Document 6819715
advertisement

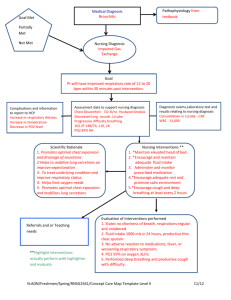
Student Name: Vendula Stepan Nursing Assessment Form Client Name: F.V. 84 years old Medical Diagnosis: SEE PATHOLOGY RECORD Client Perception of Health Needs: Being as much independent as she can but needs assistance with daily care. Client Goals for Health: Maintain mobility and current condition, never give up on anything. Allergies (food, medication, environmental) Penicillin, Sulfa/Sulfonamide, Emycin base – hives, Procaine – swelling blisters, Mold SEE MEDICATION RECORD Medications Dietary considerations Regular Vital Signs T 36.3 P 73 R 16 BP 172/64 O2 97% RA Pain rating 0 HEALTH ASSESSMENT DATA Physiological Variable General Appearance/Mental State: Cardiovascular System: Female, 84 years old. Appears stated age. No signs of distress. Alert and oriented, confusion varies day by day. Body type – well nourished. Affect and facial expression appropriate to situation. Posture – slightly bent. Gait unsteady and weak., Speech clear, understandable and moderately paced. Radial pulse regular, strong, no edema, capillary refill less than 2 seconds, history of DVT Respiratory System: Gastrointestinal System: Rate 16, air entry equal bilaterally, no crapitations or wheezes, no supplementary O2 use, no accessory muscles used. Abdomen round and soft. Bowel sounds x 4. Regular bowel movement. Urinary System: Sensory Systems: Bladder incontinence, No pain or bladder tenderness reported. Vision – both eyes impaired, wears glasses, family history glaucoma, yearly check ups History caract surgery Hearing – no hearing impairment Speech – preferred spoken language English, excellent ability to follow directions Student Name: Vendula Stepan HEALTH ASSESSMENT DATA Nervous System: Integumentary System: No tremors Skin thin, pink, intact, dry, very fragile, often skin tears, no edema Musculoskeletal System: Reproductive System: Uses wheelchair Unstable gait Bilaterally hip replacement One person Assist + using transfer belt Postmenopausal Tubal ligation Endocrine System: Client Resuscitation Status: History of Tonsillectomy M1 – medical care and interventions, excluding resuscitation Spiritual Variable (Environment) Developmental Variable (Environment) According to the patient she is Christian, Attends all activities provided in the long term facility – craft, board games, making puzzles. Married, retired, previous occupation a nurse, living in the long term facility – single room, two kids –son Doug and son David Development stage according to Erikson’s Theory: Integrity versus despair Sociological Variable (Environment) Psychological Variable (Environment) Born in Canada, Primary language English enjoys any social activities and loves to be involved in anything. Support system her husband and two sons. Both sons living in Camrose. Determinants of health impacting client’s health (Environment) My patient previous occupation was a nurse. The long term facility she resides in has positive influence on her health because of the ability to socialize with other residents, with all the stuff and as well she is involved in the nursing environment. She loves this socializing aspect and being around what she has done for her whole life. She is support for residence and always tries to make them feel better if they don’t feel well. Every day she helps with small stuff such as folding towels. Interdisciplinary Team Members Physician- RN and LPN nurses, Nursing Assistants, Registered Dietitian ,Occupational therapist, Pharmacist, Resident Care manager ,Chaplain Health Priorities - Client stated: “Never give up on anything in your life especially your health. If you don’t feel well go and see your doctor. There is always a way to get healthy and feel better.” Client also feels that being independent leads you to better quality life. Client Strengths - Client is very pleasant residence. She is very strong minded person and is very good influence for other residence. Loves to socialize and being part of any activities happening in long term facility. Student Name: Vendula Stepan HEALTH ASSESSMENT DATA Laboratory/Radiology Reports 7.4.2015 Chemistry – Creatinine 285 umol/l high, GFR 13 high CBC – RBC – 3.85 10*9/L Low HGB – 109 g/L low HCT – 0.34 L/L low 15.05.2015 Xray of hand Severe tissue swelling and some body erosions and surrounding the third and fourth finger DIP joints. It could potentially be from trauma, or from goat, or less likely from infections. No soft tissue classification. Student Name: Vendula Stepan Pathophysiology Record Must be written in your own words (i.e., as if teaching a patient) Medical Diagnosis Pathophysiology Signs and Symptoms High blood pressure – blood pressure is the force of blood pushing against the walls of the arteries as the heart pumps blood. When the blood pressure is too high it can cause damage Headache, blurred vision, nausea, vomiting, weakness, fatigue, confusion and mental changes A weakness of the heart that leads to a buildup of fluid in the lungs and surrounding body tissues. breathing difficulties during the night or when lying down, coughing and wheezing, fatigue and weakness, shortness of breath, swollen ankles Osteoporosis Bones becoming fragile and brittle Bone fractures especially in vertebra Dementia other than Alzheimers A chronic or persistent disorder of the mental processes caused by brain disease or injury and marked by memory disorders, personality changes, and impaired reasoning. Memory loss, impaired judgment, Difficulties with abstract thinking, Faulty reasoning, Inappropriate behavior, Loss of communication skills, Disorientation to time and place, Gait, motor, and balance problems. Hypertension Congestive Heart Failure 1. Complications Stroke – rupture of cerebral vessels due to hypertension Pulmonary edema Heart failure Renal insufficiency – poor urine output, protein in the urine, problems with elimination waste Shortness of breath, Orthopnea – shortness of breath while lying flat, Paroxysmal nocturnal dyspnea (PND) - sudden episodes that awaken a patient at night, fluid retention – edema and gain weight, loss of muscle mass, loss of appetite, pulmonary edema, abnormal heath rhythms Bone fractures loss of ability to function or care for self, loss of ability to interact with others, reduced lifespan, increased infections anywhere in the body, forgetting recent events or conversations, difficulty performing more than one task at a time, forgetting details about current events, difficulty swallowing both foods and liquids Student Name: Vendula Stepan Pathophysiology Record Must be written in your own words (i.e., as if teaching a patient) Medical Diagnosis COPD – emphysema Gastrointestinal disease 2014 – GI bleed diverticulitis Pathophysiology Signs and Symptoms Complications All chronic obstructive lung problems Irreversible enlargement of the air spaces beyond the terminal bronchioles, most notably in the alveoli, resulting in destruction of the alveolar walls and obstruction of airflow. Disease of the large intestine, diverticulum small sac forms along the wall of the colon if it get infected - diverticulitis Chronic hypoxemia - an abnormally low concentration of oxygen in the blood, hypercapnia - excessive carbon dioxide in the bloodstream, chronic cough most in the morning, dyspnea – difficult breathing, wheezing, pursed lip breathing Abdominal pain, fever, nausea, vomiting, rectal bleeding Pneumothorax – collapsed lungs, cor pulmonare - a section of the heart expands and weakens, right sided heart failure, respiratory failure Renal failure – chronic Kidneys fail to adequately filter waste products from the blood. Abnormal dark or light skin, bone pain, drowsiness or problems concentrating or thinking, numbness or swelling in the hands and feet, muscle twitching or cramps, easy bruising, blood in the stool, excessive thirst. Goat A disease in which defective metabolism of uric acid causes arthritis, especially in the smaller bones of the feet, deposition of chalkstones, and episodes of acute pain. Formation of one or more blood clots in one of the body's large veins, usually in legs Sudden onset of a hot, red, swollen joint first in big toe, tenderness, hyperuricemia – high blood levels of uric acid DVT – deep vein thrombosis pain, swelling and tenderness in one of the leg (usually your calf), redness of skin, warm in the area of clot Bleeding, urinary problems, abscess - a pus-filled cavity or lump in the tissue, Fistulas are abnormal tunnels that connect two parts of the body together, such as your intestine and your abdominal wall or bladder, peritonitis – infection of the abdomen, intestinal obstruction Anemia, hypertension – high blood pressure, bone changes of secondary hyperparathyroidism - an abnormally high concentration of parathyroid hormone in the blood, pulmonary edema, infections, poor wound healing, Joint damage, tophi - crystals of sodium urate often form in tissues both outside and inside the joint, kidney stones, depression, anxiety Pulmonary embolism, postphlebitic syndrome - caused by damage to veins from the blood clot Student Name: Vendula Stepan Nursing Process Care Plan (Use 1 sheet per Diagnosis) Nursing Diagnosis Planning Interventions Evaluation Use assessment data to establish a nursing diagnosis that reveals: • an actual problem • a potential problem • an educational need or a need related to medication administration 1. Client Goals: Write one specific and measurable client behavioral response. 1. List Interventions: Select nursing interventions to meet the goals set, and to change or maintain health status 1. Achievement of Expected Outcomes: Assess goal achievement and reasons, and set new plan as needed. 2. Client Responses and Findings: Describe why goal was met of not met. Summarize the effectiveness of nursing interventions. 3. Further Nursing Actions: Assess evidence that outcome was met. Readjust nursing care plan as necessary. Chronic pain related to chronic physical disability as evidenced by gout. Patient reports pain at a level 0-4 on a scale 0-10 every day. Assess pain characteristics – quality, severity, location, onset, precipitating factors, relieving factors Patient didn’t experience any pain – pain level 0 every day during my every day shift. Patient engages in desired activities. Rationale : Assessment of chronic pain guides the pain management plan. Goal was met because patient was taking her pain medication on regular base and was able to participate in desired activities. 2. Expected Outcomes: Write statements in measurable terms that support the goal by using the SMART criteria: Specific Measurable Attainable Realistic Time-based Patient uses pharmacological and nonpharmacological pain relief strategies. 2. Rationale for Interventions: Provide rationale for selection of nursing interventions and use appropriate literature such as text, articles, and internet sites to support internet sites to support choices. Assess patient’s ability to complete activities of daily activity and demands of daily living. Rationale: Fatigue, anxiety and depression due to chronic pain and may affect activities and reduce the patient’s ability to fulfill role responsibilities Encourage the patient to follow a pain management strategy. Rationale: Medications should be given around-theclock to achieve consistent pain relief. Student Name: Vendula Stepan Nursing Process Care Plan (Use 1 sheet per Diagnosis) Nursing Diagnosis Planning Use assessment data to establish a nursing diagnosis that reveals: • an actual problem • a potential problem • an educational need or a need related to medication administration 1. Client Goals: Write one specific and measurable client behavioral response. Risk for falls related to decrease mobility as evidenced by using a wheelchair. Client will not experience any falls during my shifts within one week. 2. Expected Outcomes: Write statements in measurable terms that support the goal by using the SMART criteria: Specific Measurable Attainable Realistic Time-based Client and I will make necessary physical changes in environment such as maintain proper illumination inside and outside where the patient moves and walks, remove clutter from bedside tables, hallways, bathrooms and grooming areas, secure electrical cords against the baseboards….. to ensure increased safety within first week. Interventions Evaluation 1. List Interventions: Select nursing interventions to meet the goals set, and to change or maintain health status 1. Achievement of Expected Outcomes: Assess goal achievement and reasons, and set new plan as needed. 2. Client Responses and Findings: Describe why goal was met of not met. Summarize the effectiveness of nursing interventions. 3. Further Nursing Actions: Assess evidence that outcome was met. Readjust nursing care plan as necessary. 2. Rationale for Interventions: Provide rationale for selection of nursing interventions and use appropriate literature such as text, articles, and internet sites to support internet sites to support choices Asses ability to use call bell, side rails, bed controls, safety bars near toilets and proper light. Rationale: “Easy modification in a health care environment can reduce the risk of falls.” (Potter & Perry, 2014, p. 810) Routinely assist client in toileting on her own schedule. Rationale: “Many falls by older adults are related to the urge to urinate. Anticipate an older adults need to urinate and provide scheduled bathroom visits.” (Potter & Perry, 2014, p. 1136) Ensure that patient wears properly fitting shoes or slippers with a nonskid surface. Rationale: “Such footwear reduces the chances of slipping.” (Potter & Perry, 2014, p. 811) Client didn't experience any falls within one week. Goal was met because patient called anytime when she needed any assistance, had proper shoes on while I was transferring her to her wheelchair and as nurse I was coming regularly to check on patient in case she needs to go to washroom. Student Name: Vendula Stepan Nursing Process Care Plan (Use 1 sheet per Diagnosis) Planning Interventions Evaluation Use assessment data to establish a nursing diagnosis that reveals actual / potential wellness / problems. • an actual problem • a potential problem • an educational need or a need related to medication administration 1. Client Goals: Write one specific and measurable client behavioral response. 2. Expected Outcomes: Write statements in measurable terms that support the goal by using the SMART criteria: Specific Measurable Attainable Realistic Time-based 1. List Interventions: Select nursing interventions to meet the goals set, and to change or maintain health status. 2. Rationale for Interventions: Provide rationale for selection of nursing interventions and use appropriate literature such as text, articles, and internet sites to support choices. 1. Achievement of Expected Outcomes: Assess goal achievement and reasons, and set new plan as needed. 2. Client Responses and Findings: Describe why goal was met of not met. Summarize the effectiveness of nursing interventions. 3. Further Nursing Actions: Assess evidence that outcome was met. Readjust nursing care plan as necessary. Decreased cardiac output related to inadequate blood pumped by the heart as evidenced by hypertension. Maintain patient blood pressure within acceptable range by taking medication to control blood pressure within one month. Monitor and record BP. Measure in both arms and thighs three times, 3–5 min apart while patient is at rest, then sitting, then standing for initial evaluation. Rationale: Comparison of pressures provides a more complete picture of vascular involvement or scope of problem. Systolic hypertension also is an established risk factor for cerebrovascular disease and ischemic heart disease, when diastolic pressure is elevated. Goal was not met. Patient’s blood pressure still remains high. Nursing Diagnosis Client and I will discuses activities in which client can participate in to reduce blood pressure. Client and I will talk about diet restriction decreasing dietary sodium, fat and cholesterol. Client and I will talk about medication which she will take for her blood pressure and its side effects. Asses for edema Rationale: May indicate heart failure, renal or vascular impairment. Assess the presence, quality of central and peripheral pulses. Rationale: Pulses in the legs/feet may be diminished, reflecting effects of vasoconstriction (increased systemic vascular resistance [SVR]) and venous congestion. Observe skin color, moisture, temperature, and capillary refill time. Rationale: Presence of pallor; cool, moist skin; and delayed capillary refill time may be due to peripheral vasoconstriction or reflect cardiac decompensation/decreased output. Student Name: Vendula Stepan Medication Research Record Ensure you relate the medication information to the appropriate medical diagnosis. Please use lay terms as if you were teaching a patient. Medication/Reason for Medication Order Tylenol, Novo- Gesic Forte acetaminophen 500mg tablet Ventolin HFA salbutamol 100 mcg/dose MDI 200 Lopresor, Betaloc, ApoMetoprolol metoprolol 25mg tablet La-A-Day, Miralax powder polyethylene glycol 3350 powder Dosage/Safe Dose Action as Related to Medical Diagnosis 2xdaily Oral 500 mg 8,20 Generalized pain – nonopiod analgesics Inhibits the synthesis of prostaglandins that may serve as mediators of pain and fever, primarily in the CNS Used as a long term control agent in patients with chronic bronchospasm spasm of bronchial smooth muscle producing narrowing of the bronchi GI – hepatitic failure – failure of the liver and hepatotoxicity – toxicity of liver GU – renal failure Derm – rash, hives Asses type, location and intensity of pain Asses amount , frequency and type of drugs taking in patients selfmedicating, especially OTC drugs CNS – nervousness, restlessness, tremor CV – chest pain, palpitations GI – nausea, vomiting Neuro - tremor Assess lung sounds, pulse and blood pressure Monitor pulmonary function testes before and during therapy Decrease blood pressure and heart rate by blocking stimulation of beta adrenergic receptors. CNS – fatigue, weakness, anxiety EENT – blurred vision, stuffy nose Resp – wheezing CV – pulmonary edema, hypotension GI – constipation, diarrhea GU – urinary frequency Derm – rashes MS – back pain, joint pain Monitor blood pressure and pulse Monitor intake and output and weight Treatment of constipation – evacuation of the GI tract without water or electrolyte imbalance GI – abdominal bloating, cramping, nausea Assess patient for abdominal distention, presence of bowel sounds and usual pattern of bowel function Assess color, consistency and amount of stool produced 4xdaily Inhalation Inhale 2 puffs 8,12,17,20 2x daily Oral 25mg 8,20 Daily Oral 17 gm dissolve in water or juice 8 Common Side Effects Nursing Implications Student Name: Vendula Stepan Medication Research Record Ensure you relate the medication information to the appropriate medical diagnosis. Please use lay terms as if you were teaching a patient. Medication/Reason for Medication Order Dosage/Safe Dose Action as Related to Medical Diagnosis Entrophen, Asaphen aspirin 81mg tablec EC Daily Oral 81mg 8 For stroke prevention, reduce inflammation and fever by inhibitin the production of prostaglandins, also decreases platelet aggregation EENT – hearing loss, ringing in the ears GI – bleeding heartburn, nausea, abdominal pain, vomiting Misc – allergic reactions including anaphylaxis and laryngeal edema Assess pain Monitor patient for toxicity and overdose Oscal, Novo-Calcium Calcium salts 1250 mg Daily Oral 500mg 8 Adjunct in the prevention of postmenopausal osteoporosis CNS – tingling CV – arrhythmias GI – constipation, nausea, vomiting GU - calculi Daily Oral 1000 unit 8 Vitamin D is a fat-soluble vitamin that helps your body absorbs calcium and phosphorus. Having the right amount of vitamin D, calcium, and phosphorus is important for building and keeping strong bones. Vitamin D is used to treat and prevent bone disorders - Osteoporosis Seen primarily as manifestations of toxicity. CNS – headache, weakness CV – hypertension, edema, palpitations, fast heart beat, GI – constipation, dry mouth, nausea Derm – hives, itching, rash Assess patient for symptoms of hypocalcemia Monitor blood pressure and pulse Monitor patient for toxicity and overdose Assess for symptoms of vitamin deficiency Assess patient for bone pain and weakness Assess patient for Toxicity and Overdose – nausea, vomiting, anorexia, weakness, constipation, headache, bone paint and metallic taste Daily Oral 100mg 8 Prevention of attack of gouty arthritis, inhibits production of uric acid – lowering of serum uric acid levels CNS – drowsiness GI – diarrhea GU – renal failure Derm – rash Hemat – bone marrow depression Misc - hypersensitivity reactions Vitamin D3 Cholecalciferol 1000 unit tablet Zyloprim, Novo-purol allopurinol 100mg tablet Common Side Effects Nursing Implications Monitor output and intake Assess patient for rash or any other severe hypersensitivity reactions Monitor for joint pain and swelling Monitor serum uric acid levels, renal and liver function tests Student Name: Vendula Stepan Medication Research Record Ensure you relate the medication information to the appropriate medical diagnosis. Please use lay terms as if you were teaching a patient. Medication/Reason for Medication Order Risperdal risperidone 0.125mg tablet Coversyl, Aceon perindopril 2mg tablet Dosage/Safe Dose Action as Related to Medical Diagnosis Common Side Effects Nursing Implications Daily at bedtime Oral 0.125 mg 20 Decrease symptoms of psychoses or bipolar mania by antagonizing dopamine and serotonin in the CNS CNS – aggressive behavior, dizziness, headache, increase dreams, increased sleep duration, insomnia EENT – visual disturbance Resp – cough, dyspnea GI – constipation, dry mouth Derm – skin rash, itching Misc – weight gain Monitor patient mental status Monitor mood changes Monitor blood pressure and pulse Monitor for extrapyramidal side effects and neuroleptic malignant syndrome – restlessness, muscle spasm and twisting motions, mask like face, rigidity, tremors, fever, respiratory distress, seizures Daily Oral 2 mg 8 Management of hypertension – high blood pressure - lowering blood pressure and decrease development of overt heart failure CNS – dizziness, fatigue, headache Resp – cough CV – hypotension – low blood pressure, GI – taste disturbance, nausea GU – proteinuria – protein in the urine, renal failure Monitor blood pressure and pulse Monitor weight Monitor blood - CBC Student Name: Vendula Stepan Nursing Care Plan - Summary Describe the benefits of using the nursing process and the nursing concepts in your assessment and nursing care. Assessment: The benefits of using nursing process and the nursing concepts in my assessment helped to organize my work step by step and therefore assisted me to better understand what the appropriate outcome for my patient should be. Nursing Care: Proper assessment helped me to prioritize my nursing care resulting in better clarification of focusing on issues that require priority. In relations to the assessment I made on my patient my priority was to focus on patients pain level due to her medical diagnose - goat, control patients pain and therefore increasing better quality of life.