Jan16_-_A5i_Healthcare_Associated_Infections_January_(HCAI).
advertisement
.")
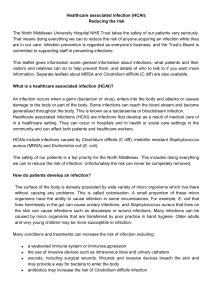
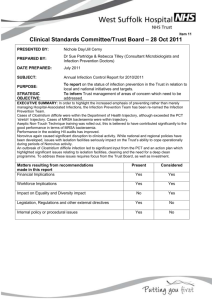
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST Board Paper - Cover Sheet Report Title Healthcare Associated Infections (HCAI) Lead Director Nursing & Patient Services Director Report Author Classification Helen Lamont, Nursing and Patient Services Director Ashley Price, Director of Infection Prevention and Control (DIPC) NHS Unclassified Purpose (Tick one only) Approval Links to Strategic Objectives Links to CQC Fundamental Standard(s) Identified Risk? (If yes, risk reference) Decision Agenda Item A5(i) Information To put patients and carers at the centre of all we do and to provide care of the highest standard in terms of both safety and quality To continue to be recognised as a first-class teaching hospital, counted amongst the top 10 in the country, which promotes a culture of excellence, in all that we do Regulation 12, 15, 20 Yes, specified in Risk Register. Breaches of target Significant outbreaks have financial, reputational and patient safety implications Resource Implications Legal implications and equality and diversity assessment Benefit to patients and the public No additional resource implications Report History This is a regular monthly update to the Board on Healthcare Associated Infections (HCAI) Next steps To read, discuss and approve this paper Failure to effectively control infections may lead to patient harm, litigation against the Trust and loss of reputation. There are no specific equality and diversity implications from this paper. Infection Prevention & Control is fundamental to providence and safe, clean environment for patients, staff and visitors. Agenda item A5(i) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST HEALTHCARE ASSOCIATED INFECTIONS (HCAI) EXECUTIVE SUMMARY This paper summarises the Trust’s position in relation to HCAI and the external targets at the end of December 2015, Month 9 2015/16. There were eight C. difficile cases in December, bringing the total to date to 72 against a year-end target for 2015/16 of 77. 11 cases have been successfully appealed and ten more are being considered. This significantly mitigates the current position. No further cases of MRSA bacteraemia were reported during December 2015. One case from October has now been assigned as Third Party following arbitration. This means that five MRSA cases are currently attributed to the Trust so far in 2015/16 (7 reported minus 2 Third Party). The staff seasonal flu vaccination campaign continues, with uptake of the vaccine among frontline staff at a lower level compared with last year, at 52% this year against 59% last year. A significant amount of work continues to ensure that risks of HCAI are minimised for the benefit of the patients and the Trust including Ward refurbishments on both sites. RECOMMENDATION To (i) note the content of this report (ii) comment accordingly. Mrs Helen Lamont Nursing & Patient Services Director Dr Ashley Price Director of Infection Prevention and Control 14th January 2016 THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST HEALTHCARE ASSOCIATED INFECTIONS (HCAI) 1. INTRODUCTION This paper provides the monthly report to the Board in relation to Healthcare Associated Infections (HCAI) describing the progress against targets for the year, and reporting the Trust’s position for the end of Month 9 (2015/16). The performance is summarised in the Healthcare Associated Infection report at Appendix i. 2. INFECTION UPDATE (i) MRSA Bacteraemia – (Target = Zero Tolerance) No further cases of MRSA were reported during December 2015; the year to date total is seven. One case from October has now been assigned as Third Party following arbitration. This means that five MRSA cases are currently attributed to the Trust so far in 2015/16 (7 reported minus 2 Third Party). This year’s figure of five cases attributed to the Trust compares with three cases to the end of December 2014. A new action plan to support reduction of Staphylococcal infections is in development by the IPC Team. (ii) Clostridium difficile – (Target = 77) The Board is aware that the Trust’s target has been set at 77 cases for the current financial year. In December, eight cases were identified, bringing the year-to-date total to 72 cases, against a cumulative target of no more than 57.8 cases. However, taking into account the 11 appeals, this means 61 cases for the year to date. The graph below demonstrates this year’s performance when compared with the number of cases last year, i.e. in 2014/15 taking into account the successful appeals (65 as a year-end figure in 2014/15, rather than 89). At the same time last year, the Trust had reported 46 cases of C. difficile by the end of December 2014, compared to 61 cases by the end of December 2015. Lessons learned from every case of C. difficile are circulated to clinical staff via the Quarterly HCAI Reports and monthly from the Serious Infection Review Meetings. A renewed focus on antibiotic stewardship is also being led among the medical staff by a Consultant Microbiologist. A new Take Five audit has now been implemented, requiring that five patients have their antibiotics audited on every Ward each month. The IPC Operational Group is reviewing the C. difficile Action Plan. 1 C. diff 2014/15 & 2015/16 (minus succesful appeals) 90 80 70 60 50 40 30 20 10 0 (iii) Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb C. difficile 2014/15 5 9 13 17 21 27 36 40 46 54 64 Mar 73 Trajectory 2015/16 6.4 12.8 19.3 25.7 32.1 38.5 44.9 51.4 57.8 64.2 70.6 77.0 C. difficile 2015/16 2 4 8 15 23 29 38 53 61 MSSA In November 2015 there were nine MSSA bacteraemias attributed to the Trust, bringing the year-to-date total to 51 cases. This compares with 44 cases at the same point in 2014/15. In December 2015 there were eight MSSA bacteraemia attributed to the Trust, bringing the year-to-date total to 59 cases. This is compared with 50 cases at the same point in 2014/15. There are currently no national targets for MSSA but the Trust continues to monitor and report the numbers of MSSA bacteraemia. Root Cause Analysis (RCA) is undertaken in cases where a Consultant Microbiologist feels there are lessons to learn. MSSA was a significant focus at the December 2015 IPC Operational Group meeting and additional work and actions were agreed. A new Action Plan identifies initiatives that have already been implemented over the last year and also outlines future proposed actions. These include changes to the MSSA RCA process. A revised RCA is awaiting approval and, once approved, will be completed in all cases of Trust-acquired MSSA (defined as being identified more than 48 hours after admission). . (iv) E. coli In November there were 20 E. coli bacteraemia attributed to the Trust, bringing the year-to-date total to 112 cases. This is compared with 95 cases at the same point in 2014/15. The numbers will continue to be monitored monthly by IPCC. In December there were 17 E. coli bacteraemia attributed to the Trust, bringing the year-to-date total to 129 cases. This is compared with 101 cases at the same point in 2014/15. The numbers will continue to be monitored monthly by IPCC, who are aware that the number of E. coli cases this year has increased when compared with 2014/15. 2 A working group involving the Continence Team, IPC and staff from Neurosciences and Musculoskeletal Directorates have developed a new document to promote urinary catheter removal. This incorporates the urinary catheter care plan and the HOUDINI framework (this is a protocol which allows the earliest removal of a urinary catheter by Nurses). It is an acronym which reminds Nurses why they should not remove a catheter. This has been approved by The Clinical Records Advisory Committee (CRAC) and Trust-wide rollout is imminent. As with MSSA, there are currently no national targets for E. coli but the Trust continues to monitor and report their numbers. The primary source of each E. coli bacteraemia is recorded by the Microbiology lab for information. 3. ONGOING WORK (i) Communication Mandatory Training In November, the IPC Mandatory Training figure was 87% and in December was 84.58% (this is subject to change as training data is currently being migrated between systems and validation is not yet complete). There has been an overall improvement in this figure since April 2015, when the figure was 69%. (ii) Outbreaks There were three outbreaks of diarrhoea and vomiting during December, one at Freeman Hospital and two at the RVI. Norovirus was isolated from samples from one of the Wards at the RVI, but in the other two Wards no causative organism was identified. There were three C. difficile periods of increased incidence (PIIs) in December, involving two patients being positive on each of the three Wards. Meetings to discuss these cases will take place and ribotyping will identify whether the cases were linked. Patient Services and the IPC Team were involved in managing these outbreaks, which are now closed. (iii) Flu Vaccination Campaign This year’s flu campaign has now ended. It was delivered in partnership with Lloyds Pharmacy. At 24th December 2015, the vaccination uptake was 52% for frontline staff and 45% for all staff, meaning that 4,350 vaccines have been administered to frontline staff so far, and 6,619 in total. At the end of last year’s campaign, the uptake was higher, at 59% for frontline staff but was lower overall at 41%, with 5,184 vaccines delivered to frontline staff and 6,352 in total. 3 The campaign has been successful in the following ways: (iv) Improved and greater accuracy in recording of flu vaccination statistics Good coverage of clinics across the campaign – using the same location for dropin clinics gave a clearer message More vaccines delivered than in previous years Less impact on Newcastle OHS, in terms of nurse cover / phone calls and emails into the department Good marketing campaign simple and consistent message Regular emails as to flu dates and location increased uptake The use of lanyards for Peer vaccinators was positively praised by staff and managers. It allowed staff to easily identify the peer vaccinators. Flu Admissions The Trust is beginning to see a rise in the number of admissions from flu, with eight cases during the last week of December. Point of care testing is being undertaken in Assessment Suite, which yields faster results than sending routine full respiratory samples to the lab. A graph of Trust admissions for flu is below. 4 4. RISKS AND RISK MITIGATION Risks relating to Infection Prevention and Control are monitored and managed on an ongoing basis at the monthly Infection Prevention and Control Committee (IPCC) and the IPC Operational Group, which now meets monthly. As well as the high-profile work to minimise MRSA and C. difficile infections, the IPC Team works hard to ensure that the Trust protects its patients from the threats posed by emerging infections. A renewed focus on MSSA bacteraemia is now underway within the Trust. All key infection risks are recorded on the Trust’s Risk Register, with the person responsible being clearly identified, and the Register being regularly reported at IPCC. 5. SUMMARY The current MRSA bacteraemia and C. difficile position continues to be a high priority in relation to patient safety and the potential financial and reputational risks to the Trust. A significant amount of high profile Trust-wide work continues across all aspects of IPC to protect the patients in the care of the Trust. 6. RECOMMENDATION To (i) note the content of this report (ii) comment accordingly. Mrs Helen Lamont Nursing & Patient Services Director Dr Ashley Price Director of Infection Prevention and Control 14th January 2016 5