governance and/or risk management committee(s);
c.
establish a log of key tasks;
d.
assign responsibilities and preliminary timeframes for completion of all tasks;
e.
seek appropriate clinical advice; and
f.
convene the Hazard Alert Committee as necessary, to advise on the
management of the Hazard Alert.
Planning for patient contact
17.
The Hazard Alert Co-ordinator, in collaboration with relevant clinicians and with advice
from the Hazard Alert Committee as appropriate, and taking into account the technical
and clinical advice available about the hazard, its urgency and management (including any
advice received from the CMO, the State/Territory CHO and/or the State/Territory Recall
Co-ordinator, if available), should:
a.
document a patient contact protocol that includes:
i.
the preferred mode(s) of patient contact (e.g. telephone, letter or a
combination of contact modalities) and the order in which they will
be effected;
ii.
who will contact patients;
iii.
the target timeframe for contacting patients;
iv.
key messages to be provided to patients, including:
A.
factual advice about the nature and significance of the
hazard and its recommended management, consistent with
the advice provided to the Healthcare Organisation by the
Sponsor, the TGA, the CMO, the relevant professional
college(s), the State/Territory CHO and/or the
State/Territory Recall Co-ordinator;
B.
details of specific actions the patient is advised to take to
protect their health and wellbeing (for example, initiate an
immediate consultation with their general practitioner or
specialist);
C.
details of a contact telephone number for patient to make
inquiries; and
13
D.
18.
a request for the patient or their family/carer to contact
the Healthcare Organisation within a specified timeframe
to confirm they have received the advice about the Hazard
Alert;
b.
prepare template patient contact letters, where required;
c.
prepare tools (e.g. standard forms) to record the outcome of each patient
contact;
d.
ensure adequate resources are available to provide appropriate clinical support
to patients including, where necessary:
i.
specialist consulting services;
ii.
theatre time and/or resources; and/or
iii.
a telephone inquiry line staffed by trained healthcare professionals;
e.
identify and train the staff who will be responsible for interacting with patients;
and
f.
implement appropriate training and develop appropriate resources for use by
personnel who may receive inquiries direct from the public or patients.
Arrangements for clinical interventions are outside the scope of the Protocol. In
collaboration with clinicians the Hazard Alert Co-ordinator should, however, commence
developing procedures addressing:
a.
any special elements of consent procedures needed to support the subsequent
clinical management of patients affected by the Hazard Alert;
b.
the scope of documentation to be included in patient clinical records of:
i.
the clinical interventions undertaken in response to the Hazard Alert;
ii.
where explantation occurs, the observed state of the Implanted
Medical Device;
c.
any testing, photography or other procedures proposed to be conducted on
explanted devices; and
d.
the disposition of devices that are explanted as a result of a Hazard Alert, noting
that:
i.
the safety of individuals potentially exposed to explanted devices
must be a priority; and
ii.
legal ownership of explanted devices may vary depending on
contractual arrangements.
Identifying affected patients
19.
The Hazard Alert Co-ordinator should:
a.
in collaboration with relevant personnel (e.g. procurement, supply and clinical
personnel):
i.
determine how many of the Implantable Medical Devices that are
subject to the Hazard Alert have been purchased by and/or supplied
to the Healthcare Organisation;
ii.
consider whether any of the Implantable Medical Devices that are
subject to the Hazard Alert have, or may have, been supplied by
visiting medical officers directly for patient use, and therefore will
not appear on usual hospital supply/inventory records;
14
iii.
b.
determine the number of patients in whom the Implantable Medical
Device that is subject to the Hazard Alert has been implanted; and
activate the documented procedure referred to in clause 12 to generate a
patient contact list.
Contacting patients
20.
21.
22.
23.
The Hazard Alert Co-ordinator should provide to the persons who have been allocated
responsibility for effecting patient contact:
a.
the patient contact list(s);
b.
where contact will be made by telephone, written advice of the information to
be conveyed to patients;
c.
where contact will be made by letter, template patient contact letters;
d.
tools to record the outcomes of patient contact efforts; and
e.
the agreed method and timelines for managing the Hazard Alert.
All written communications with patients about Hazard Alerts should be signed by a senior
manager or clinician, whose identity is clear.
Unless exceptional circumstances apply, all verbal communications with patients about
Hazard Alerts should be by senior healthcare professionals with specific knowledge of
both the implant that is subject to the Hazard Alert and the hazard that has been
identified.
The person(s) responsible for effecting patient contact should, in accordance with the
parameters defined in clause 1716.c:
a.
contact patients as expeditiously as possible;
b.
maintain accurate records in the agreed format of the outcomes of both
successful and unsuccessful patient contact efforts; and
c.
submit those records to the Hazard Alert Co-ordinator in accordance with the
agreed timelines.
Following up patients unable to be contacted
24.
25.
26.
Where the agreed patient contact procedures are followed but the Hazard Alert
Co-ordinator is unable to reliably verify that an affected patient has been contacted, the
Hazard Alert Co-ordinator should:
a.
if the urgency of the situation permits, make further efforts to contact the
patient; and/or
b.
utilise HPOS to identity the patient’s current contact details as recorded in the
Medicare customer database.
Following receipt from Medicare Australia of the patient’s current contact details as
recorded in the Medicare customer database, the Hazard Alert Co-ordinator should repeat
the step defined in clause 23 above.
Both the Healthcare Organisation and the relevant treating clinician should add an alert to
the medical record of each patient with an Implanted Medical Device that has been
subject to a Hazard Alert if the patient has not been contacted, to enable the patient to be
informed of the Hazard Alert in the event they make contact in the future.
15
Responding to inquiries
27.
Subject to privacy and confidentiality obligations:
a.
the Healthcare Organisation should:
i.
ensure accurate and timely responses to members of the public
and/or patients who initiate inquiries about the Hazard Alert;
ii.
consider establishing a ‘fast track’ process to provide specific device
information in writing to patients who have received an implant of a
similar type but are unsure whether their particular device is subject
to a Hazard Alert, which:
A.
minimises time delays and inconvenience for patients;
B.
is appropriately recorded; and
C.
does not incur any cost for patients.
iii.
respond to all relevant inquiries by the State/Territory Recall Coordinator, the TGA/Australian Recall Co-ordinator and/or the CHO
about the progress and/or effectiveness of the Hazard Alert
management process, subject to local communication protocols; and
iv.
maintain accurate records of all relevant inquiries and responses.
Maintaining appropriate records
28.
The Hazard Alert Co-ordinator should ensure accurate records of the Hazard Alert
management process and outcomes are maintained, including:
a.
the number of affected patients;
b.
records of all committee meetings and correspondence (email and other) about
the Hazard Alert and its management;
c.
a log of all telephone calls relating to the Hazard Alert and its management,
including a summary of issues discussed;
d.
date(s) letters are sent and/or telephone calls are made to patients;
e.
date(s) patient contact is confirmed;
f.
date(s) patients are reviewed by a clinician (if applicable);
g.
date(s) of receipt of returned written communications to patients;
h.
date of accessing the HPOS system to ascertain further contact details from the
Medicare customer service database;
i.
records relating to adverse events associated with the Hazard Alert
management process and outcomes;
j.
a log of complaints and other consumer feedback about the process; and
k.
outcomes of patient contact efforts.
16
PART 4 – RECOVERY
M.
Evaluating and reporting management and outcomes
29.
When implementation of the Hazard Alert management plan is completed, the Hazard
Alert Co-ordinator should:
a.
collate data and other information relevant to the Healthcare Organisation’s
performance in managing the Hazard Alert;
b.
lead a local review of the timeliness, efficiency and effectiveness of
management of the Hazard Alert incorporating:
i.
engagement of relevant personnel including the Healthcare
Organisation’s risk and quality assurance managers and participating
clinicians;
ii.
review of data and other information relevant to the Healthcare
Organisation’s performance in managing the Hazard Alert; and
iii.
identification of potential improvements;
c.
lead implementation of improvements identified in step b above;
d.
prepare a final report including:
i.
a reconciliation of the patient contact list with the patients
contacted;
ii.
an assessment of the effectiveness of management of the Hazard
Alert; and
iii.
specific recommendations for improvement;
e.
submit the final report, as appropriate, to:
i.
relevant clinicians;
ii.
the Healthcare Organisation quality manager and/or risk manager;
and
iii.
relevant Healthcare Organisation quality, clinical governance and/or
risk management committees.
17
N.
Supporting system level accountability
30.
Subject to relevant protocols and privacy and confidentiality obligations, the Healthcare
Organisation should:
a.
submit a comprehensive report on the management of the Hazard Alert to the
relevant State/Territory Recall Co-ordinator; and
b.
respond in a timely manner to requests for information about the effectiveness
of implementation of this Protocol from:
i.
the State/Territory Recall Co-ordinator;
ii.
the CHO;
iii.
the Sponsor;
iv.
the TGA and/or
v.
any other relevant authority.
END OF PROTOCOL
18
DICTIONARY
Active Implantable Medical Device means an active medical device, other than an Implantable
Medical Device, that is intended by the manufacturer:
(a)
(b)
either:
(i)
to be, by surgical or medical intervention, introduced wholly, or partially, into
the body of a human being; or
(ii)
to be, by medical intervention, introduced into a natural orifice in the body of a
human being; and
to remain in place after the procedure.
Active Medical Device:
(a)
(b)
means a medical device that is intended by the manufacturer:
(i)
to depend for its operation on a source of electrical energy or other source of
energy (other than a source of energy generated directly by a human being or
gravity); and
(ii)
to act by converting this energy; but
does not include a medical device that is intended by the manufacturer to transmit
energy, a substance, or any other element, between an active medical device and a
human being without any significant change in the energy, substance or other element
being transmitted.
Explantation means the removal of an Implanted Medical Device from a person’s body.
Hazard Alert means the issuing of precautionary information about an Implanted Medical Device.
Hazard Alert Co-ordinator means the person appointed from time to time to assume the
responsibilities of co-ordinating the management of Hazard Alerts in a Healthcare Organisation or
Facility.
Healthcare Facility means any public or private facility in which an Implantable Medical Device is
implanted in a human being, including a hospital, day procedure centre or professional consulting
suite.
Healthcare Organisation means any entity or individual that provides healthcare services that
include the implantation of Implantable Medical Devices in human beings.
Implantable Medical Device means a medical device (other than an Active Implantable Medical
Device) that is intended by the manufacturer:
a.
b.
to be, by surgical intervention, wholly introduced into the body of a human being, and to
remain in place after the procedure; or
to replace, by surgical intervention, an epithelial surface, or the surface of an eye, of a
human being, and to remain in place after the procedure; or
19
c.
to be, by surgical intervention, partially introduced into the body of a human being, and to
remain in place for at least 30 days after the procedure.
Implanted Medical Device means an Implantable Medical Device or an Active Implantable Medical
Device that has been implanted in a human being.
Recall means the permanent removal of therapeutic goods from supply or use for reasons relating to
deficiencies in the quality, safety or efficacy of the goods. It includes:
a.
b.
requests to pharmacists, hospitals, pathology laboratories, fractionators, operating and
research facilities, biomedical engineers or others to check and return goods found to be
defective; and
removal from supply or use of goods with inherent design or manufacturing defects.
Sponsor means the person, business or company that has the primary responsibility for the supply,
including for clinical investigational use, of the product in Australia. The Sponsor may also be the
manufacturer of goods.
State/Territory Recall Co-ordinator means the person(s) appointed from time to time by each State
and Territory to co-ordinate recalls of therapeutic goods in their jurisdictions.
20