3 health efect caused by radiation - GNSSN Home
advertisement

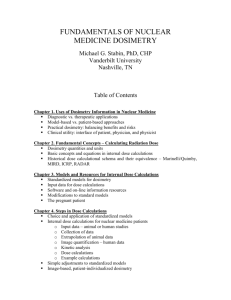
3. HEALTH EFFECTS CAUSED BY RADIATION AND BASIS FOR RADIOLOGICAL PROTECTION 3.1. Introduction When ionizing radiation passes through matter, some of its energy is imparted to the matter by means of ionization and excitation of atoms and molecules. Impartment of radiation energy to matter is the start point for developing radiation health effects in human, animals, plants and microorganisms – in all alive beings. Tissues and organs are composed by cells of different kinds and radiation damage of these cells leads to development of radiation health effects. The target for most biological effects of ionising radiation is the genome of the cell, the DNA, which is the macromolecule of deoxyribonucleic acid. That molecule has very complicated structure, which primary structure could be imagined as double helix. Two stands of DNA helix contain complimentary copies of cell genome information, which plays the key role of the cell reproduction. Even a single ionization by a particle or a photon can cause a break in the DNA molecule. If it is a break in one strand of the DNA only (a single strand break) it will most probably be perfectly repaired with no consequences for the cell genome. Cells have tremendous ability to repair damage. As a result, not all radiation damages of DNA are irreversible. In many instances, the cells are able to completely repair any damage and function normally. If, however, both DNA strands are broken close to each other, repair mechanisms are likely to fail and the cell genome may be modified. In some case, as shown in Figure 03-1, the damage is severe enough that the cell dies or loss ability for reproduction (cell division). In other instances, the cell is damaged but it still able to reproduce. The daughter cell, however, may be lacking some critical life sustaining components, and they die. Finally, the cell may be affected in such a way that it does not die but is simply mutated. The mutated cell reproduces and thus perpetuates the mutation. This could be the beginning of the malignant tumour. Figure 03-1. Outcomes of DNA damage Generally, cells are most sensitive to radiation when they are in stage of cell division, so that the most radiosensitive tissues are the blood, the intestinal wall, the skin, and the foetus. Cells of that tissues and organs demonstrate the high reproduction intensity. Conversely, the most radioresistant tissues are muscle, nerves, and the adult brain, where the intensity of cell reproduction is minimal. 1 Probability of development of DNA damage after irradiation is grooving up with concentration of ionizations and excitations in the media, which defines the absorbed dose of ionizing radiation. The absorbed dose D R is the energy imparted to matter by ionizing radiation R per unit mass of irradiated material at the place of interest. The unit of absorbed dose is J×kg-1, called the gray (Gy). Table 03-01 presents a list of radiation-induced health effects that would be critical during an emergency. Experience and research indicate that evaluation of the dose to the target organs presented in the table should provide a basis for criteria for making decisions that will address the full range of potential adverse health effects in emergency exposure situation. Table 03-1. Critical radiation-induced health effects during a radiation emergency Health effect Fatal Haematopoietic syndrome Gastrointestinal syndrome Target organ or entity Severe deterministic health effects Red marrow (a) Small intestine for external exposure (a) or Colon for internal exposure (b) Lung (a), (c) Embryo/foetus in all periods of gestation Pneumonitis Embryo/foetal death Nonfatal Moist desquamation Skin (d) Necrosis Soft tissue (e) Cataract Lens of the eye (a), (f) Acute radiation thyroiditis Thyroid (a) Hypothyroidism Thyroid (a) Permanently suppressed ovulation Ovary (a) Permanently suppressed sperm Testes (a) counts Severe mental retardation Embryo/foetus 8–25 weeks of gestation Verifiable reduction in IQ Embryo/foetus 8–25 weeks of gestation Malformation Embryo/foetus 3–25 weeks of gestation [#543] Growth retardation Embryo/foetus 3–25 weeks of gestation [#543] Stochastic health effects Thyroid cancer Thyroid All stochastic health effects All organs taken into account in definition of effective dose (a) External exposure to the red marrow, lung, small intestine, gonads, thyroid and lens of eye from irradiation in a uniform field of strongly penetrating radiation is addressed by AD red marrow. (b) (c) (d) (e) (f) Different targets for gastrointestinal syndrome are proposed because of difference in dose formation in small intestine and colon in case of internal exposure. This is due to difference in the kinetics of ingested material in the gastrointestinal (GI) tract, which leads to much higher doses in colon than in small intestine after intake. For the gas-exchange (alveolar interstitial (AI)) region of the respiratory system. Skin structures at a depth of 50 mg/cm2 (or 0.5 mm) under the surface and over an area of 100 cm2 To a depth of 0.5 cm in tissue. Lens structures at a depth of 300 mg/ cm2 (or 3 mm) under the surface. 2 The health effects of ionizing radiation need a time for development from physical act of energy absorption to medical syndrome. Figure 03-2 presents the time perspective of development biological effects. This time perspective plays the important role in evaluation of causality of health effects and exposure. TIME SCALE EFFECTS Fractions of seconds Energy absorption Changes in biomolecules (DNA, membranes) Seconds Biological repair Change of information in cell Minutes Hours Weeks Germ cell Cell death Days Organ failure Mutations Somatic cell Clinical changes Months Years Leukaemia or solid cancer Decades Hereditary effects Generations Figure 03-2. Biological effects of radiation in time perspective. Another aspect of time perspective is the competition of deterministic and stochastic effects in causation of untimely death after exposure. Because of short time for development, the deterministic effects win in case of high dose exceeding the threshold level. The overexposed individual will die because of development of deterministic effects before the stochastic effect becomes apparent. Therefore At high doses cell death and loss of ability for reproduction reproductive leads to development of deterministic health effects (organ death or clinical changes). Such an effect is described as a severe deterministic effect if it is fatal or life threatening or results in a permanent injury that reduces quality of life. At low doses, when probability of cell survival after irradiation is high, the development of mutated cell could give a rise for stochastic health effects of radiation (hereditary effects or cancers). 3.2. Dosimetric quantities for use in characterization of emergency exposure situation Biological effects of radiation are correlated with the energy absorbed by ionization and excitation in unit mass of tissue (the absorbed dose). The effects are modified by microscopic spatial distribution of energy of radiation imparted to matter, which depends on quality of radiation. It also can be modified by dose rate, concentration of oxygen in tissue as well as by other factors determining radiosensitivity of biological object concerned. The absorbed dose in organ or tissue provides the dosimetric basis for evaluating the risk of development of stochastic and deterministic effects after the exposure. The average absorbed dose in organ or tissue D R ,T (absorbed organ dose) is the dosimetric quantity, which 3 characterises the energy absorbed by ionization and excitation in unit mass of tissue or organ T [#502]: D R ,T E R ,T , (03- 1) mT where E R ,T is the energy absorbed in tissue or organ T and mT is the mass of that organ or tissue. The unit of absorbed dose is J×kg-1, called the gray (Gy). The dosimetric quantities of effective dose, equivalent dose, and RBE weighted absorbed dose are used in evaluating radiation induced consequences in emergency exposure situations. The dosimetric quantities of personal dose equivalent and ambient dose equivalent are used in individual and areal monitoring in emergency. These quantities are listed in Table 03-2. The Figure 03-3 [#501] illustrates links between absorbed organ dose and other dosimetric quantities. Table 03-2. Dosimetric quantities used to characterise of emergency exposure situation Operational quantities Radiation protection quantities Dosimetry quantity RBE weighted absorbed dose in organ or tissue Equivalent dose in organ or tissue Symbol Purpose Unit AD T For evaluating deterministic health effects induced due to exposure of an organ or tissue Gy HT For evaluating stochastic health effects induced due to exposure of an organ or tissue Sv Effective dose Personal dose equivalent H P (d) For evaluating detriment related to the occurrence of stochastic health effects in an exposed population For monitoring external exposure of an individual Ambient dose equivalent H*(d ) For monitoring a radiation field at the site of an emergency E Sv Sv Sv The radiation protective quantities of effective dose, equivalent organ dose, and RBE weighted organ dose could not be directly measured. They have to be calculated on the base of characteristics of exposure pathways and exposed person. Radiation protection quantities are used for purposes of radiation protection and safety to express the criteria of safe conditions for life and work. 4 Intake of radionuclide I, Bq RBE weighted dose in tissue or organ T, ADT [Gy] RBER,T Risk of deterministic effects Absorbed dose in tissue or organ T, DT [Gy] Radiation fluence F, [cm-2] Equivalent dose Equivalent dose tissue Equivalent dose inin tissue oror organ in tissue or organ T,T, [Sv] organ T T, HTH[Sv] HT [Sv] WR Effective dose, E [Sv] Radiation detriment QR Personal dose equivalent, HP(d) [Sv] Individual monitoring QR Ambient dose equivalent, H*(d) [Sv] Area monitoring WT Absorbed dose D [Gy] at surface of body Absorbed dose D [Gy] at a point Risk of stochastic effects Figure 03-3. Dosimetric quantities and their application in an emergency exposure situations. The RBE weighted dose in an organ or tissue (RBE weighted average absorbed dose) AD T is defined as a product of averaged absorbed dose D R ,T of radiation (R) in organ or tissue (T) and the relative biological effectiveness ( RBE R ,T ): AD T D R ,T RBE R ,T (03- 2) The relative biological effectiveness is a measure of the relative effectiveness of different radiation types at inducing a specified health effect, expressed as the inverse ratio of the absorbed doses of two different radiation types that would produce the same degree of a defined biological end point. Values of relative biological effectiveness in causing the development of deterministic effects are selected to be representative of the severe deterministic effects that are significant to emergency preparedness and response. The tissue specific and radiation specific values of RBE R ,T for the development of selected severe deterministic effects are as shown in the Table 03-3 [#501], [#511], [#512]. The RBE weighted dose is intended to account for differences in biological effectiveness in producing deterministic health effects in organs or tissues of reference man due to the quality of radiation. The unit of the RBE weighted dose in SI is Jkg-1 and is called the gray (Gy) [#501], [#502]. R 5 Table 03-3. Tissue- and radiation-specific values of RBE for developing selected severe deterministic health effects. Health effect Critical organ Haematopoietic syndrome Red marrow Pneumonitis Lung (b) GI Syndrome Colon Exposure (a) RBE External and internal External and internal n0 Internal Internal External and internal External and internal n0 Internal Internal External and internal 1 3 1 2 1 3 1 7 1 External and internal n0 3 Internal 1 0 (c) Internal 1 External , Necrosis Soft tissue (d) 0 External n 3 1 External , Moist desquamation Skin (e) External n0 3 (f) Intake of iodine isotopes 0.2 Hypothyroidism Thyroid Other thyroid seekers 1 (a) External , exposure includes the dose from bremsstrahlung produced within the source materials; (b) Tissue of alveolar-interstitial gas exchange region of respiratory tract; (c) For alpha-emitters uniformly distributed in the contents of the colon, it is assumed that irradiation of the walls of the intestine is negligible; (d) Tissue at a depth of 0.5 cm; (e) Tissue at a depth of 0.5 mm below skin surface over an area of more than 100 cm2; (f) Uniform irradiation of the tissue of the thyroid gland is considered to be five times more likely to produce deterministic health effects than internal exposure to low energy beta-emitting isotopes of iodine such as 131I, 129I, 125I, 124I and 123I. Thyroid seeking radionuclides have a heterogeneous distribution in thyroid tissue. 131I emits low energy beta-particles that lead to a reduced effectiveness of irradiation of critical thyroid tissues due to the dissipation of particles’ energy in other tissues. The RBE weighted organ dose is used for characterizing high-dose exposure to evaluate the likelihood of development of severe deterministic effects after external exposure and intake of radioactive material. The guidelines for evaluation of the likelihood of development of severe deterministic effects are provided in Refs. [#511], [#512], [#555], [#530]. The equivalent dose in organ or tissue (radiation weighted averaged absorbed dose in organ or tissue) H T is defined as the product of the averaged absorbed dose in the organ or tissue (D) and the radiation weighting factor w R [#502]: H T D R ,T w R R (03- 3) It is an organ-specific quantity that may be used for assessment of the risk of any radiationinduced cancer in an organ. The equivalent dose is intended to account for differences in 6 biological effectiveness in producing stochastic health effects in organs or tissues of reference man due to the quality of radiation. Equivalent dose is a measure of the dose to a tissue or organ designed to reflect the amount of harm caused. The values of an equivalent dose to a specified tissue from any type of radiation can therefore be compared directly. The unit of the equivalent dose in SI is Jkg-1 and is called the sievert (Sv) [#502]. Values of w R are shown in Table 03-4. Table 03-4. Radiation weighting factors for evaluation equivalent dose in tissue or organ Radiation Radiation weighting factor Photons, electrons, positrons and muons Protons and charged pions Alpha particles, fission fragments, heavy ions Neutrons 1 2 20 A continuous function of neutron energy: 2.5 18.2 exp( [ln( E n )] 2 / 6), E n 1 MeV 2 w R 5.0 17.0 exp( [ln( 2E n )] / 6), 1 MeV E n 50 MeV 2 E n 50 MeV 2.5 3.25 exp( [ln( 0.04E n )] / 6), The equivalent organ dose is used for characterizing low-dose exposure to evaluate the likelihood of development of stochastic effects after external exposure and intake of radioactive material. The guidelines for evaluation of the likelihood of development of stochastic effects are provided in Refs. [#519], [#533], [#547]. The effective dose is defined as the product of the equivalent dose in a tissue (T) and the tissue weighting factor ( w T ) representing its proportion of the detriment resulting from irradiation of tissue (T) to the total detriment when the whole body is irradiated uniformly [#502]. E HT w T (03- 4) T The effective dose is intended to account for differences in biological effectiveness in producing stochastic health effects due to the quality of radiation and its distribution in the body of reference man. The values of w T currently recommended by the ICRP are as given in Table 035. The total effective dose for the specified period (e.g., day, year, etc.) is widely used to formulate the regulatory requirements. It is the sum of the relevant doses from external exposure in the specified period and the relevant committed doses from intakes in the same period; the period for calculating the committed dose shall be 50 years for intakes by adults and to age 70 years for intakes by children. Values of effective dose from any type(s) of radiation and mode(s) of exposure could be compared directly. 7 Table 03-5. Tissue weighting factors for evaluation effective dose wT Tissue Bone-marrow (red), colon, lung, stomach, breast, remainder tissues Gonads Bladder, oesophagus, liver, thyroid Bone surface, brain, salivary glands, skin w T (a) 0.12 0.72 0.08 0.08 0.04 0.16 0.01 0.04 Total 1.00 (a) The w T for the remainder tissues (0.12) applies to the arithmetic mean dose of the 13 organs and tissues for each sex listed below. Remainder tissues: adrenals, extrathoracic (ET) region, gall bladder, heart, kidneys, lymphatic nodes, muscle, oral mucosa, pancreas, prostate (male), small intestine, spleen, thymus, uterus cervix (female). The organ weighting factors were chosen by the ICRP to reflect the relative detriment from cancer or occurrence of sever hereditary effects in the first generations after uniform whole-body exposure. The radiation detriment is the product of probability of occurrence and severity of injury or damage, which lead to a shortening duration of a normal life. The concept of radiation detriment have been introduced in the 1990 Recommendations of the ICRP [#552] and was upgraded in the 2007 Recommendations of the ICRP [#522]. Cancer needs a long period for latent developing. The shortest latent period is about 4-5 years for leukaemia. The first wave in Error! Reference source not found. presents development of leukaemia after brief exposure of red marrow. The wave in Error! Reference source not found. presents development of solid cancers (malignant tumours). The latent period for these cancers is several decades. Figure 03-4. Development of the stochastic effects in exposed group after brief uniform exposure of whole body. The Error! Reference source not found. shows the dynamics of development of radiation induced cancers after brief whole body exposure. The value of R T is a risk of development fatal cancer in organ T. It depends on dose, dose rate, time passed after exposure, and organ concerned. The value of TLat is the latent period, which depends on organ concerned. Cancer needs a long period for latent developing. The shortest latent period is about 4-5 years for leukaemia. The first wave in Error! Reference source not found. presents development of leukaemia after brief exposure of red marrow. The wave in Error! Reference source not found. presents development of solid cancers (malignant tumours). The latent period for these cancers is several decades. 8 Organs of the human body have different radiosensitivity. The severity of manifestations of the stochastic effect of irradiation of this organ is characterized by the average number of years of normal life lost because of cancer. The lower the latency period for cancer - the more years of life may be lost and the greater the severity of this effect. Without medical care, development of cancer leads to death quite quickly. The difference between life expectancy and latent period ( TLat ) is the lost period of normal life for victim ( TLost ). The value of TLost is used for evaluation of radiation detriment. Table 03-6 presents values of TLost used in evaluation of w T [#552]. Table 03-6. Life expectancy lost from stochastic effects Loss of lifespan, years Organ where stochastic effect is developed Red marrow 30 Gonads, Breasts 20 Bone surfaces, Liver, Skin, Thyroid, Lung, Colon, Remainder organs 15 Esophagus, Stomach, Urinary bladder 10 Reference stochastic effect 15 The radiation detriment is the product of probability of occurrence and severity of injury or damage, which lead to a shortening duration of a normal life. Severity of injury is measured in terms of years of a normal life, which loosed due to developing a radiation health effect. Its value characterizes the reference man. Value of radiation detriment cannot be measured. Radiation detriment is a quantity, which could be calculated on the base of estimating an effective dose. Limitation of radiation detriment is the basis for framework of radiation protection and safety. The effective dose was invented by the ICRP to account differences in biological effectiveness in producing harm, due to the quality of radiation and its distribution in the body of exposed individual. The effective dose (E) is widely used for justifying and optimizing protective actions [#502]. Effective dose is intended for use as a radiation protection quantity and therefore should not be used for epidemiological evaluations, nor should it be used for any specific investigation of human exposure. The 2007 Recommendations of the International Commission on Radiological Protection [#522] in paragraphs 153-154 determine the area for use of effective dose as follows. (153) The main and primary uses of effective dose in radiological protection for both occupational workers and the general public are: prospective dose assessment for planning and optimisation of protection; and retrospective dose assessment for demonstrating compliance with dose limits, or for comparing with dose constraints or reference levels. (154) In this sense, effective dose is used for regulatory purposes worldwide. In practical radiological protection applications, effective dose is used for managing the risks of stochastic effects in workers and the public. The calculation of effective dose or corresponding conversion coefficients for external exposure, as well as dose coefficients for internal exposure, are based on absorbed dose, weighting factors ( w R and w T ), and reference values for the human body and its organs and tissues. Effective dose is not based on data from individual persons (see 9 Annex B). In its general application, effective dose does not provide an individual-specific dose but rather that for a Reference Person under a given exposure situation. (155) There may be some circumstances in which parameter values may be changed from the reference values in the calculation of effective dose. It is, therefore, important to distinguish between those reference parameter values that might be changed in the calculation of effective dose under particular circumstances of exposure and those values that cannot be changed under the definition of effective dose (e.g., the weighting factors). Thus, in the assessment of effective dose in occupational situations of exposure, changes may be made that, for example, relate to the characteristics of an external radiation field (e.g., direction of exposure) or to the physical and chemical characteristics of inhaled or ingested radionuclides. In such cases it is necessary to clearly state the deviation from the reference parameter values. The effective dose is used for expression of dose limitations, e.g. dose limits, dose constraints or reference levels to control the exposure of the members of the public and workers. To estimate the radiation detriment due to use of radiation sources, the ICRP determined the detrimentadjusted nominal risk coefficients [#522]. This risk coefficient is the likelihood of loss of 15 years of normal life per 1 sievert of effective dose. Table 03-7 provides the detriment-adjusted nominal risk coefficients of effective dose for developing reference stochastic effect after exposure to radiation at low dose rate. Table 03-7. Detriment-adjusted nominal risk coefficients for developing reference stochastic effect after exposure to radiation at low dose rate Exposed population Total Cancer Heritable effects The general public 5.7×10-2 Sv-1 5.5×10-2 Sv-1 0.2×10-2 Sv-1 Occupational workers 4.2×10-2 Sv-1 4.1×10-2 Sv-1 0.1×10-2 Sv-1 In accordance to the ICRP, as mentioned above, the effective dose should not be used for evaluation of medical consequences of radiation exposure of the person. The detriment-adjusted nominal risk coefficients of effective dose from Table 03-7 provides basis for assessment of expected collective loss of life span by the members of certain exposed cohort. The collective exposure of cohort is expressed in terms of collected effective dose, which is the sum of effective doses received by the members of certain cohort S En . (03- 5) n The unit of collective dose is man-sievert (man-Sv). Product of detriment-adjusted nominal risk coefficient and collective dose provides estimation of collective loss of life span as follows. Expected detriment = Collective effective dose × Detriment-adjusted nominal risk coefficients for stochastic effects × Expected loss of lifespan For instance, the expected collective detriment of group of workers with collective dose of 1 man-Sv will be 0.63 man-y: 1 man-Sv × (4.2×10-2 Sv-1×15 y) = 0.63 man-y. 10 (03- 6) The assessment of collective dose and collective detriment could be used in cost-benefit analysis for optimization of radiation protection. It also used in comparison of different sources of harm [#569]. The operational quantities of personal dose equivalent and ambient dose equivalent are directly measurable quantities characterizing the exposure of reference person in actual radiation field. They are used for purposes of radiation protection and safety to express the operational criteria: ambient dose equivalent ( H*(d) ), i.e. the dose equivalent that would be produced by the corresponding aligned and expanded field in the ICRU sphere at a depth d on the radius opposing the direction of the aligned field; and personal dose equivalent ( H P (d) ), i.e. the dose equivalent in soft tissue below a specified point on the body at an appropriate depth d. Their units in SI are Jkg-1 and are expressed as sievert (Sv). Ambient dose equivalent and personal dose equivalent are the operational quantities based on the dosimetric quantity of dose equivalent. The dose equivalent is the product of the absorbed dose at a point in the tissue or organ and the appropriate quality factor for the type of radiation giving rise to the dose [#558]: H DR QR (03- 7) R The quality factor QR was introduced as a weighting factor to modify the absorbed dose and to define the dose equivalent with an objective to account the dependence of probability of development of stochastic effects on the quality of radiation. This dimensionless factor is given as a function of the unrestricted linear energy transfer as shown in Figure 03-5. Quality factors are the product of the relative biological effectiveness, (RBE's), averaged over several types of tissue, and certain other linear energy transfer (LET) factors expressing biological differences resulting from radiation absorption of the radiation type of interest and the reference radiation (200-250 keV X rays); they are assumed to be independent of type of organ exposed. Figure 03-5. Quality factor of radiation as a function of LET. 11 Any statement of personal dose equivalent or ambient dose equivalent should include a specification of the reference depth, d, with the value expressed in mm [#558]: If depth of 10 mm is employed; the operational quantities of H P (10) and H*(10) provide the best estimation of effective dose of external exposure in uniform parallel field of penetrating radiation; If a depth of 0.07 mm is employed, the operational quantity of H P (0.07) provides the best estimation of equivalent dose in basal layer of skin; If a depth of 3 mm is employed, the operational quantity of H P (3) provides the best estimation of equivalent dose in lens of eye. The table 03-02 shows that units of some dosimetric quantities, e.g. equivalent organ dose and effective dose, are similar. That situation should be kept in mind and any statement of dose value should include the reference to the dosimetric quantity used for characterization of exposure conditions. For instance, the statement of “1 mSv of effective dose” instead of “exposure dose of 1 mSv” shall be used. 3.3. Health effects caused by ionizing radiation Deterministic health effects The scientific knowledge about deterministic effects is based on radiobiological research and evaluation of clinical observation of people overexposed in radiation accidents or received high radiation doses in course of radiation therapy. In 1944 – 2010, about 260 radiation accidents were reported worldwide in which about 3000 people were exposed with RBE weighted whole body dose of above 0.25 Gy or organ dose above 0.75 Gy. These accidents were resulted in 168 registered fatalities [#509]. That number does not include fatalities in 9 reported nuclear submarine emergencies. Massive cell death in irradiated organ or tissue causes development of deterministic health effects of radiation (deterministic effect). The deterministic heath effect is a radiation effect for which generally a threshold level of dose exists above which the severity of the effect is greater for a higher dose. Cell survival after exposure is a stochastic process with probability depends on the exposure dose and dose rate. The higher dose and dose rate, the less probability of survival the fewer portions of cells in the organ survived after exposure [#504]. The effect will usually also decrease with dose rate, because a more protracted dose causes the cell damage to be spread out in time, allowing for more effective repair or repopulation. Deterministic effects occur at high doses when enough cells in an organ or tissue are killed or prevented from reproducing and functioning normally and there is a loss of organ function. A threshold dose exists above which the effects on an organ or biological system are clinically observable. Above the appropriate threshold, the effect becomes more severe as the radiation dose increases, reflecting the number of cells damaged. The threshold value reflects the minimal portion of survived cell that may be enough for relatively normal function of organ or tissue in organism. If exposure dose is below threshold, the loss a portion of cells of particular organ or tissue may be compensated by more intensive work of other organs or tissues. In general, the dose-response function for tissues, i.e. the plot on linear axes of the probability of harm against dose, is sigmoid in shape. When dose is over threshold, a portion of survived cells is so small, that the system compensation of cell death could not be effective and the clinical effect of concern is developing. Dose-response function for deterministic effects is given in Figure 03-6(a). The onset of the symptoms usually shortens (from weeks to hours) and their severity increases with increasing a dose. Severe deterministic effects if developed leads to radiation induced death of exposed person. Causation of deterministic effects and exposure to ionizing radiation has a deterministic character. The time of appearance of tissue damage ranges from a few hours to many years after 12 the exposure, depending on the type of effect and the characteristics of the particular tissue. Cell death is an end-point of biological processes developing in time. The time period between exposure and developing radiation induced clinical effect is comparable with cell reaction to exposure or with life span of cell and varies from hours to months. Formerly, deterministic effects were termed "non-stochastic" effects. Now the new term “tissue reaction” is used by the ICRP for such kind of health effects [#551]. (a) (b) Figure 03-6. Dose-response dependence for radiation–induced health effects. (a) Deterministic effects; (b) Stochastic effects. Deterministic health could be classified as sever and non-severe. Such an effect is described as a ‘severe deterministic effect’ if it is fatal or life threatening or results in a permanent injury that reduces quality of life. Vomiting is an example of non-severe deterministic effect caused by total body irradiation. Time of its manifestation reflects severity of that effect and depends over the dose. Figure 03-7. Manifestation of emesis after brief whole body external exposure The quantitative characteristic of its severity is the time to onset of vomiting: the lover time to onset, the more severe the level of whole body exposure and injury is. Time to onset of vomiting is a function of a torso dose. Dose in red marrow could be assumed equal to this quantity in case of preliminary characterizing the emergency exposure. This dependence is useful for dose assessment in case of emergency exposure to photons. The Figure 03-7 presents a median RBE weighted dose in torso as a function of time to onset of vomiting [#506], [#507]: AD Torso 50 a t b , (03- 8) where AD Torso 50 is the median estimate of RBE weighted dose in torso (Gy), a = 4.47±0.16, and b = -0.57±0.045 and t - time to first emesis (hours). 13 In case of criticality emergency, the RBE of neutrons for this effect is about 1 [#507]. Confidence limits (yellow area) represent one SE from the fitted line (solid dark blue). Whole body radiation dose of greater than 1 Gy received in a short time results in the clinical "acute radiation syndrome". The symptoms include headache, dizziness, nausea, diarrhea, insomnia, decrease in white blood cells and platelets. This syndrome, which is dose related, can result in disruption of the functions of the bone marrow system (>1 Gy), the gastro-intestinal system (>5 Gy), and the central nervous system (>20 Gy). An acute dose over 3 Gy could be lethal if no qualified medical care is provided. Severity of the effects is characterized by probability of radiation induced premature death and time of occurrence and realization of effect in radiation-induced death. Figure 03-8 from Ref [#505] illustrates an increasing severity of radiation effects with increasing dose. The range depends on the non-uniformity of the dose distribution and individual radiosensitivity. 4 Gy – threshold (5% probability of death) for the haematopoietic syndrome; 6-8 Gy – threshold for radiation pneumonitis; 50 Gy – very fast death. It is recommended to briefly outline the general characteristics of the haematopoietic, gastrointestinal and neurovascular syndromes. Figure 03-8. Severity of acute radiation syndrome after brief whole body external exposure Information on humans and animals has made it possible to describe the symptomatology associated with the acute radiation syndrome (ARS) caused by more or less uniform irradiation of whole body. In humans, ARS is defined as the symptoms manifested after whole body exposure to ionizing radiation, and is often called radiation sickness. From a physiological standpoint, ARS is a combination of subsyndromes. They appear in stages and are directly related to the level of received dose as given in Figure 03-8 [#505]. These subsyndromes begin to occur within hours after exposure and may last for several weeks. Patients who vomit greater than 4 hours post-accident are likely to have, at worst, a mild acute radiation syndrome. Patients who experience radiation-induced emesis within one hour after a radiation incident require extensive and prolonged medical intervention, and an ultimately fatal outcome is expected in many cases. The median dose for this case is found to be 6.5 Gy with an interquartile (25%-75%) range of approximately 5-11 Gy. 14 Figure 03-9. Median lethal dose as a function of dose rate of whole body exposure Risk models and associated parameters were developed using the available data on animal experiments and analysis of human exposures as described in detail in [#510]. The Figure 03-9 shows the estimated median lethal RBE weighted dose (AD50) to the human relative to the dose rate for humans, based on data collected in [#510] to confirm the risk model for haematopoietic syndrome. This data also illustrates the strong dependence of risk on dose rate: LANGHAM 67 estimates based on linear probit model for exposure for 0–1 day and 1–7 days. HIROSHIMA: estimate for Hiroshima with AD50 dose at about 900 meters from hypocentre; dose estimate modified based on DS86 dosimetry and new transmission factors. MEXICAN FAMILY: Mexican family unknowingly exposed intermittently in their home to orphan 60Co source; 4 out of the 5 died. JAPANESE FISHERMEN: Seven of the 23 fishermen exposed to fallout gamma radiation had estimated total-body doses greater than 4 Gy; none died from marrowsyndrome mode. OTA 80: Judgment of AD50 provided by the Office of Technology Assessment for a one week exposure period. BIR REPORT: Judgment of AD50 provided by the British Institute of Radiology for a one month exposure period (1982). Values of quantitative characteristics of the risk of development the fatal or nonfatal deterministic effects depends on irradiation history presented by time dependence of dose rate [#501], [#511], [#512]. The threshold doses attributing the fatal deterministic effects for brief exposure are presented in the Table 03-8. Table 03-8. Threshold dose of brief exposure Syndrome Critical organ or tissue AD05, Gy Embryo 0–18 d 0.3 Embryo / foetus 18–150 d 0.6 Foetus > 150 d 2 Haematopoietic Red marrow 3 Gastrointestinal Small intestine 12 Embryo or foetal death 15 Syndrome Critical organ or tissue AD05, Gy Soft tissue 25 (a) Necrosis Derma of skin 10 (b) (a) The dose delivered to 100 cm2 at a depth of 0.5 cm under the body surface due to close contact with a radioactive source; (b) The dose is to the 100 cm2 dermis (skin structures at a depth of 40 mg/cm2 (or 0.4 mm) below the surface). Nonfatal deterministic effects of exposure should be taken into account in response to radiological or nuclear emergency. The threshold doses attributing the nonfatal deterministic effects for brief exposure are presented in the Table 03-9. Table 03-9. Nonfatal deterministic effects of external exposure of embryo and foetus Symptom Malformation Possible verifiable reduction in IQ Growth retardation Severe mental retardation Period of embryo / foetus gestation 8-25 weeks 8-25 weeks AD05, Gy 0.1 0.1 8-25 weeks 8-15 weeks 16-25 weeks 0.25 0.6 0.9 The action of penetrating radiation on the whole-body was the main reason of the development of clinical syndromes of ARS such as bone-marrow and intestinal syndromes and their combinations, which are characteristic for dose range 1-16 Gy. Less penetrating, only to the depth of skin, beta irradiation at the doses at least 10 to 20 times higher than average whole-body dose became the cause of the vast radiation injuries of the skin in more than 50% of the patients. These injuries significantly aggravated the clinical course of sickness and greatly influenced the outcomes. Sometimes on the background of shallow radiation injuries, the isolated centres of more deep local radiation injuries (LRI) have arisen because of local application or contact with the objects contaminated by radionuclides such as the wet clothes or boots [#508]. 134 cases of ARS among responders (emergency workers): 28 died in 1986 from a combination of high external doses of -exposure and skin burns due to -emitters 17 died in 1987-2004 from various causes, not all directly linked to radiation No cases of acute radiation syndrome have been recorded among the general public. Table 03-10 presents outcomes of high dose exposure of the Chernobyl emergency workers. Most of fatal deterministic effects in Chernobyl emergency workers were caused by combination of high doses of external exposure to penetrating radiation and spacious skin burns caused by heavy contamination of wet protective closes by fission products, presumably by Ru-106 and Rh-106 [#508]. 16 Table 03-10. Responders with ARS following the Chernobyl accident Degree of ARS Range of whole body RBE weighted dose, Gy Number of patients treated N of deaths Mild (I) 0.8-2.1 41 - Moderate (II) 2.2-4.1 50 1 Severe (III) 4.2-6.4 22 7 Very severe (IV) 6.5-16 21 20 Total 0.8-16 134 28 Stochastic health effects The scientific knowledge about stochastic effects is based on radiobiological research and evaluation of clinical observation of survives of A-bombing of Hiroshima and Nagasaki, and people received significant doses in course of radiation therapy or unintended intake of radioactive material by dial workers and uranium miners in course of work. Stochastic effects could occur at all dose levels because of cell mutations caused by damage to the DNA. A modified cell that is still able to perform mitosis can give rise to a clone of cells that may eventually result in a cancer in the exposed person. Such effects develop in the long term, often decades after the exposure. The probability that effects will occur either in the exposed person (somatic effects) or in descendants (hereditary effects) increases in proportion to a dose. Causation of stochastic effects from exposure to ionizing radiation has a probabilistic character. It is based on comparison of cancer mortality or morbidity for adequate groups of exposed and intact persons. Validity of this approach is limited due to natural fluctuations of cancer morbidity and mortality. So in case of human exposure with very low dose the development of radiation induced cancers additional to natural ones could not be proved and, therefore, detected, because All radiation-induced stochastic effects are similar to those developing in non-irradiated population; There are no signs or characteristics that may indicate that the cancer in the exposed person or hereditary effect in his or her progeny is caused by irradiation; One can only estimate probability of causation of diagnosed effect From the common point of view, initial damaged cell must pass through number of phases for developing malignant tumour from one mutated cell. They are the cell initiation; dysplasia; benign tumour and malignant tumour. These processes are developing in time, so the time between cell initiation and developing radiation induced cancer may be comparable with life span of exposed human or animal. Development of malignant tumour during this time has not any clinical effects and this period is named a latent period of cancer development. Stochastic effect is the radiation-induced health effect, occurring without a threshold level of dose, whose probability is in many cases proportional to the dose and whose severity is independent of the dose. These effects include radiation-induced cancers and hereditary effects, and are characterized by very long period of latent development of the disease after exposure. All radiation-induced stochastic effects are similar to those developing in non-irradiated population. There are no signs or characteristics that may indicate that the cancer in the exposed person or hereditary effect in his or her progeny is caused by irradiation. Stochastic effects are not immediately evident or certain to occur, but the likelihood that they will occur increases as 17 the dose increases as given in Figure 03-6(b). The induction of cancer is recognized as the most important long-term stochastic health effect from emergency exposure of the public. Cancer needs a long period for latent development. The shortest latent period is about several years. The scientific knowledge about stochastic effects is mainly based on evaluation of health status of people survived after atomic bombing of Hiroshima and Nagasaki in 1945. From among about 284 000 A-bomb survivors in both Hiroshima and Nagasaki confirmed by the 1950 national census, a basic cohort called the Life Span Study (LSS) was organized in 1958. It consists of, 1) all of the heavily exposed A-bomb survivors, 2) a selected population of the less exposed, matched by age and sex with the first group, and 3) non-exposed residents of both cities selected on the basis of matched age and sex with the first group, with the total number of study subjects reaching about 120 000. Until 2002, the radiation doses were reconstructed for 86 611 of them. Cancer is a common disease. In economically developed countries, over one third of the population develops cancer at some time during their lives and between one fifth and one-quarter of individuals eventually dies of malignant disease. In addition, cancer is becoming more important as a major cause of disability and death in less developed countries. Epidemiological studies of relatively large populations exposed to significant levels of acute radiation exposure, in particular the studies of the cohort of Japanese survivors of the atomic bombings of Hiroshima and Nagasaki, have established that such exposure can cause most forms of cancer. They have also shown that the excess risk is modified by other factors (such as sex or age at exposure) and how this excess risk is expressed over time. For example, the studies show that the risk of radiation-induced acute leukaemia is significantly greater at younger ages at exposure. The excess risk is manifest as a “wave” over time since exposure, beginning at about two years after exposure, rising to a peak between five and ten years after exposure and then falling away to a low level some 20 years after exposure. Thus, if the convolution of size and dose of an exposed population is large enough, the epidemiological study of such a population allows the number of cases of cancer that may be attributed to irradiation to be determined and how this varies with other factors such as age and gender. Risk models have been developed to describe the expression of radiation-induced cancer risk in terms of important determinants of risk, for example the organ-specific cumulative equivalent dose, from which the excess relative risk may be derived for a particular set of individual circumstances. Here, the excess relative risk is the proportional increase in the risk of the particular cancer that is due to exposure to radiation for the specific set of individual circumstances; this proportional increase is with respect to the background risk of the specific cancer in the absence of the additional dose of radiation [#504]. Table 03-11. Life Span Study mortality (1950-2002) Deaths observed expected excess Attributable fraction Solid cancer 6 718 6 205 513 8.3% Leukaemia 317 219 98 44.7% Diseases The Table 03-11 presents data of 52 years follow-up of the atomic bomb survivors to among these people, the leukaemia incidence started to increase two years after exposure and then gradually faded. The maximum increase occurred less than ten years after exposure. In contrary, the incidence for solid tumours started to increase later, about 5 years after exposure, but the 18 increase is still going on and seems to continue to the end of life. It is actually accentuated when the exposed population gets older and natural cancer incidence increases. In 2002, the Dosimetry System 2002 was completed [#513]. It contains the reassessment of the atomic bomb radiation dosimetry for Hiroshima and Nagasaki. It includes records of 86 611 people with evaluated dose. Among them 38 509 with Colon dose < 5 mSv (mean = 0.2 mSv) and 37 401 with Red marrow dose < 5 mSv [#514]. A substantial increase in thyroid cancer incidence has occurred in the three republics (the whole of Belarus and Ukraine, and the four most affected regions of the Russian Federation) since the Chernobyl accident among those exposed as children or adolescents. Between 1991 and 2005 the 5,127 cases of thyroid cancer were reported amongst those under age 14 years in 1986, and 6,848 cases amongst those under age 18 years in 1986. It was demonstrated, that in Belarus, after the Chernobyl accident in 1986, thyroid cancer incidence rates among children under age of 10 years increased dramatically in comparison with pre-Chernobyl level and subsequently declined, specifically for those born after 1986. This pattern suggests that the increase in incidence in 1991-1995 was associated with the accident. The increase was primarily among the children under age 10 years at the time of the accident. For those born after 1986, there was no evidence for an increase in the incidence of thyroid cancer. The increase in the incidence of thyroid cancer among children and adolescents began to appear about 5 years after the accident and persisted up until 2005. The background rate of thyroid cancer among children under age 10 years is approximately 2 to 4 cases per million per year. Table 03-12. Thyroid dose in entire population at affected territory in 1986 Persons in age group Quantity 0-17 y Adults All ages Total 26,330,000 71,576,000 97,896,000 Hthy< 50 mSv 23,032,000 68,319,000 91,351,000 Hthy > 50 mSv 3,288,000 (12.5 %) 3,257,000 (4.6 %) 6,545,000 (6.7 %) Estimates for the dose to the thyroid are presented in Table 03-12 [#520] for four age categories and the total population according to the region/oblast or city of residence and for contaminated areas of the three countries (all of Belarus and Ukraine and 19 regions of the Russian Federation). The estimates of the collective dose to the thyroid are presented according to 8 individual dose intervals, ranging from less than 0.05 Gy to more than 5 Gy. The Figure 03-10 presents thyroid cancer incidence rate among those exposed as children and adolescents (age under 18 years in 1986) in Belarus [#564], [#565]. 19 Figure 03-10. Thyroid cancer incidence in 1986-2002 among Belarusians of 18 years old and younger in 1986. Linear Non-Threshold hypothesis Until now, biological markers of radiation-induced cancer were not found. Therefore, the only way to confirm the risk estimates is to use an epidemiological investigation of the affected population. Power of epidemiological consideration depends on the number of the affected population, expected number of excess radiation-induced cancers, background level of the same type of cancer and on a variation of this background level in population equivalent to the one under study. The number of excess radiation-induced cancers depends on the exposure dose, time of the follow-up, and size of the affected group (sample size of the irradiated and controlled cohorts). Contribution of total cancer mortality to the mortality statistics in developed countries is about 20-30%. This high level of background cancer incidence is characterized by a wide variation. It is similar to year-by-year variation of total annual mortality, which can be higher than 3%. The nature of these variations is not clear, but it is much higher than expected statistical fluctuations of background level of cancer mortality. Radiogenic and natural cancers are similar and the only way to detect excess cancers in exposed group is to compare cancer incidence in it with that in control group. The control and exposed groups must have the same age and gender composition. The simplest way to detect this difference is to apply common methods of mathematical statistics to results of the epidemiology of cancer in given groups. It is assumed in this approach, that the groups are composed of individuals for whom development of a cancer is a random Poisson process, and Poisson distribution [#517] describes cancer incidence. In this assumptions level of detectability of difference between two groups is the only matter of number of “items” in control and affected group. The similar approach is used in nuclear physics when activity of a sample is measured in presence of background contamination. 20 Figure 03-11. Non-Poisson variation of annual mortality in France. Number of people in study and control cohorts Reality is more complicated than simple statistical model. The Poisson distribution could not present the statistics of total and cancer mortality. The Figure 03-11 presents the effect of 4% variation of total mortality in thousands death per year in 100,000 people observed in France with total population of 55,000,000 inhabitants in 1976-2000 [#516]. Non-Poisson variation of background cancer mortality is similar to that presented in Figure 03-11 and could not be reduced by expanding the number of people in examined cohort. Because of non-Poisson variation of cancer mortality, the excess radiation induced cancers could not be detected in exposed cohort if their level does not exceed 4% of the background level. These variations and a high level of background incidence, which is about 25% in developed countries, are the major factors limiting the statistical power of epidemiological investigations. The statistically determined sample size of the irradiated and controlled cohorts needed to detect a significant increase in total cancer risk from whole body exposure of 100 mSv is about 100,000 (of each cohort) [#511]. Area of detectability Equivalent dose in whole body, Sv Figure 03-12. Statistical limitation of detectability of stochastic health effects in exposed population. Therefore, threshold of detectability is an average dose of public exposure that, if exceeded, leads to an additional (above the background level) total number of stochastic health effects in the irradiated population that theoretically may be confirmed by means of current epidemiological methods with a 95% level of confidence. For the case of developing any cancer excluding leukaemia and thyroid cancers, the epidemiological estimate of number of people in study and control group, which is needed to detect an increase in solid cancer mortality in case of brief whole body exposure to penetrating radiation, is shown in Figure 03-12: N 10 9 H WB 2 , H WB 100 mSv , (03- 9) 21 where H WB is the whole body equivalent dose in mSv. Value of N could not be defined if H WB 100 mSv [#518]. Considering a 4% variation of background mortality with time, which has a non-statistical nature as discussed earlier, whole body exposure of 100 mSv should be treated as the minimal level of exposure which cause a detectable increase of cancer incidence [#516]. This level cannot be decreased by simply expanding the control of test groups as discussed above. The conclusion of the UNSCEAR regarding detectability of radiogenic cancers [#519], [#520], [#521] supports that evaluation of threshold for detectability of increase of a number of all cancers in case of uniform exposure of people, when all internal organs are exposed to the same dose. The concept of detectability of radiation-induced cancer is also valid for a case of exposure of a single organ, e.g. thyroid after intake of I-131 or red marrow after intake of Sr-90. For such case the level of detectability will be another then for case of whole body exposure as show in Ref. [#511]. The undetectability of radiation induced health effects at low doses raised up in 1970-s, when the firs lessons were learning from Life Span Study of A-bomb survives. In the same time, the need to have some simple instrument to assess risks of exposure to low doses became actual because of significant improvement of working conditions in radiation industry, and decrease of individual doses of radiation workers worldwide. To solve the problem, the ICRP introduced the Linear Non-Threshold (LNT) hypothesis of developing the stochastic health effects. The LNT was formulated in paragraph 27 of the 1977 Recommendations of the ICRP [#523] as follows. (27) ... For radiation protection purposes it is necessary to make certain simplifying assumptions. One such basic assumption underlying the Commission’s recommendations is that, regarding stochastic effects, there is, within the range of exposure conditions usually encountered in radiation work, a linear relationship without threshold between dose and the probability of an effect. LNT proposes that the risk of stochastic effects is directly proportional to the dose for all levels of dose and dose rate (below those at which deterministic effects occur). It stats that any nonzero dose implies a non-zero risk of stochastic effects. This is the working hypothesis on which the IAEA safety standards (and ICRP’s Recommendations) are based. It is not proven — indeed, it is probably not provable — for low doses and dose rates, but it is considered the most defensible assumption on which to base safety standards. The 1977 Recommendations of the ICRP [#515] were superseded by 1990 Recommendations of the ICRP [#552] and then by 2007 Recommendations of the ICRP [#522], but the key concept based on the Linear Non-Threshold (LNT) hypnosis was remained unchanged. This paragraph 27 of the ICRP publication 26, several hundreds of words, is the only technical basis for assessment the radiation risks in a very low dose area, below 10 mSv of whole body equivalent dose. However, this hypothesis plays the key role in framework of radiation protection. Concept of a dose as the only characteristic of exposure, which is needed for risk assessment is most valuable conclusion the Linear Non-Threshold hypnosis. The “summation” concept is, and will be a technical bass for radiation protection dosimetry in low dose area. 22 Figure 03-13. Use of Linear non-threshold hypothesis Thus, although proof of development of additional cancers at small doses is not found, it has been accepted, that the increase of frequency of development of stochastic effects in group of equally irradiated people is proportion to any dose received by them above the normal background. The Figure 03-13 is an illustration of such dependence. It shows increment of risk of development of any cancer after exposure as a function of increment of equivalent dose in whole body. Thus, it is assumed that there is no dose threshold below which stochastic effects do not occur. The LNT hypothesis results in a highly overestimated estimation of danger due to low doses. The accepted decision entirely is caused by the desire to simplify methods for estimation values of small doses in organs or tissues and thus to secure the personnel and the public from possible radiation induced risk even at those levels of an exposure at which development of radiation health effects is not proved yet. Likelihood of harmful effect The radiation protection dosimetric quantities of RBE weighted organ dose, equivalent organ dose and effective dose might be calculated for any exposure conditions, but each of these quantities was invented for use in only certain field of exposure assessment. The field of exposure assessment is the range of exposure conditions, which could be properly characterized in terms of considered dosimetric quantity to evaluate the likelihood of harmful radiation health effect. Figure 03-14 provides an example of the field of exposure assessment of these quantities in event of brief exposure to external penetrating radiation. Equivalent dose in whole body, Sv Figure 03-14. Probability of severe health effects as a function of brief exposure of whole body to external penetrating radiation. 23 The fields are not exactly distinguished. For instance, the development of radiogenic cancers and severe deterministic effects have to be considered when determining risk of harmful health effects if the equivalent whole body dose is around 1-2 Sv. For this exposure conditions the equivalent organ dose has to be determined to evaluate the risk of development of stochastic effects and RBE weighted organ dose – to evaluate the risk of development of deterministic effects. Characterization of those exposure conditions in terms of effective dose will be nonproductive. Analogously, characterization of low dose brief exposure in terms of RBE weighted organ dose will be also non-productive. Therefore, In case of high dose exposure, when the equivalent dose in whole body is greater than 2 Sv, contribution of stochastic effects to total probability of premature death is negligible, and only the RBE weighted dose should be used as the characteristic of human exposure in that field of exposure assessment; In the case, when the equivalent dose in whole body is in the range of 1-2 Sv, contribution of deterministic and stochastic effects to total probability of premature death is comparable, and it is reasonable to use equivalent organ dose and RBE weighted organ dose as the characteristics of human exposure in that field of exposure assessment; In case of intermediate dose exposure, when the equivalent dose in whole body is in the range of 1-0.1 Sv, contribution of deterministic effects to total probability of premature death is negligible, and it is reasonable to use only equivalent organ dose as the characteristics of human exposure in that field of exposure assessment; In case of low dose exposure, when the equivalent dose in whole body is less than 0.1 Sv, the development of undetectable effects is expected, so the effective dose is usually in use as the characteristic of human exposure in that field of exposure assessment to set limitations for human’s exposure. 24 REFERENCES [#501] FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS, INTERNATIONAL ATOMIC ENERGY AGENCY, INTERNATIONAL LABOUR ORGANIZATION, PAN AMERICAN HEALTH ORGANIZATION, WORLD HEALTH ORGANIZATION, Criteria for Use in Preparedness and Response for a Nuclear or Radiological Emergency, IAEA Safety Standards Series No. GSG-2, IAEA, Vienna (2011). [#502] INTERNATIONAL ATOMIC ENERGY AGENCY, Radiation Protection and Safety of Radiation Sources: International Basic Safety Standards. Interim edition, General Safety Requirements Part 3, Safety Standard Series No. GSR Part 3 (Interim), IAEA, Vienna (2011). [#503] INTERNATIONAL ATOMIC ENERGY AGENCY, The Radiological Accident in Samut Prakarn, IAEA, 2002 [#504] INTERNATIONAL ATOMIC ENERGY AGENCY, INTERNATIONAL LABOUR ORGANIZATION, WORLD HEALTH ORGANIZATION, Approaches to attribution of detrimental health effects to occupational ionizing radiation exposure and their application in compensation programmes for cancer: A practical guide / edited by Shengli Niu, Pascal Deboodt, Hajo Zeeb. Occupational Safety and Health Series, No. 73, Geneva, ILO, 2010 [#505] Cerveny T. J., MacVittie T. J., and Young, R. W., Acute radiation syndrome in humans In: Walker RI, Cerveny TJ (eds.) Medical Consequences of Nuclear Warfare, Part I, Vol. 2. In: Zajtchuk R, Jenkins DP, Bellamy RF, Ingram VM (eds.) Textbook of Military Medicine. Falls Church, VA: Office of the Surgeon General, Department of the Army, USA, 1989, 17-36. [#506] Biodosimetry Assessment Tool (BAT) Version 0.7.5 Beta, Rev. A 23 May 2002. Armed Forces Radiobiology Research Institute, Bethesda, MD, USA. [#507] U.S. DEPARTMENT OF HOMELAND SECURITY, Dirty Bombs. Radiological Dispersal Device (RDD) Dirty Bomb Medical Preparedness and Response: Guidance for First Responders and Health Care Workers - Radioactive Illnesses, Radiation Injuries, Decontamination, U.S. Department of Homeland Security, 2011. [#508] Gus'kova A.K., Nadezhina N.M., Barabanova A.V., Baranov A.E., Gusev I.A., Protasova T.G., Boguslavskij V.B. and Pokrovskaya V.N., Acute effects of radiation exposure following the Chernobyl accident: immediate results of radiation sickness and outcome of treatment. In Medical aspects of the Chernobyl accident (Proceedings of the conference in Kiev 11-13 May, 1988). Vienna: IAEA; Technical Document Series No 516: 233-256; 1989. [#509] INTERNATIONAL ATOMIC ENERGY AGENCY, Lessons Learned from the Response to Radiation Emergencies (1945-2010), Emergency Preparedness and Response Series EPR-LESSONS LEARNED, IAEA, Vienna (2012) [#510] Abrahamson, S., Bender, M.A., Boecker, B.B., Gilbert, E.S. and Scott, B.R. Health Effects Models for Nuclear Power Accident Consequence Analysis. Modification of Models Resulting From Addition of Effects of Exposure to Alpha-Emitting Radionuclides. Part II: Scientific Bases for Health Effects Models. NUREG/CR-4214 Rev. 1, Part II Addendum 2 LFM-136 (1993). 25 [#511] INTERNATIONAL ATOMIC ENERGY AGENCY, WORLD HEALTH ORGANIZATION, Development of extended framework for emergency response criteria Interim guidance for comments. IAEATECDOC-1432, IAEA, Vienna (2005). [#512] INTERNATIONAL ATOMIC ENERGY AGENCY, Dangerous Quantities of Radioactive Material, Emergency Preparedness and Response Series EPR-D-VALUES, IAEA, Vienna (2006). [#513] Reassessment of the Atomic Bomb Radiation Dosimetry for Hiroshima and Nagasaki – Dosimetry System 2002. Radiation Effects Research Foundation, 2005. [#514] A long-term cohort study on the A-bomb survivors of Hiroshima and Nagasaki, recent results and a future scope. Toshiteru Okubo, Chairman of Radiation Effects Research Foundation, Hiroshima and Nagasaki, Japan. Materials presented in the IAEA. October 2009. [#515] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, Recommendations of the International Commission on Radiological Protection. ICRP Publication 26. Ann ICRP Vol 1, No 3 (1977). [#516] Libmann J. Elements of nuclear safety. IPSN, Paris (1996). [#517] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and Effects of Ionizing Radiation. UNSCEAR 2006 Report to the General Assembly with Scientific Annexes. Annex A. Epidemiological studies of radiation and cancer. New York, United Nations (2006). [#518] González A.J. The radiological health consequences of Chernobyl: the dilemma of causation. Symposium on Nuclear Accidents. In: Nuclear accidents: Liabilities and guarantees: Proceedings of the Helsinki symposium, OECD Nuclear Energy Agency (1993). [#519] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and Effects of Ionizing Radiation. UNSCEAR 2000 Report to the General Assembly with Scientific Annexes. Annex G. Biological effects at low radiation doses. New York, United Nations (2000). [#520] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION, Sources and Effects of Ionizing Radiation. UNSCEAR 2010 Report to the General Assembly. New York, United Nations (2011). [#521] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION, Sources and Effects of Ionizing Radiation. UNSCEAR 2012 Report to the General Assembly, New York, United Nations (2012). [#522] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103, Ann ICRP 37(2-4), Elsevier (2007). [#523] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, Recommendations of the International Commission on Radiological Protection. ICRP Publication 26, Ann ICRP 1(3), Pergamon Press, Oxford, UK (1977). [#530] KUTKOV V., BUGLOVA E., and MCKENNA T. Severe deterministic effects of external exposure and intake of radioactive material: basis for emergency response criteria, J. Radiol. Prot. 31, 237–253 (2011). [#531] INTERNATIONAL ATOMIC ENERGY AGENCY, Actions to Protect the Public in an Emergency due to Severe Conditions at a Light Water Reactor, Emergency Preparedness 26 and Response Series EPR-NPP PUBLIC PROTECTIVE ACTIONS, IAEA, Vienna (2013). [#532] MCKENNA T., KUTKOV V., VILAR WELTER P., DODD B., and BUGLOVA E. Default operational intervention levels (OILs) for severe nuclear power plant or spent fuel pool emergencies. Health Phys. 104 (2013) 459-470. [#533] U.S. NATIONAL ACADEMIES/NATIONAL RESEARCH COUNCIL, Health effects of exposure to low levels of ionizing radiation, BEIR V, National Academy Press, Washington. D.C. (1996) [#534] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, Pregnancy and Medical Radiation. ICRP Publication 84. Ann ICRP Vol. 30 No. 1, Pergamon Press, Oxford, UK (2000). [#535] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION, Sources and effects of ionizing radiation. UNSCEAR 1993 Report to the General Assembly with Scientific Annexes. Annex G. Hereditary effects of radiation, New York, United Nations (1993). [#536] KUTKOV V. A., DEMIN V. F. and GOLIKOV V. Ya., Standardization for ionizing radiation, Atomic Energy 85(2), 589-594, New York: Springer (1998). [#537] INTERNATIONAL NUCLEAR SAFETY ADVISORY GROUP, Defence in Depth in Nuclear Safety, INSAG-10, IAEA, Vienna (1996). [#538] KUTKOV V., KOCHETKOV O. and PANFILOV A., Strategy of control at source as a base for protecting workers against risks arising from exposure to ionizing radiation in the Russian Federation. In: Occupational Radiation Protection: Protecting Workers against Exposure to Ionizing Radiation, Int. Conf., 26-30 August 2002, Geneva, Switzerland, IAEA-CN-91/126, 39 – 44, CD-ROM Contr. Papers, Vienna, IAEA, (2003). [#539] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and effects of ionizing radiation. UNSCEAR 2000 Report to the General Assembly with Scientific Annexes. Annex B. Exposures from natural radiation sources, New York, United Nations (2000). [#540] FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS, INTERNATIONAL ATOMIC ENERGY AGENCY, INTERNATIONAL LABOUR ORGANIZATION, OECD NUCLEAR ENERGY AGENCY, PAN AMERICAN HEALTH ORGANIZATION, UNITED NATIONS OFFICE FOR THE COORDINATION OF HUMANITARIAN AFFAIRS, WORLD HEALTH ORGANIZATION, Preparedness and Response for a Nuclear or Radiological Emergency, IAEA Safety Standards Series No. GS-R-2, IAEA, Vienna (2002). [#541] U.S. NATIONAL COUNCIL ON RADIATION PROTECTION AND MEASUREMENTS, Considerations regarding the unintended radiation exposure of the embryo, foetus or nursing child, NCRP Commentary 9, Bethesda, NCRP (1994). [#542] U.S. NATIONAL COUNCIL ON RADIATION PROTECTION AND MEASUREMENTS, Potential impact of individual genetic susceptibility and previous radiation exposure on radiation risk for astronauts, NCRP Report 167, Bethesda, NCRP (2010). [#543] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, Biological Effects after Prenatal Irradiation (Embryo and Fetus), ICRP Publication 90, Ann ICRP Vol. 33(1-2), Pergamon Press, Oxford, UK (2003). 27 [#544] U.S. NATIONAL COUNCIL ON RADIATION PROTECTION AND MEASUREMENTS, Uncertainties in the Estimation of Radiation Risks and Probability of Disease Causation, NCRP Report 171, Bethesda, NCRP (2012). [#545] DOUPLE et al., Long-term radiation-related health effects in a unique human population: Lessons learned from the atomic bomb survivors of Hiroshima and Nagasaki, Disaster Med. Public Health Prep. 5 (Suppl 1), S122–S133 (2011). [#546] PRESTON et al., Solid cancer incidence in atomic bomb survivors exposed in utero or as young children, J. Natl. Cancer Inst. 100(6), 428–436 (2008). [#547] U.S. NATIONAL ACADEMIES/NATIONAL RESEARCH COUNCIL. Health Risks from Exposure to Low Levels of Ionizing Radiation, BEIR VII, Phase 2, National Academies Press, Washington. D.C. (2006). [#548] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and effects of ionizing radiation. UNSCEAR 2001 Report to the General Assembly with Scientific Annexes. Annex. Hereditary effects of radiation, New York, United Nations (2001). [#549] U.S. NATIONAL COUNCIL ON RADIATION PROTECTION AND MEASUREMENTS, Radiation dose management for fluoroscopically-guided interventional medical procedures, NCRP Report 168, Bethesda, NCRP (2010). [#550] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION, Sources and effects of ionizing radiation. UNSCEAR 1993 Report to the General Assembly with Scientific Annexes. Annex F. Influence of dose and dose rate on stochastic effects of radiation, New York, United Nations (1993). [#551] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, ICRP Statement on Tissue Reactions / Early and Late Effects of Radiation in Normal Tissues and Organs – Threshold Doses for Tissue Reactions in a Radiation Protection Context. ICRP Publication 118, Ann. ICRP Vol. 41 No 1-2, Elsevier (2012). [#552] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, 1990 Recommendations of the International Commission on Radiological Protection, ICRP Publication 60, Ann ICRP, Vol. 21, No 1-3 (1991). [#553] Cohen B. L. and Lee I. S., Catalogue of Risks Extended and Updated, Health Physics, Vol. 61, 317 (1991). [#554] FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS, INTERNATIONAL ATOMIC ENERGY AGENCY, INTERNATIONAL LABOUR ORGANIZATION, OECD NUCLEAR ENERGY AGENCY, PAN AMERICAN HEALTH ORGANIZATION, UNITED NATIONS OFFICE FOR THE COORDINATION OF HUMANITARIAN AFFAIRS, WORLD HEALTH ORGANIZATION, Preparedness and Response for a Nuclear or Radiological Emergency, IAEA Safety Standards Series No. GSR Part 7, IAEA, Vienna (2015)<to be updated>. [#555] INTERNATIONAL ATOMIC ENERGY AGENCY, WORLD HEALTH ORGANIZATION, Generic Procedures for Medical Response During a Nuclear or Radiological Emergency, Emergency Preparedness and Response Series, EPRMEDICAL, IAEA, Vienna (2005). [#556] INTERNATIONAL ATOMIC ENERGY AGENCY, PAN AMERICAN HEALTH ORGANIZATION, WORLD HEALTH ORGANIZATION, Cytogenetic Dosimetry: Applications in Preparedness for and Response to Radiation Emergencies, Emergency Preparedness and Response Series, EPR-BIODOSIMETRY, IAEA, Vienna (2011). 28 [#557] INTERNATIONAL ATOMIC ENERGY AGENCY, INTERNATIONAL LABOUR ORGANIZATION, Occupational Radiation Protection. IAEA Safety Standards Series No. <DS453>, IAEA, Vienna (2015)<to be updated> [#558] INTERNATIONAL COMMISSION ON RADIATION UNITS AND MEASUREMENTS, Quantities and Units in Radiation Protection Dosimetry, ICRU Report 51, ICRU, Bethesda (1993). [#559] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION. Relative Biological Effectiveness (RBE), Quality Factor (Q) and Radiation Weighting Factor (wR). ICRP Publication 92. Ann ICRP Vol.33 No.4. Pergamon Press, Oxford, UK (2003). [#560] US NUCLEAR REGULATORY COMMISSION, EVANS, J.S., ABRAHAMSON, S., BENDER, M.A., BOECKER, B.B., GILBERT, E.S. and SCOTT, B.R. Health Effects Models for Nuclear Power Accident Consequence Analysis. Part I: Introduction, Integration, and Summary. NUREG/CR-4214 Rev. 2, Part I ITRI-141 (1993). [#561] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, Protection of the Public in Situations of Prolonged Radiation Exposure. ICRP Publication 82, Ann ICRP Vol. 29 No. 1-2. Pergamon Press, Oxford, UK (2000). [#562] EUROPEAN ATOMIC ENERGY COMMUNITY, FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS, INTERNATIONAL ATOMIC ENERGY AGENCY, INTERNATIONAL LABOUR ORGANIZATION, INTERNATIONAL MARITIME ORGANIZATION, OECD NUCLEAR ENERGY AGENCY, PAN AMERICAN HEALTH ORGANIZATION, UNITED NATIONS ENVIRONMENT PROGRAMME, WORLD HEALTH ORGANIZATION, Fundamental Safety Principles, IAEA Safety Standards Series No. SF-1, IAEA, Vienna (2006). [#563] INTERNATIONAL NUCLEAR SAFETY ADVISORY GROUP, Defence in Depth in Nuclear Safety, INSAG-10, IAEA, Vienna (1996). [#564] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and Effects of Ionizing Radiation. UNSCEAR 2000 Report to the General Assembly with Scientific Annexes. Annex J. Exposures and effects of the Chernobyl accident. New York, United Nations 2000. [#565] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and Effects of Ionizing Radiation. UNSCEAR 2008 Report to the General Assembly with Scientific Annexes. Annex D. Health effects due to radiation from the Chernobyl accident. New York, United Nations 2011. [#566] Ghiassi-NEJAD M., MORTAZAVII S.M.J., CAMERON J. R., NIROOMAND-RAD A., and KARAM P. A., “Very High Background Radiation Areas of Ramsar, Iran: Preliminary Biological Studies,” Health Physics 82, no. 1, 2002: 87–93. [#567] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and Effects of Ionizing Radiation. UNSCEAR 1994 Report to the General Assembly with Scientific Annexes. Annex B: Adaptive responses to radiation in cells and organisms. New York, United Nations 1994. [#568] LUCKEY T. D. 2007. Documented optimum and threshold for ionizing radiation, Int. J. Nuclear Law, 1, p. 378-409 [#569] Cohen B. L., Catalog of Risks Extended and Updated, Health Physics, Vol. 61 (1991) 317. [#570] INTERNATIONAL ATOMIC ENERGY AGENCY, Safety Assessment and Verification for Nuclear Power Plants. IAEA Safety Standards Series No. NS-G-1.2, IAEA, Vienna (2001). 29