Response to Reviewer 2 comment No. 1

Reviewer 1
Reviewer’s report
1.
A reference for the ethical clearance should be included, not just a general
Statement.
Response Reviewer 1 comment No. 1:
This study was part of a larger vaccination study, performed in the Delta Amacuro in
2012 . Detailed information of the ethical approval for this study has been added at the Methods section after ‘…The nature and objectives of the study were explained to the parents of children in Spanish and/or in their native language.
’:
‘This study was a pilot study within a larger study on response to pneumococcal vaccination which was approved by the ethical committee of the Instituto de
Biomedicina, Caracas 1010A, issued on the 22th of March 2011 in Caracas,
Venezuela. Furthermore, the study was approved by the Servicio de Atención y
Orientación Indígena (S.A.O.I) on the 2th of December 2010 in Tucupita, Venezuela.’
2.
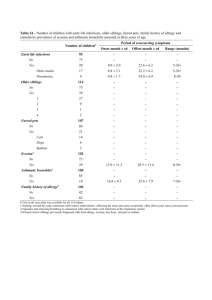
A table detailling the parasitological findings would be interesting, as most epidemiological studies docus only on helminths and data on protozoa are very scarce
Response Reviewer 1 comment No. 2:
We agree that is interesting to show the details of the parasitological findings since data on prevalence rates of these pathogens are indeed scarce. We added the detailed prevalences of helminth and protozoan infections, which were observed with both microscopy and PCR, in table 1.
3.
lamblia should be consequently written in miniscules.
Response Reviewer 1 comment No. 3:
We want to thank the reviewer for noticing. Due to spell-check errors some letters were changed into capitals. We changed all the lamblia’s with capitals in the entire article to miniscules again.
Level of interest: An article whose findings are important to those with closely related research interests
Quality of written English: Acceptable
Statistical review: No, the manuscript does not need to be seen by a statistician.
Declaration of competing interests:
I declare that I have no competing interests
Reviewer 2
Reviewer’s report
Objective:
1.
In the abstract and introduction the research question is formulated as ” We performed a cross-sectional survey to study the association of helminth and protozoan infections with atopic eczema and recurrent wheezing in Warao
Amerindia n children aged 0 to 2 years.”
However in the methods section it seems as if there was a different approach:”To determine which characteristics were associated with atopic eczema and recurrent wheezing, multivariate logistic regression models were built. Only variables with a p-value <0.20 in univariate analyses were considered as candidates for the multivariate model …..”
This latter approach gives the impression that a prediction model was built.
However if the authors meant to built a prediction model then I the method section should be expanded to show how the prediction model was built (i.e. was a forward or a backward approach used? What is the AUC etc).
On the other hand: If the authors meant to study the association between helminth and protozan infections and atopic asthma and recurrent wheezing a different statistical analysis should have been performed.
Please clarify as this is a fundamental issue. Also please change the objective in either the objective or methods section accordingly as well as the whole paper.
For example in the abstract the conclusion and objective do not match:
“Objective: a cross-sectional survey to investigate the association between helminth and protozoan infections and recurrent wheezing and atopic eczema in Warao
Amerindian children in Venezuela.”
While the conclusion is:
“High prevalence rates of atopic eczema and recurrent wheezing in Warao
Amerindian children under 2 years of age were related to stunting and intestinal protozoan infections respectively.” (stunting was not part of the research question under investigation according to the stated objective)
Response to Reviewer 2 comment No. 1:
We agree with the reviewer that the objectives of this study are not clearly presented.
Malnourishment was from the beginning one of the objectives, which was not mentioned in the abstract and the introduction. We added malnutrition to the objective, so that the objective and conclusion match in the revised version of our manuscript. [25] Furthermore, we added the following paragraph describing the reason for including malnourishment as one of the objects of interest in our study to the Introduction section:
‘Helminthiasis and giardiasis in school-age Venezuelan children were associated with acute and chronic nutritional status respectively. [25] The vicious cycle of malnutrion and parasitic infections is associated with immune modulation. A disturbed immune
balance may play a role in the development of immune-mediated diseases like atopy
.’
In order to have an adequate power, a study using a prediction model requires a minimum of 100 events and 100 non-events. (Vergouwe Y, Steyerberg EW,
Eijkemans MJC, Habbema JDF: Substantial effective sample sizes were required
for external validation studies of predictive logistic regression models. Journal
of Clinical Epidemiology 2005;58:475
–483.) Although we included 229 children in our survey, there are a few subpopulations within this study. For example, recurrent wheezing ( in children ≥ 12 months) was measured in 128 children, with 23 events and 95 non events (table 2b). Also, the number of stool samples collected was only
100 of 229. As said in the Methods, our study is a pilot-study to study associations between atopic eczema, recurrent wheezing, parasitic infections and malnourishment. Larger studies are required to built predictions models.
Thanks to the very relevant suggestion of the reviewer, we adapted our statistical analyses. Because we performed an association study, we now performed univariate analyses for all variables measured. Subsequently, a multivariable analyses was performed in which we included all variables that formed part of the study objectives irrespective of their p-value in univariate analysis (i.e. Atopic eczema, recurrent wheezing, malnourishment, protozoan infections and helminth infections) as well as age and sex if p < 0.20.
We added information on this statistical analysis to the methods section:
‘Categorical variables were analyzed using univariate analysis. To determine which characteristics were associated with atopic eczema and recurrent wheezing, multivariable logistic regression models were built. The variables of interest (i.e. atopic eczema, recurrent wheezing, malnutrition, protozoan infections and helminth infections) were included in the multivariable model irrespective of their p-values in the univariate analysis. Age and gender were included in the multivariable model if p
<0.20 in univariate analyses. Statistical analyses were performed using the SPSS program for Windows version 20.0 (SPSS Inc, Chicago, IL).’
Additionally, we added a sentence in acknowledgements to acknowledge the advice on statistical analyses we received from statistician J in 't Hout:
’Finally we thank
Joanna in ‘t Hout for her professional statistical assistance.’
Introduction:
2.
“Atopic disorders comprise a range of allergic diseases including asthma, anaphylaxis, allergic rhinitis and atopic eczema.”
Asthma is not necessarily an allergic disease (please read: Moncayo et al., 2010
Risk factors for atopic and non-atopic asthma in a rural area of Ecuador) this could have implications for this research.
Response to Reviewer 2 comment No. 2:
We agree with the reviewer that asthma is not necessarily an allergic disease. Also wheezing is not necessarily an atopic disease. In the INTRODUCTION section we therefore we changed the sentence from
“Atopic disorders comprise a range of allergic diseases including asthma, anaphylaxis, allergic rhinitis and atopic eczema.” to “Atopic disorders comprise a range of allergic diseases including allergic asthma, anaphylaxis, allergic rhinitis and atopic eczema.”
In the discussion section, we also provide information of atopic and non-atopic wheezing. We added a part of the article of Moncayo et al 2010 in this section after ‘….Atopy as measured by skin prick tests and atopic dermatitis in infancy has also been identified as a predictor for the subsequent development of asthma.’
‘Another study among schoolchildren living in a poor rural region of tropical Latin
America, showed a predominance of non-atopic compared with atopic wheeze. However the subjects of this study were between 6 and 16 years old and thus not comparable to our study population. [54] ‘
3.
I would be gratefull if the authors could explain why this sentence is relevant to this article:
The hygiene hypothesis is consistent with the extremely high prevalence of asthma in Tristan da Cunha [12, 13] and the Western Carolinas [14, 15], two isolated, highly inbred island communities with a low incidence of respiratory and other viral infections.
Response to Reviewer 2 comment No. 3:
This sentence was meant as an example of communities which support that diminished microbial exposure during early childhood increases susceptibility to allergic diseases. In these two communities the incidence of viral and respiratory infections in early childhood are low and the prevalence of asthma is very high.
These findings are in line with the hygiene hypothesis. Relating to this article, the
Warao community also is an isolated, highly inbred island community and therefore we expect to find low prevalences of allergic diseases as the prevalences of viral and respiratory infections are very high (Verhagen LM, Warris A, Hermans PWM, del
Nogal B, de Groot R, de Waard JH: High Prevalence of Acute Respiratory Tract
Infections Among Warao Amerindian Children in Venezuela in Relation to Low
Immunization Coverage and Chronic Malnutrition. The Pediatric Infectious
Disease Journal 2012; 31 (3).) As the reviewer has noticed, we did not connect these expectations in the introduction section. Therefore, lacking its relevance for this article, we deleted this sentence from the introduction.
Methods section:
4.
Data collection:
“Warao Amerindian children aged between 0 and 2 years from 11 villages that are geographically spread throughout the Orinoco Delta were included in a crosssectional survey.”
So this is not a random sample, please comment on the effects this may have on the conclusions being drawn in the limitations section.
Response to Reviewer 2 comment No. 4:
To give a more detailed explanation of the location of the study communities, we changed the main text in the METHODS section by adding the municipality where the study took place.
‘The Delta Amacuro or Orinoco Delta comprises 4 municipalities. This cross-sectional survey was undertaken in 11 geographically spread isolated Warao villages, located in the largest of the 4 municipalities, Antonio Diaz, which has almost 19,000 inhabitants. Warao Amerindian children aged between 0 and 2 years were included.’
The 11 villages were geographically spread throughout the municipality, but indeed, we did not officially randomize the selection of the villages. There were no nonresponders in this study and every child in this age category was included. There may have been confounding of recurrent wheezing prevalences if there were epidemic viral infections at the time of survey, leading to overreporting of recurrent wheezing. We added this possibility at the DISCUSSION section.
‘Additionally, although included villages were chosen to be geographically spread throughout t he Antionio Díaz municipality, no randomization procedure was performed for the selection of villages. If reported wheezing episodes were related to viral infections, substantial variation between communities in the prevalence of recurrent wheezing could be associated with the rapid spread of viral infections within communities. Because most Warao people live with several families together in one house, viral infections spread rapidly, leading to a rise in overall prevalence when a few community members bec ome infected.’
5.
“A physical examination including anthropometric measurements of the child and inspection of the skin was performed and documented on a standardized data collection sheet.”
Please elaborate on how anthropometric meaurements were taken.
Response to Reviewer 2 comment No. 5:
To clarify how the anthropometric measurements were taken, we added the following sentences to the METHODS section: ‘’Children were measured for height and weight without shoes and in light indoor clothing using a tape measure with a precision to
0.1 cm. Weight was measured using an electronic digital scale, with a maximum capacity of 150 kg and a precision to 0.1 kg.’’
Statistical analysis:
6.“
Only variables with a p-value <0.20 in univariate analyses were considered as candidates for the multivariate model.”
The way the model is explained it appears to me that many predictors/determinants are used to built a model: in this case the term multivariable should be used. The term multivariate regression refers to cases were there is more than one outcome.please explain (I would recommend to read
Multifarious terminology: multivariable or multivariate?cunivariable or univariate?
Peter 2008)
Response to Reviewer 2 comment No. 6:
We thank the reviewer for noticing that the term multivariate was being used wrongly.
After reading the article of Peter, 2008 and after consultation of a statistician (J. in ‘t
Hout, Radboud University Nijmegen) we agree that the term multivariable is the term which is correct in the used analysis. Therefore, we changed the term multivariate into multivariable in the the abstract, in table 2 (comment No. 9) as well in the main text of the article.
7.
I would also appreciate if the authors can explain why: “Age and sex were retained in the final multivariate model, irrespective of their p-values in univariate analysis.”
Response to Reviewer 2 comment No. 7:
We put age and sex in the multivariable model despite of their values, because age and sex are considered to be intrinsic factors of the subjects. However, we agree with this reviewer that in the association model it is not necessary to always retain age and sex, especially since the number of participants was limited. In the new multivariable analyses age and sex were retained in the multivariable model only if p
< 0.20. We deleted the sentence
“Age and sex were retained in the final multivariate model, irrespective of their pvalues in univariate analysis.” from the article.
Results:
8.
In table 1 the characteristics of the study are shown.
It gives the impression not many variables were measured. However in the methods section the authors mention that they perfomed a (modified) ISAAC questionnaire, this questionnaire includes far more questions than displayed in table 1. Important to show: How many children had eczema, wheezing etc, also why do the authors not show the prevalences of helminths and protozoa in this table. In addition to the named variables, all important variables (eg potential confounders/effect modifiers or predictors) should be shown in this table.
On the other hand if this really is the only data that was collected, I think the data are not enough to do these analyses. The commonly known counfounders/effectmodifiers or determinants are not measured)
Response to Reviewer 2 comment No. 8:
We agree with the reviewer that the data on which the article was based and written were not transparent for the reader. As the reviewer suggested, we added the prevalence rates of atopic eczema, recurrent wheezing and the specific parasitic infections in Table 1.
We also agree with the reviewer that some potential confounders were not measured in our study. We discussed this topic in the end of the DISCUSSION section of the revised manuscript in the limitations section. This discussion is shown below:
‘Although we performed a multivariable analysis taking into account possible confounders such as age and sex, unmeasured factors may have caused residual confounding. Male gender, low birth weight (< 2,500 g), low gestational age (< 37 weeks), breastfeeding for less than 6 months, congenital heart disease, family history of atopy, asthma, smoking exposure, stove warming, have been identified as
significant risk factors for recurrent wheezing while the presence of pets at home seems to be a protective factor. [56] It is difficult to obtain information on birth weight and gestational age in the Warao population, because documentation on new-borns is not collected consistently and paperwork is scarce. Most women deliver their children at home and do not visit a hospital. There is no documentation available on gestational age because women mostly do not know their pregnancy duration. As virtually all Warao children are breastfed until at least 12 months of age, it is not likely that the lack of information on duration of breastfeeding has influenced our study results. The prevalence of congenital heart disease is unknown. Also, the lack of information on smoking exposure and the presence of pets in the household may have caused residual confounding.’
The ISAAC questionnaire was not used in its total format to investigate recurrent wheezing. Only the question ‘Has your child had episodes of wheezing in the previous 12 months, and if yes how many?’ Subsequently, we defined ‘recurrent wheezing’ in children ≥ 12 months of age when the child suffered from two or more wheezing episodes in the past 12 months. We added information on why we chose this definition of recurrent wheezing to the DISCUSSION section after ‘….The prevalence of recurrent wheezing in our study population was 23%.’
‘’ Similar prevalence rates of recurrent wheezing in children aged 0 to 2 years were observed in urban areas of Brazil and Norway [34, 35], although study definitions regarding the minimal number of wheezing episodes (respectively three in the first year of life and two in the first two years of life) were not identical to our study. In a rural area of Colombia, the prevalence of recurrent wheezing (≥3 episodes) in children aged
24 months was 14%. [36] Definitions of recurrent wheezing in young children used in different studies vary widely. Our definition of recurrent wheezing has been used previously in preschool children. [37, 38] In urban areas with hospitals keeping patient records, questionnaires for recurrent wheezing in infants can be validated by comparing the parental answers to questionnaires with diagnoses made by pediatric respiratory specialists and this has led to the use of such questionnaires in urban health centres in Latin America. [39, 40] The diagnostic value of these questionnaires in rural indigenous populations remains to be seen.
Additionally, an extra table is included in the manuscript to clarify the exact information that was asked to define atopic eczema and the corresponding answers
(table 3: Questionnaire Atopic eczema based on SCORAD Protocol and UKWP criteria/Nottingham protocol) This table is mentioned in the main text in the
METHODS section.
9.
Table 2 should be changed according to which objective is being answered
(see my earlier comment of the objective statement being different in methods and introduction) .
Also in my opinion it is a very confusing table. The authors are trying to put too much information in 1 table. It would be better to make 2 different tables 1 for wheezing and 1 for eczema and then also include the OR (CI) and p value for the univariate analysis.
Response to Reviewer 2 comment No. 9:
We agree with the reviewer that table 2 might be a confusing table and there is a lot of information in that one table. Therefore we splitted up table 2 in table 2a for atopic eczema and table 2b for recurrent wheezing. OR (CI) and p value for univariate analyses were added where missing to clarify the statistic results. Also the term multivariate was changed into multivariable. As malnourishment is one of the objectives, no changes were made in the characteristics column. (see explanation in the response to comment No. 1)
In table 2a and 2b pathogenic protozoan infections and non-pathogenic protozoan infections were fused to protozoan infections, because only 1 subject suffered from a single non-pathogenic protozoan infection and the rest of the subject with a nonpathogenic protozoan infection were also infected with a pathogenic protozoa.
10.“ Children with recurrent wheezing suffered more often from atopic eczema than children without recurrent wheezing, but this was not statistically significant
(32% vs. 16%, p=0.055).
”
This sentence does not make sense to me. Either children suffer more from eczema (and then is is statistically significant, or they do not suffer more from eczema, because its not statistically significant!
Alternatively in this case the authors could argue that its borderline significant!
Response to Reviewer 2 comment No. 10:
We agree with this reviewer that it should be clearly written if an outcome is or is not statistically significant and not suggesting that is a significant outcome while it actually is not. Because it indeed is a borderline significant outcome, we changed this sentence from “Children with recurrent wheezing suffered more often from atopic eczema than children without recurrent wheezing, but this was not statistically significant
(32% vs. 16%, p=0.055).” into ‘’A borderline significant trend towards more atopic eczema in children suffering from recurrent wheezing was observed (32% vs. 16%, p=0.055).’’
Discussion:
11.
There is not clear limitations section. I would like to urge the authors to include a limitations section discussing amongsth others:
1. The way the study population was chosen and what kind of effects that may have on the interpretation of the results
2. The limitations of the a questionnaire (recall bias etc) and the ISAAC questionniare inparticular (e.g definition for wheezing)
Response to Reviewer 2 comment No. 11:
We agree with the reviewer that it would be useful to mention the limitations of this study. Therefore we added 2 alinea’s after ‘…..
Possibly, there is a need for health and educational services on this topic.’
‘In addition to the already mentioned limitation such as the interpretation of the diagnosis of recurrent wheezing, the lack of blood samples or skin-prick tests, there are several other limitations to our study, some of which are related to the challenging logistics of conducting an epidemiological study in an area with a poor infrastructure characterized by low literacy and poor access to health care. Although
we performed a multivariable analysis taking into account possible confounders such as age and sex, unmeasured factors may have caused residual confounding. Male gender, low birth weight (< 2,500 g), low gestational age (< 37 weeks), breastfeeding for less than 6 months, congenital heart disease, family history of atopy, asthma, smoking exposure, stove warming, have been identified as significant risk factors for recurrent wheezing while the presence of pets at home seems to be a protective factor. [56] It is difficult to obtain information on birth weight and gestational age in the Warao population, because documentation on new-borns is not collected consistently and paperwork is scarce. Most women deliver their children at home and do not visit a hospital. There is no documentation available on gestational age because women mostly do not know their pregnancy duration. As virtually all Warao children are breastfed until at least 12 months of age, it is not likely that the lack of information on duration of breastfeeding has influenced our study results. The prevalence of congenital heart disease is unknown. Also, the lack of information on smoking exposure and the presence of pets in the household may have caused residual confounding.
Second, viral infections at the time of the survey may have caused clustering diagnosis of recurrent wheezing per village. Finally the use of a questionnaire in general may have caused recall bias. However a questionnaire is the most reliable instrument in the Warao population because hospital data on atopic diseases are scarce due to the lack of personal medical reco rds.’
- Minor Essential Revisions
12.
Abstract : the objective is written in de methods section. According to the journals guidelines it should be in the introduction section.
Response to Reviewer 2 comment No. 12:
We thank the reviewer for noticing this mistake. After redefining and clarifying the objective (comment No. 1), the objective was written in the introduction section and removed from the methods section.
13.
Discussion: Please check the layout of the 4th paragraph, its not in line with the others paragraphs.
Response to Reviewer 2 comment No. 13:
We have corrected the lay-out of the 4th paragraph. It is now in line with the other paragraphs.
Level of interest: An article whose findings are important to those with closely related research interests
Quality of written English: Acceptable
Statistical review: Yes, and I have assessed the statistics in my report.
Declaration of competing interests:
'I declare that I have no competing interests'